

Coronary Artery Disease: Not Always the Case for ST-Elevation Myocardial Infarction
ABSTRACT: We report a case of an acute ST-T elevation myocardial infarction in a middle-aged female with a mechanical mitral valve prosthesis and subtherapeutic INR levels. We performed a primary coronary intervention, using a thromboaspiration catheter. After blood clot aspiration, a TIMI III flow was restored and no residual lesions remained at the site of the occlusion. A transesophageal echo revealed a movable thrombus over the mechanical mitral valve prosthesis and patient underwent subsequent mitral valve replacement. Embolic myocardial infarction remains underdiagnosed. A high level of suspicion and the quest of the source of embolus are crucial.
J INVASIVE CARDIOL 2012;24(7):E142-E144
Key words: acute coronary syndrome, coronary embolism, aspiration catheter
____________________________________________________
It is indisputable that plaque rupture is the most common cause of acute myocardial infarction (MI).1 Nevertheless, coronary embolism, a cause of acute MI that is less rare than previously thought, is a clinical entity that needs to be considered in every case of myocardial infarction (MI) in the absence of significant coronary artery disease (CAD). This case report describes a case of acute MI due to coronary embolism from a thrombosed prosthetic mitral valve, successfully managed by thrombus removal using aspiration catheter.
Case Report. A 62-year-old woman presented at the emergency department of our hospital, complaining of acute onset of severe chest pain radiating down her left arm. Her symptoms had begun 2 hours earlier. Her past medical history was notable for rheumatic heart disease, paroxysmal atrial fibrillation, stroke, hypothyroidism, and prosthetic mitral valve replacement a year before.
 She had no history of CAD, diabetes mellitus, hyperlipidemia, hypertension, and she was a non-smoker. A coronary angiography performed in our institution a year ago, just before her valve replacement, was unremarkable for CAD, showing completely normal coronary arteries. Her current medication included coumadin, digoxin, metoprolol, thyroxine, and omeprazole. On physical examination, the patient’s blood pressure was 100/70 mm Hg and her pulse rate was 80 bpm, without evidence of elevated jugular pressure. No peripheral edema or rales were detected on chest auscultation. Electrocardiography at presentation revealed sinus rhythm with right bundle branch block and ST-T segment elevation in leads V2-V6 (Figure 1).
She had no history of CAD, diabetes mellitus, hyperlipidemia, hypertension, and she was a non-smoker. A coronary angiography performed in our institution a year ago, just before her valve replacement, was unremarkable for CAD, showing completely normal coronary arteries. Her current medication included coumadin, digoxin, metoprolol, thyroxine, and omeprazole. On physical examination, the patient’s blood pressure was 100/70 mm Hg and her pulse rate was 80 bpm, without evidence of elevated jugular pressure. No peripheral edema or rales were detected on chest auscultation. Electrocardiography at presentation revealed sinus rhythm with right bundle branch block and ST-T segment elevation in leads V2-V6 (Figure 1).
 Blood count chemistries, cholesterol profile, and myocardial injury enzymes were within normal limits. INR was at a subtherapeutic level of 1.1.
Blood count chemistries, cholesterol profile, and myocardial injury enzymes were within normal limits. INR was at a subtherapeutic level of 1.1.
Therapy with 325 mg aspirin, loading 600 mg clopidogrel, and 5.000 IU unfractionated heparin was started, and the patient was immediately transferred to the catheterization laboratory. Coronary angiography showed total occlusion of mid left anterior descending (LAD) coronary artery, with thrombolysis in acute myocardial infarction (TIMI) 0 flow as shown in Figure 2. After vessel 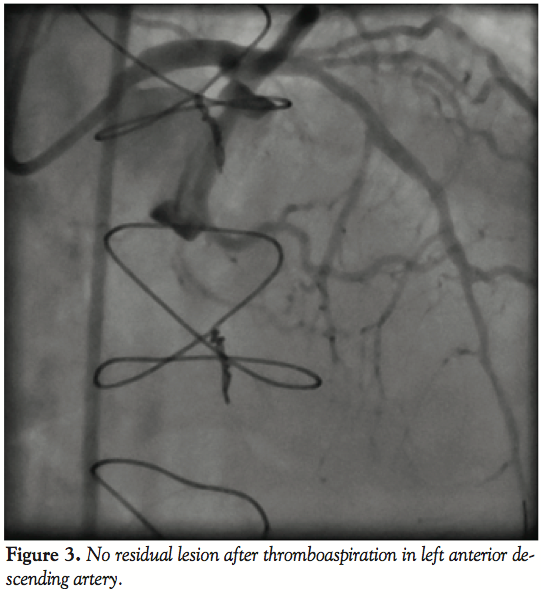 wiring through an Extra Back Up 6 Fr guiding catheter (Medtronic), an aspiration catheter (6 Fr Export AP; Medtronic) was inserted. The blood clot was successfully aspirated with immediate relief of pain and resolution of ST segment elevation. TIMI III flow was restored with no residual lesions at the site of thrombus or the distal parts of the vessel (Figure 3). A decision was made not to deploy a balloon or a stent in the affected area. Left circumflex and right coronary arteries were normal, as detected 1 year before.
wiring through an Extra Back Up 6 Fr guiding catheter (Medtronic), an aspiration catheter (6 Fr Export AP; Medtronic) was inserted. The blood clot was successfully aspirated with immediate relief of pain and resolution of ST segment elevation. TIMI III flow was restored with no residual lesions at the site of thrombus or the distal parts of the vessel (Figure 3). A decision was made not to deploy a balloon or a stent in the affected area. Left circumflex and right coronary arteries were normal, as detected 1 year before.
