

Coronary Computed Tomography Angiography Indicates Complexity of Percutaneous Coronary Interventions
Abstract: Background. Coronary computed tomography angiography (CCTA) provides information regarding lesion morphology and three-dimensional coronary anatomy incremental to coronary angiography. We addressed the question whether preprocedural CCTA bears potential for guiding percutaneous coronary interventions (PCI). Methods and Results. Sixty-six coronary lesions attempted with PCI within 6 months of preprocedural CCTA were retrospectively assessed. Lesion parameters from unenhanced computed tomography (CT) for calcium scoring and CCTA were analyzed and compared with PCI complexity. Complex PCI was defined as use of buddy wire, kissing balloon, necessity of high pressure balloons, or rotablator. Complex PCIs were observed in 32 interventions (48%). Median Agatston score and Hounsfield Units were higher in lesions with complex as compared to those with non-complex interventions with 130 (interquartile range, 23-276) vs 29 (0-158; P=.01), and 493 (245-631) vs 341 (68-520 Hounsfield Units; P=.04), respectively. Median local plaque volume and plaque mass were higher in complex PCI with 17 (2-39) vs 5 (0-19.5 mm3; P=.007), and 48 (15-99) vs. 16 (1.5-63 mg hydroxyapatite/mm3; P=.03), respectively. Lesions leading to complex PCI were longer [1.8 (1.2-2.8) vs 1.3 (0.8-1.7) cm; P=.03], and had a higher rate of calcified plaques (23% vs 3%; P=.03). There was a significant correlation between CCTA- and angiography-derived local SYNTAX Scores (P<.001); the CCTA-derived score seems to be predictive for failed and complex PCI (area under the curve = 0.75 ± 0.13 and 0.66 ± 0.08, respectively). Conclusions. Preprocedural lesion assessment by CCTA indicates complexity of PCI. In patients with suspected complex coronary anatomy, prior CCTA adds important information for planning PCI.
J INVASIVE CARDIOL 2012;24(5):196-201
Key words: coronary intervention, complications, ultrafast CT
____________________________________________
Percutaneous coronary intervention (PCI) nowadays has become standard of care in symptomatic coronary artery disease (CAD) with suitable anatomy, and it is increasingly used in the treatment of complex CAD.1 However, overall lesion complexity impacts in many respects on the procedure itself, as well as on short- and long-term outcome.2,3 Lesion localization, severe calcifications, and vessel tortuosity may challenge the skills of the operator and increase the risk of procedural complications such as coronary artery dissection, perforation, and plaque shift. Hence, comprehensive preprocedural patient evaluation and lesion characterization are fundamental. In recent years, coronary computed tomography angiography (CCTA) has become a promising non-invasive imaging technique, mostly applied prior to coronary angiography. Although preferentially used in patients with low to intermediate probability of CAD to avoid invasive diagnostics for exclusion of the condition in these patients,4 CCTA provides nevertheless important incremental information to coronary angiography with regard to lesion characterization and three-dimensional coronary anatomy.
The angiographic SYNTAX score, developed to determine the complexity of CAD, is a comprehensive lesion-based scoring system, comprising the number of lesions, location, and complexity such as tortuosity, length, and calcification.1,3,5 An individual score is calculated for each significant lesion, and the total SYNTAX score is derived by adding all separate scorings together. The SYNTAX score has become an easily applicable angiographic scoring tool to assist in patient selection for interventional or surgical revascularization and risk stratification with respect to major adverse events following PCI.2,3
So far, the potential incremental information of CCTA for guiding PCI has been studied only for chronic total occlusions (CTO), although suggestions for a broader use have been made.6-8 Indeed, lesion length >15 mm, target vessel tortuosity, and severe calcification assessed by CCTA and unenhanced computed tomography (CT) have been identified as independent predictors of procedural failure for CTO.9-15
Thus, we hypothesized that preprocedural lesion characterization by CCTA and unenhanced CT might contribute to predict PCI complexity in extensive and complex CAD. To support this hypothesis and to provide the rationale for future research, we analyzed retrospectively the correlation between specific CCTA parameters and indicators of complex PCI, an operational study definition for the purpose of this study, comprising use of buddy wire, kissing balloon, necessity of high-pressure balloon, or use of rotablator due to heavy calcifications. Furthermore, we compared the lesion-related SYNTAX scores obtained by CCTA with those obtained by coronary angiography. Preprocedural lesion characterization by CCTA might provide important additional information on lesion complexity prior to invasive diagnostics, and thus may allow for early stratification of the most appropriate PCI strategy.
