

Conservative Management of Spontaneous Coronary Artery Dissection
Key words: angiography, spontaneous coronary artery dissection
A 53-year-old woman with history of hypertension was admitted for acute coronary syndrome without persistent ST-segment elevation. Electrocardiogram was normal, while echocardiogram revealed hypokinesia of the mid-apical anterior wall and interventricular septum with normal ejection fraction.
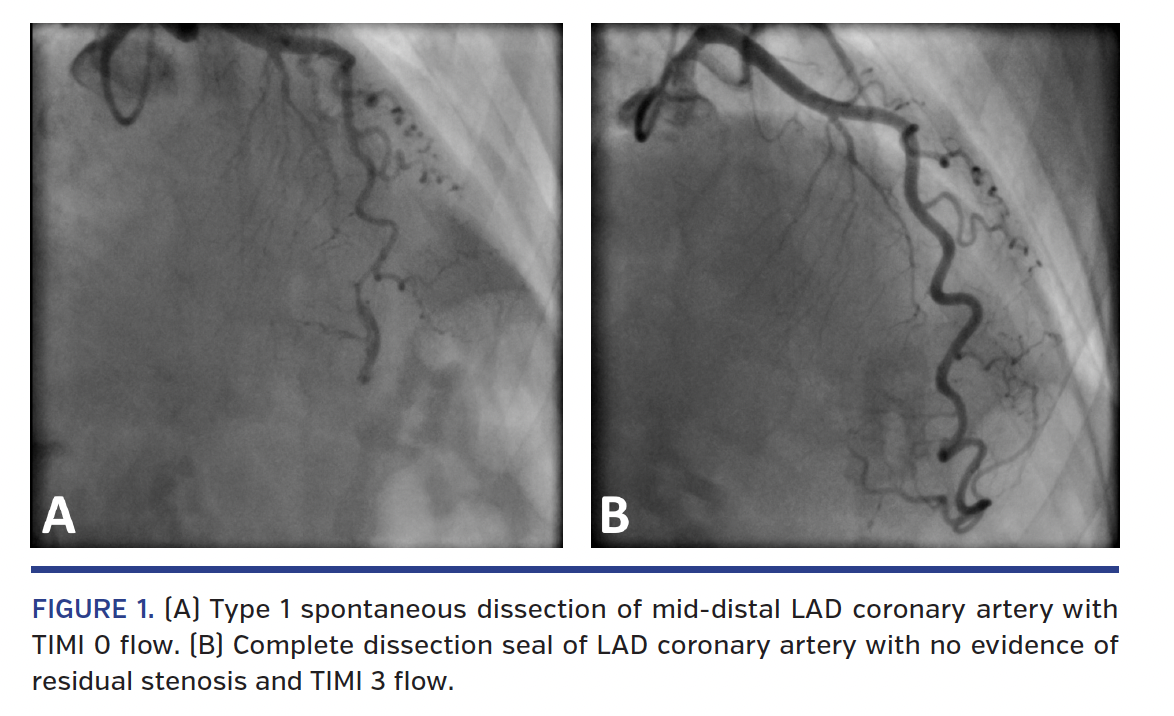
Coronary angiography showed type 1 spontaneous dissection of the mid-distal left anterior descending (LAD) coronary artery with Thrombolysis in Myocardial Infarction (TIMI) 0 flow (Figure 1A; Video 1). In consideration of the clinical stability and the anatomical features (medium caliber and tortuosity of the vessel), we chose a “watchful waiting” strategy based on medical therapy.
After 20 days, we performed a staged coronary angiography, which revealed a complete seal of the dissection in the LAD, with no evidence of residual stenosis and TIMI 3 flow (Figure 1B; Video 2). Echocardiogram showed normal parietal kinetics of the left ventricle.
Spontaneous coronary artery dissection (SCAD) is caused by separation of the vessel wall and hematoma development. This uncommon lesion is typical in young woman, in particular during the peripartum/postpartum period; it’s not related to atherosclerotic disease and can cause different degrees of myocardial ischemia. Based on angiographic appearance, three different types of SCAD are described: type 1 = presence of wall contrast staining with different degrees of obstacle to blood flow; type 2 = long, stenosis-like lesion (>20 mm) due to wall hematoma; and type 3 = focal stenosis-like lesion (<20 mm).
Coronary angiography is the principal diagnostic tool. Intracoronary imaging (intravascular ultrasound or optical coherence tomography) is then performed to confirm the diagnosis, to identify the presence of intimal flap, and to determine the extension of the dissection. Coronary computed tomography scan is another useful and non-invasive exam both in the diagnostic phase and at follow-up.
Revascularization is not the first choice, but it’s necessary in case of ongoing ischemia, left main artery dissection, or hemodynamic instability; complications during percutaneous coronary intervention (PCI) are more frequent compared with routine PCI (dissection extension, stent malapposition, long stent required).
In this case, we confirmed that SCAD often resolves spontaneously, with total angiographic disappearance of the pathological image. The healing period and predisposing factors are not clear. In general, an average period of 35 days from the event is usually sufficient to demonstrate angiographic healing. Medical therapy is mandatory and is based on long-term aspirin and beta-blockers.
View the Accompanying Video Series Here
From the Unità Operativa Complessa di Cardiologia, Ospedale San Francesco, Nuoro, Italy.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted December 23, 2019.
Address for correspondence: Dr Giovanni Lorenzoni, Ospedale San Francesco, Unità Operativa Complessa di Cardiologia, via Mannironi 1, Nuoro, Italy. Email: giovannilorenzoni@alice.it