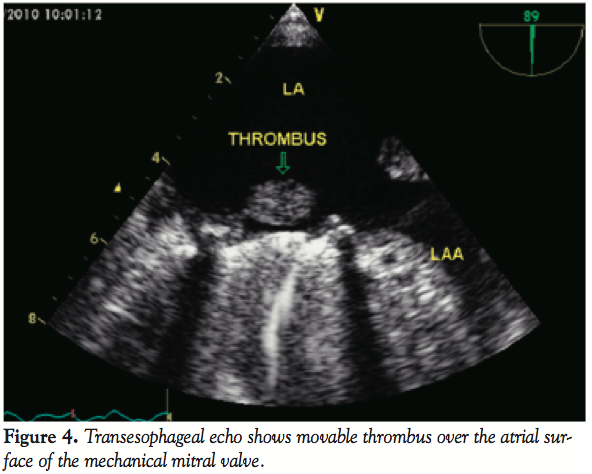 A transthoracic echo followed by transesophageal echo obtained after the coronary procedure in the coronary care unit showed a 2.5 cm visible movable thrombus over the atrial surface of the mechanical mitral valve (Figure 4), and almost normal systolic left ventricular function with mild apical hypokinesia. Levels of troponin T and CK were actually raised up to 4.8 ng/mL and 900 IU/L, respectively. The patient was commenced on heparin continuous IV infusion, and a cardiothoracic reintervention was performed 1 week later, confirming the existence of a voluminous thrombus over the prosthetic mitral valve and proceeding in a replacement of the thrombosed valve. Although surgery was technically considered high risk due to a recent history of MI, considerable valve thrombus burden discouraged other non-surgical approaches. Actually, 6 months later, the patient is asymptomatic with normally functioning mitral valve prosthesis.
A transthoracic echo followed by transesophageal echo obtained after the coronary procedure in the coronary care unit showed a 2.5 cm visible movable thrombus over the atrial surface of the mechanical mitral valve (Figure 4), and almost normal systolic left ventricular function with mild apical hypokinesia. Levels of troponin T and CK were actually raised up to 4.8 ng/mL and 900 IU/L, respectively. The patient was commenced on heparin continuous IV infusion, and a cardiothoracic reintervention was performed 1 week later, confirming the existence of a voluminous thrombus over the prosthetic mitral valve and proceeding in a replacement of the thrombosed valve. Although surgery was technically considered high risk due to a recent history of MI, considerable valve thrombus burden discouraged other non-surgical approaches. Actually, 6 months later, the patient is asymptomatic with normally functioning mitral valve prosthesis.
Discussion. The clinical diagnosis of coronary embolism is often challenging and even more rarely definite. Its incidence varies from previous reports several years ago, and comes up to 13%.2 The suspicion of coronary embolic event arises from the coexistence of angiographic evidence of occlusion or thrombus, a source of embolus and the syndrome of acute MI with normal coronary arteries.
Factors predisposing to coronary embolism include: non-infected valvular heart disease, infective endocarditis, prosthetic heart valves, and atrial fibrillation. Patients prone to the development of mural thrombus in the left ventricle due to dilated or ischemic cardiomyopathy are at increased risk for coronary embolism. Cardiac catheterization is the major cause of iatrogenic coronary embolism. Rare causes include neoplastic, bone marrow, paradoxical, and air emboli and fragments of suture material following open-heart surgery. The consequences of the embolic event depend upon the size of the embolus and the size of the affected vessel or the territory of myocardium the affected vessel supplies.3 The coronary arteries of patients with embolic acute MI are often normal without atherosclerotic lesions.
Coronary embolism usually affects the left coronary system, particularly the LAD. Pesendorfer et al,4 using an in vitro model, found that embolism happens due to active suction of blood/thrombus into the coronary artery at the onset of diastole, at the level of aortic valve. Since the left coronary artery is larger than the right one, a greater proportion of flow is received by the left one, hence, more emboli. Because of the direct downward course of the LAD, it may be more liable to embolization than the left circumflex artery, which is at a right angle to the main trunk.5 In our case, the patient had a totally occluded LAD, and we confirmed the mitral valve as the source of embolus (Figure 4). In all previously reported cases,6-8 a source of embolus was not evident, making the diagnosis of embolic acute MI rather presumptive.