Methods
Patients. The study population comprises 39 patients in whom 49 PCIs were performed for 66 single coronary lesions within 6 months of preprocedural CCTA. The study population was recruited out of 326 consecutive patients who underwent both unenhanced CT and CCTA for any clinical or scientific purposes at our institution. CT and CCTA are performed at our institution in patients with low to intermediate probability of significant CAD. Thus, the majority of patients with unenhanced CT and CCTA did not have subsequent coronary interventions. Due to the retrospective design of this study, the patient selection was completely investigator-independent. Although the PCI operators were entitled to access the CCTA data, no single cardiac catheterization report in the study group keeps record of having made use of them periprocedurally. Routine assessment of cardiac biomarkers was performed the day following the procedure. In-hospital major adverse cardiac events (MACE) including death, myocardial infarction, and target lesion revascularization were assessed.16
CT data acquisition. All CT examinations were performed using a LightSpeed VCT XT scanner (GE Healthcare) with a protocol for prospective triggering (SnapShot Pulse, GE Healthcare). Scanning parameters for the unenhanced calcium scoring scan were: 120 kV tube voltage, 200 mA tube current, 0.35 s rotation time, and 2.5 mm slice thickness. For the enhanced CCTA study, all patients received a single dose of 2.5 mg isosorbiddinitrate sublingual (Isoket; Schwarz Pharma) 2 minutes prior to the scan. Intravenous metoprolol (5-20 mg) (Beloc; AstraZeneca) was administered if necessary to achieve the target heart rate (HR) <65 bpm. Then, 80 mL of iodixanol (Visipaque 320, 320 mg/mL; GE Healthcare) were injected through an 18-gauge catheter into an antecubital vein at a flow rate of 5 mL/s followed by 50 mL saline solution. Bolus tracking was performed with a region of interest (ROI) placed into the ascending aorta, and image acquisition was started with a delay of 4 s after reaching a threshold of 120 Hounsfield Units. Body mass index (BMI), adapted tube voltage (100 kV: BMI <25 kg/m2; 120 kV: BMI ≥25 kg/m2), and tube current (450 mA: BMI <22.5 kg/m2; 500 mA: BMI 22.5-25 kg/m2; 550 mA: BMI 25-27.5 kg/m2; 600 mA: BMI 27.5-30 kg/m2; 650 mA: BMI >30 kg/m2) were applied. CCTA images were acquired using prospective triggering at 75% of the RR-interval without padding. Further scanning parameters were: 0.35 s rotation time and 64 × 0.625 mm slice acquisition. Images were reconstructed with a slice thickness of 0.6 mm, using a standard medium-soft tissue convolution kernel. All images were transferred to an external workstation (AW 4.4; GE Healthcare) for further evaluation. The effective radiation dose of each CT scan was calculated as the product of the dose-length product (DLP) and a conversion coefficient for the chest (k = 0.017 mSv/mGy cm).
CT data analysis. All unenhanced CT calcium scoring images were analyzed using dedicated software (SmartScore; GE Healthcare). Coronary artery calcium scores were separately obtained for each of the main epicardial coronary arteries: the left anterior descending artery (LAD), including the left main artery (LMA), the left circumflex artery (LCX), and the right coronary artery (RCA).
Characterization of the 66 single lesions for which PCI was attempted was retrospectively performed using CCTA and unenhanced CT parameters. Lesion morphology was assessed from CCTA, coronary artery plaques were divided into mixed, soft, and calcified plaques according to the degree of calcification as previously shown.17 The following parameters were analyzed from unenhanced CT: local plaque density (Hounsfield Units), Agatston score (segmental, per lesion), local plaque volume (mm3), and local plaque mass (mg hydroxyapatite/mm3). Local plaque length (mm) and local SYNTAX scores of each lesion were calculated from CCTA using axial source images, multiplanar reformations and curved reformations with the SYNTAX score algorithm as previously described and available on the SYNTAX score website (www.syntaxscore.com).5 The SYNTAX score comprises lesion location, vessel tortuosity, lesion anatomy, lesion length (>20 mm), plaque calcification, total occlusion, and thrombosis, as well as diffuse CAD.5
The investigators assessing CCTA and unenhanced CT were blinded to baseline characteristics, angiographic SYNTAX scores, angiographic and procedural data, as well as patient symptoms and outcomes. SYNTAX scores and calcium scores were analyzed by independent investigators.
