

Coronary to Bronchial Artery Fistula: Are We Treating It Right?
ABSTRACT: Fistulas between coronary artery and bronchial artery may be present from birth, with few hemodynamic consequences, and may remain closed due to similarity of the filling pressures at these 2 sites.1 They can also be secondary to pulmonary artery occlusive disease or chronic pulmonary inflammation.2,3 These pulmonary changes may cause a dilation of the fistula and make it functional, causing angina pectoris by coronary steal syndrome, which is the most common symptom. The presentation may also be composed of episodes of hemoptysis, heart failure, and infective endocarditis. However, most patients remain asymptomatic. The ones that need treatment may not have a good response to the medical management, requiring an intervention. This can be done using embolization coils, stents grafts, and performing surgical ligation of the fistulas.2-4
J INVASIVE CARDIOL 2012;24(11):E303-E304
___________________________________________________
 Case Report. A 62-year-old man was admitted with angina on moderate exertion and dyspnea. He had a history of hypertension, diabetes, and smoking and was on aspirin, atenolol, glibenclamide, and alpha-methyldopa. Due to pulmonary symptoms, we performed chest computed tomography (CT), bronchoscopy, and lung biopsy, which revealed bronchiectasis, interstitial fibrosis, and chronic bronchitis in the right lung. During the investigation echocardiography showed left ventricular diastolic dysfunction grade 1, ejection fraction of 65%, and mild mitral regurgitation. Exercise testing revealed ST segment depression of 1.5 mm and typical chest pain in the fourth minute of Bruce protocol. No significant changes were shown during 99mTc-sestamibi scintigraphy. Coronary CT did not reveal any coronary luminal reduction. Nevertheless, it demonstrated a retro-aortic connection between the coronary artery and
Case Report. A 62-year-old man was admitted with angina on moderate exertion and dyspnea. He had a history of hypertension, diabetes, and smoking and was on aspirin, atenolol, glibenclamide, and alpha-methyldopa. Due to pulmonary symptoms, we performed chest computed tomography (CT), bronchoscopy, and lung biopsy, which revealed bronchiectasis, interstitial fibrosis, and chronic bronchitis in the right lung. During the investigation echocardiography showed left ventricular diastolic dysfunction grade 1, ejection fraction of 65%, and mild mitral regurgitation. Exercise testing revealed ST segment depression of 1.5 mm and typical chest pain in the fourth minute of Bruce protocol. No significant changes were shown during 99mTc-sestamibi scintigraphy. Coronary CT did not reveal any coronary luminal reduction. Nevertheless, it demonstrated a retro-aortic connection between the coronary artery and 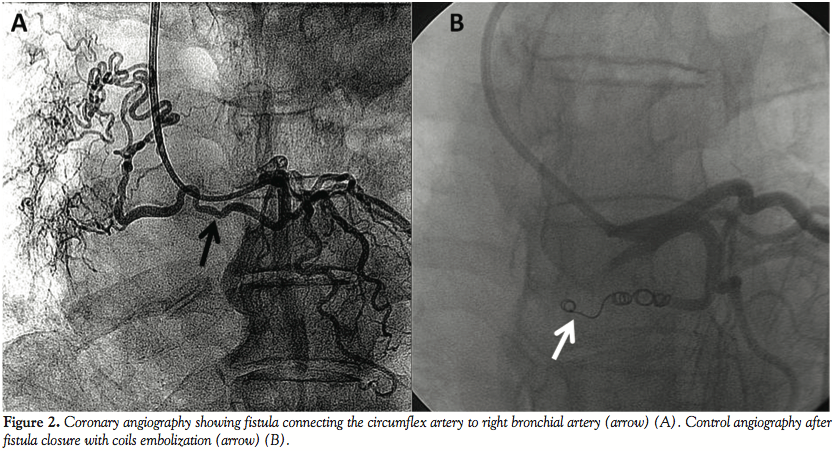 the pulmonary vasculature (Figure 1). Therefore, we performed coronary angiography, which depicted no coronary artery disease. However, it identified a fistula between the circumflex artery and right bronchial artery (Figure 2A). The fistula was successfully occluded at its proximal third with 3 coils (3 mm/3.3 mm + 4 mm/3.7 mm+ 5 mm/5.5 mm) (Figure 2B). The patient remained stable, with normal ECG and cardiac enzymes after 48 hours. At 1-month follow-up, the patient continued with the same complaint of angina. A new coronary angiography was performed. It showed no stenosis or induced coronary spasm and total occlusion of the fistula at its proximal third.
the pulmonary vasculature (Figure 1). Therefore, we performed coronary angiography, which depicted no coronary artery disease. However, it identified a fistula between the circumflex artery and right bronchial artery (Figure 2A). The fistula was successfully occluded at its proximal third with 3 coils (3 mm/3.3 mm + 4 mm/3.7 mm+ 5 mm/5.5 mm) (Figure 2B). The patient remained stable, with normal ECG and cardiac enzymes after 48 hours. At 1-month follow-up, the patient continued with the same complaint of angina. A new coronary angiography was performed. It showed no stenosis or induced coronary spasm and total occlusion of the fistula at its proximal third.