There is no consensus and very little information is available about the best possible treatment of acute MI due to coronary embolism. In previously published cases, many attempts for recanalization have been reported using: intracoronary thrombolysis, intracoronary GP IIb/IIIa antagonists, aspiration catheter and ballooning, and/or stenting with varying success rates.6-8 A really challenging case has been reported by Aslam et al,9 where there was a visible thrombus in the LAD while TIMI III flow existed. The authors decided to treat the patient with intracoronary thrombolysis because of the potential risk of thrombus dislodgement and distal embolization, causing complete occlusion of a distal branch with further damage. The final result was suboptimal, since 24 hours later, there was no thrombus resolution, and nuclear imaging 4 weeks later showed a large area of anterolateral and anteroapical infarction without an ischemic or viable myocardium.
In our case, the patient had TIMI 0 flow along LAD, and we decided to aspirate thrombus using an aspiration catheter. We supported the diagnosis of coronary embolism because of the visible thrombus over mitral valve in the transthoracic echocardiogram and the normal coronary angiography of the patient the previous year, along with the excellent result after thrombus aspiration and TIMI III flow restoration. In another reported case,10 using an aspiration catheter had an unfavorable result and using a balloon following stenting of the lesion was inevitable. Also in this case, the diagnosis of embolism was unclear. An interesting case of paradoxical embolization of the LAD was reported a year earlier.11 The clot successfully aspirated, felt to be of venous origin on histologic analysis. Nevertheless, as previously noted in the case of Kotooka et al,10 as in this case, there was no clinical or radiological confirmation of deep venous thrombosis as the source of embolus.
We did not perform IVUS in the present case, which would possibly verify the lack of atherosclerotic evidence in our patient’s vessel, as well as histologic examination of the aspiration material. Both may be limitations of the approach used for the present case. Nevertheless, the embolic source solely demonstrated the TIMI III flow restoration after aspiration without sign of any atherosclerotic lesion; the lack of predisposing risk factors for CAD of our patient; and the identical angiographic appearance of the patient’s coronary arteries 1 year before, which is why we support that coronary embolism was the first diagnosis applied for this patient.
The patient proceeded to prosthetic mitral valve replacement 2 days later. She is very active and continues to do well after 1 year.
Conclusion
Although embolic MI is not so rare a clinical entity, it remains underdiagnosed. A high level of suspicion and the quest of the source of embolus are crucial. Aggressive anticoagulation in so-needed high-risk patients according to AHA/ACC guidelines is an important preventive measure.
References
- Fuster V, Badimon L., Badimon JJ, Chesebro JH. The pathogenesis of coronary artery disease and the acute coronary syndromes. N Engl J Med. 1992;326(4):242-250.
- Prizel KR, Hutchins GM, Bulkley BH. Coronary artery embolism and myocardial infarction. Ann Intern Med. 1978;88(2):155-161.
- Charles RG, Epstein EJ, Holt S, Coulshed N. Coronary embolism in valvular heart disease. Q J Med. 1982;51(202):147-161.
- Pesendorfer F. The mechanism of coronary embolism [in German]. Beitr Gerichtl Med. 1969;26:39-43.
- Charles RG, Epstein EJ. Diagnosis of coronary embolism: a review. J R Soc Med. 1983;76(10):863-869.
- Karabinos I, Kranidis A, Spanos V. Acute myocardial infarction presumably embolic, in a patient with a mechanical aortic valve: a rare cause of non-atherosclerotic coronary artery occlusion. Hosp Chron. 2010;5(1):1-5.
- Atmaca Y, Ozdol C, Erol C. Coronary embolism in a patient with mitral valve prosthesis: successful management with tirofiban and half-dose tissue-type plasminogen activator. Chin Med J (Engl). 2007;120(24):2321-2322.
- Sial JA, Ferman MT, Saghir T, Rasool SI. Coronary embolism causing acute myocardial infarction in a patient with mitral valve prosthesis: successful management with angioplasty. J Pak Med Assoc. 2009;59(6):409-411.
- Aslam MS, Sanghi V, Hersh S, Lakier JB. Coronary artery saddle embolus and myocardial infarction in a patient with prosthetic mitral valve. Catheter Cardiovasc Interv. 2002;57(3):367-370.
- Kotooka N, Otsuka Y, Yasuda S, Morii I, Kawamura A, Miyazaki S. Three cases of acute myocardial infarction due to coronary embolism: treatment using a thrombus aspiration device. Jpn Heart J. 2004;45(5):861-866.
- Gulati A, Chan C, Rakhit R. Acute myocardial infarction due to paradoxical embolism: successful catheter aspiration and histological correlation. Heart. 2010;96(6):485-486.
____________________________________________________
From the Cardiac Catheterization Laboratory, Thriassio General Hospital of Elefsis, Athens, Greece.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted December 13, 2011, provisional acceptance given February 7, 2012, final version accepted February 27, 2012.
Address for correspondence: Dr. Anna Dagre, 23, Ikarias Str, 14578, Ekali, Athens, Greece. Email: annadagre@hotmail.com