Analysis of coronary angiography and PCI. All PCI procedures were performed during the routine interventional program at the Andreas Gruentzig catheterization laboratories. Complications were recorded according to the American Heart Association/American College of Cardiology guidelines for PCI.16,18-20 The complexity of PCI was retrospectively assessed. Complex PCI was defined as use of buddy wire, kissing balloon, necessity of high-pressure balloon pre- or postdilatation, or use of rotablator due to calcifications.14 Dissection, perforation, and plaque shift were summarized as procedure-related complications.21 It is important to emphasize that these procedural characteristics were chosen operationally for the purpose of this study as surrogate markers for information that could be derived from preceding CCTA, eg, high-pressure balloon inflation might be performed regularly in some institutions, but in this cohort, it is only applied in calcified lesions and in cases of angiographically or IVUS-documented underexpansion, and thus again it reflects complex anatomy. Since these procedure-related complications are successfully managed in the majority of cases in contemporary interventional cardiology, they usually do not figure among MACE. Failed PCI was defined as the inability to achieve an at least satisfactory PCI result, defined as <20% residual stenosis and TIMI 3 flow.16,18 CCTA and unenhanced CT parameters of significant coronary lesions with complex and non-complex PCI were compared. Local SYNTAX scores of each lesion were obtained from coronary angiography by independent investigators using the SYNTAX score algorithm as previously described and available on the SYNTAX score website (www.syntaxscore.com).5 The correlation between the score obtained by CCTA and the one obtained by coronary angiography, as well as the potential of the CCTA-derived SYNTAX score to predict failed and complex PCI, were assessed.
The investigators assessing coronary angiography and complexity of PCI were blinded to the CCTA and unenhanced CT parameters of the patients.
Statistical analysis. Continuous variables are presented as medians and interquartile ranges. Categorical variables are given as frequencies and percentages. Continuous variables were tested for differences with the Wilcoxon signed-rank test. Categorical variables were tested by the Pearson’s χ2 test. Correlation between two variables was specified by the Spearman’s rank correlation coefficient. A two-sided P-value of <.05 was considered statistically significant. All statistical analyses were performed with the use of SAS version 9.1 (SAS Institute Inc).
Results
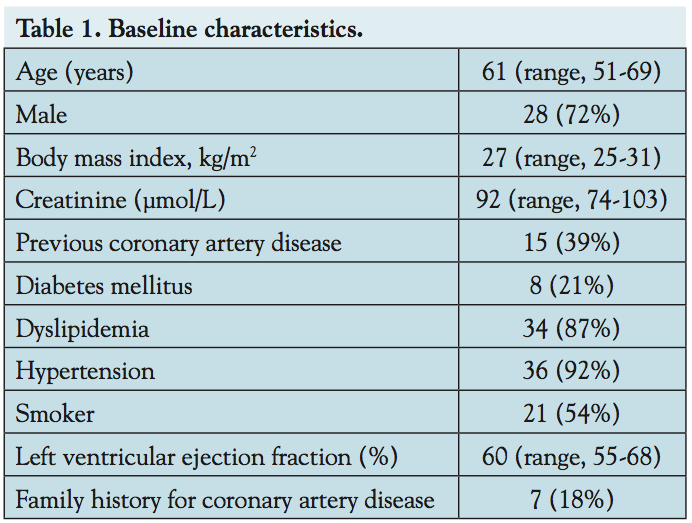 Baseline characteristics. Median age of the patients (72% male) was 61 years (range, 51-69 years). Risk factors for CAD were frequently observed: 21% of the patients suffered from diabetes, 87% had dyslipidemia, and 92% had hypertension. A total of 54% were smoking or had a history of tobacco use. Baseline characteristics are shown in Table 1.
Baseline characteristics. Median age of the patients (72% male) was 61 years (range, 51-69 years). Risk factors for CAD were frequently observed: 21% of the patients suffered from diabetes, 87% had dyslipidemia, and 92% had hypertension. A total of 54% were smoking or had a history of tobacco use. Baseline characteristics are shown in Table 1.
Due to the Zurich University Hospital’s role as a tertiary referral center, the study cohort included a high proportion of patients with previously known CAD (39%), a third of interventions were performed in patients with previous interventional (31%) or surgical coronary revascularizations (3%). Two- and three-vessel disease together were diagnosed in 66% of the patients.
Procedural characteristics. Sixty-six lesions were attempted; 35 (53%) were LAD, 14 (21%) LCX, and 17 (26%) were RCA lesions.
Complex PCI as specifically defined above was reported in 32 interventions (48%). Buddy wire was used in 8 interventions (12%), kissing balloon in 6 (9%), high-pressure balloon in 18 (27%), and rotablator in 5 (8%). Attempted PCI failed in 6 interventions (9%). Procedure-related complications were observed in 7 interventions (11%) with dissection in 5 (8%), and perforation and plaque shift in 1 patient each (2%). These procedural complications were successfully managed without any adverse consequences for the patients. Median fluoroscopy time was 16.3 minutes (range, 8.2-22.4 minutes), and median contrast volume 250 mL (range, 180-323 mL).