Discussion. Coronary-bronchial fistula is a rare finding. Its incidence varies from 0.08% to 0.61%.3,5 However, the real frequency of this disease is probably underestimated, especially in patients with an adjacent pulmonary pathology. Bronchiectasis is considered the most common cause of coronary-bronchial fistula.3 The pulmonary vascular destruction associated to peripheral inflammation causes distal hypoxia and decreases the pulmonary arterial flow. Other causes include Takayasu arteritis; pulmonary thromboembolism; pulmonary artery tumor; chronic bronchitis; Tetralogy of Fallot with pulmonary atresia; hypoplasia of the pulmonary artery; supravalvular aortic stenosis; and pulmonary tuberculosis.6 Fistulas usually originate from the circumflex coronary artery by the left atrial branch.6 This disorder may induce coronary steal syndrome, responsible for episodes of angina and even myocardial infarction. The blood shunt from the left atrial artery may lead to atrial ischemia, facilitating atrial fibrillation, which can become permanent even after fistula closure.3 Besides angiography, computed tomography can also be a reliable diagnostic method for noninvasive detection of this disorder.5 Although there is no prospective randomized trial comparing surgical and percutaneous outcomes, the latter seems to be less aggressive and as effective as surgical ligation.6 However, in cases of severe coronary artery disease, coronary artery bypass graft with ligation of the fistula may be a better treatment.5 The percutaneous treatment may be performed with coils made of platinum or plastic polymer. However, one should be aware that the latter may cause bronchial necrosis if distal embolization occurs.3
The interesting fact of this case is that even though the patient had typical coronary symptoms, a clearly positive exercise test, and an acceptable cause of these changes, the fistula closure did not provide any relief of the symptoms. This raises concern about the correct indications of fistula closure as well as which tests or procedures should be performed to determine if the fistula is the real cause of the symptoms. According to the present case, we suggest that myocardial scintigraphy should be requested and, above all, should be valued with patients like this. Even though there is a belief that the fistula dilates over time with progressively increasing risk of thrombosis, endocarditis, or rupture, in our opinion an asymptomatic patient with a small fistula should be treated conservatively. If symptoms are present, extensive investigation should be performed to avoid an unnecessary treatment. A randomized prospective trial could provide us more information about this interesting disorder.
References
- Moberg A. Anastomoses between extracardiac vessels and coronary arteries. I. Via bronchial arteries. Post-mortem angiographic studies in adults and newborn infants. Acta Radiol Diagn (Stockh). 1967;6(2):177-192.
- Jim MH, Lee SW, Lam L. Localized bronchiectasis is a definite association of coronary-bronchial artery fistula. J Invasive Cardiol. 2003;15(9):554-556.
- Jarry G, Bruaire JP, Commeau P, et al. Coronary-to-bronchial artery communication: report of two patients successfully treated by embolization. Cardiovasc Intervent Radiol. 1999;22(3):251-254.
- St John Sutton MG, Miller GA, Kerr IH, Traill TA. Coronary artery steal via large coronary artery to bronchial artery anastomosis successfully treated by operation. Br Heart J. 1980;44(4):460-463.
- Lee ST, Kim SY, Hur G, et al. Coronary-to-bronchial artery fistula: demonstration by 64-multidetector computed tomography with retrospective electrocardiogram-gated reconstructions. J Comput Assist Tomogr. 2008;32(3):444-447.
- Matsunaga N, Hayashi K, Sakamoto I, et al. Coronary-to-pulmonary artery shunts via the bronchial artery: analysis of cineangiographic studies. Radiology. 1993;186(3):877-882.
______________________________________________
From Instituto do Coração do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo – Incor/HCFMUSP.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 11, 2012, provisional acceptance given June 28, 2012, final version accepted July 2, 2012.
Address for correspondence: Luiz Fernando Ybarra MD, Rua Peixoto Gomide, 1653, apt 142, São Paulo-SP, Brazil, 01409-003. Email: lfybarra@gmail.com