Overall in-hospital MACE occurred in 4% (1 periprocedural myocardial infarction, 1 target lesion revascularization) of interventions in accordance with current standards in interventional cardiology.
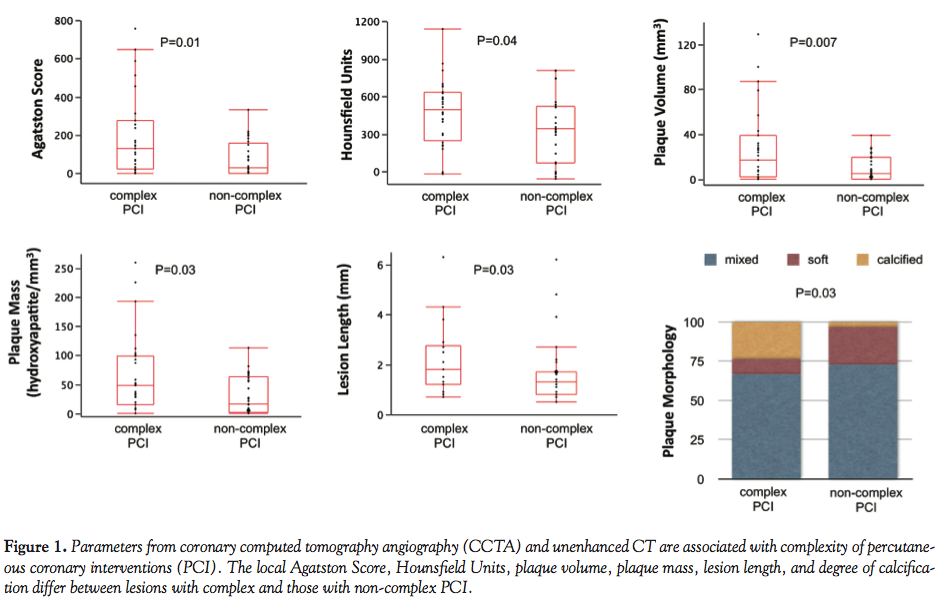 CCTA indicates complexity of PCI. Median Agatston score was significantly higher in lesions with complex as compared to those with non-complex interventions with 130 (interquartile range: 23-276) vs 29 (0-158; P=.01; n = 64). Regarding plaque density, Hounsfield Units were higher in lesions with complex as compared to non-complex PCI (493 [245-631] vs 341 [68-520 Hounsfield Units]; P=.04; n = 65). Median local plaque volume and plaque mass were higher in lesions with complex PCI with 17 (2-39) vs 5 (0-19.5 mm3; P=.007; n = 64); and 48 (15-99) vs 16 (1.5-63 mg hydroxyapatite/mm3; P=.03; n = 64), respectively. Lesions leading to complex PCI were longer compared to those with non-complex PCI (1.8 [1.2-2.8] vs 1.3 [0.8-1.7] cm; P=.03; n = 56) and had a higher rate of calcified plaques (23% vs 3%; P=.03; n = 63; Figure 1).
CCTA indicates complexity of PCI. Median Agatston score was significantly higher in lesions with complex as compared to those with non-complex interventions with 130 (interquartile range: 23-276) vs 29 (0-158; P=.01; n = 64). Regarding plaque density, Hounsfield Units were higher in lesions with complex as compared to non-complex PCI (493 [245-631] vs 341 [68-520 Hounsfield Units]; P=.04; n = 65). Median local plaque volume and plaque mass were higher in lesions with complex PCI with 17 (2-39) vs 5 (0-19.5 mm3; P=.007; n = 64); and 48 (15-99) vs 16 (1.5-63 mg hydroxyapatite/mm3; P=.03; n = 64), respectively. Lesions leading to complex PCI were longer compared to those with non-complex PCI (1.8 [1.2-2.8] vs 1.3 [0.8-1.7] cm; P=.03; n = 56) and had a higher rate of calcified plaques (23% vs 3%; P=.03; n = 63; Figure 1).
 CCTA-derived local SYNTAX scores seem to predict failed and complex PCI. There was a significant correlation between local SYNTAX scores assessed by CCTA (n = 52) and those obtained by coronary angiography (n = 64; Spearman’s rank correlation coefficient = 0.63; P<.001; Figure 2). Upon splitting the SYNTAX scores obtained by CCTA into 3 intervals, the mean values ± standard deviation of the SYNTAX score assessed by coronary angiography are 2.8 ± 1.2 for values of the local SYNTAX scores by CCTA in the interval ≤2, 6.1 ± 2.9 in the interval 2-11, and 12.0 ± 7.3 for all values >11 (Bonferroni adjusted P<.001).
CCTA-derived local SYNTAX scores seem to predict failed and complex PCI. There was a significant correlation between local SYNTAX scores assessed by CCTA (n = 52) and those obtained by coronary angiography (n = 64; Spearman’s rank correlation coefficient = 0.63; P<.001; Figure 2). Upon splitting the SYNTAX scores obtained by CCTA into 3 intervals, the mean values ± standard deviation of the SYNTAX score assessed by coronary angiography are 2.8 ± 1.2 for values of the local SYNTAX scores by CCTA in the interval ≤2, 6.1 ± 2.9 in the interval 2-11, and 12.0 ± 7.3 for all values >11 (Bonferroni adjusted P<.001).
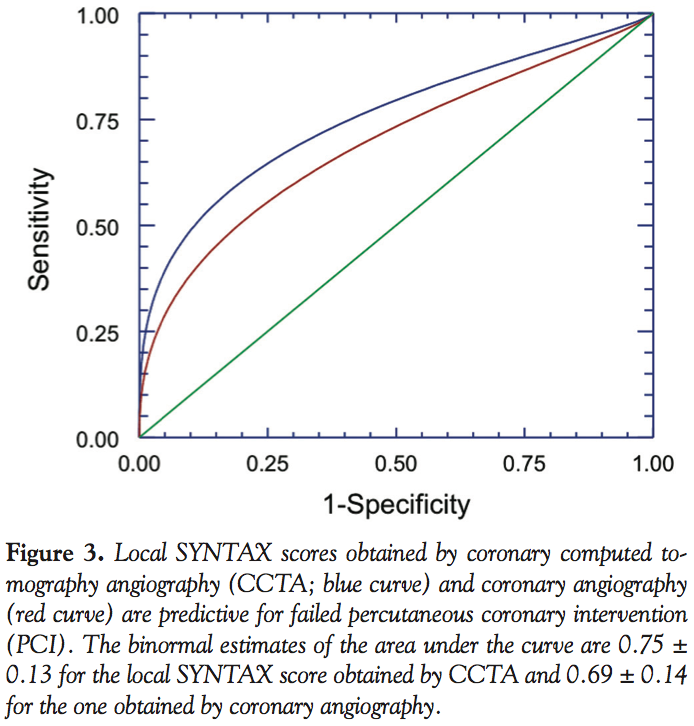 CCTA-derived local SYNTAX scores seem to be predictive for failed PCI with an area under the curve (AUC) ± standard error of 0.75 ± 0.13 in ROC analysis (Figure 3), and an intercept of 3.85 ± 1.06 (slope -0.17 ± 0.08; P=.04) assuming a logistic regression. At a CCTA-derived SYNTAX score cut-off value of 10, sensitivity was 0.66 and specifity was 0.74 for failed PCI; at an angiography-derived local SYNTAX score cut-off value of 9, sensitivity was 0.59 and specificity was 0.71, respectively (AUC = 0.69 ± 0.14; Figure 3). CCTA-derived local SYNTAX scores were less predictive of complex PCI with an AUC of 0.66 ± 0.08 in ROC analysis (cut-off value = 9, sensitivity = 0.50 and specificity = 0.82, respectively), and an intercept of 0.98 ± 0.50 (slope of -0.11 ± 0.06; P=.05) assuming a logistic regression. CCTA-derived local SYNTAX scores were not useful in predicting procedure-related complications (AUC = 0.42 ± 0.9).
CCTA-derived local SYNTAX scores seem to be predictive for failed PCI with an area under the curve (AUC) ± standard error of 0.75 ± 0.13 in ROC analysis (Figure 3), and an intercept of 3.85 ± 1.06 (slope -0.17 ± 0.08; P=.04) assuming a logistic regression. At a CCTA-derived SYNTAX score cut-off value of 10, sensitivity was 0.66 and specifity was 0.74 for failed PCI; at an angiography-derived local SYNTAX score cut-off value of 9, sensitivity was 0.59 and specificity was 0.71, respectively (AUC = 0.69 ± 0.14; Figure 3). CCTA-derived local SYNTAX scores were less predictive of complex PCI with an AUC of 0.66 ± 0.08 in ROC analysis (cut-off value = 9, sensitivity = 0.50 and specificity = 0.82, respectively), and an intercept of 0.98 ± 0.50 (slope of -0.11 ± 0.06; P=.05) assuming a logistic regression. CCTA-derived local SYNTAX scores were not useful in predicting procedure-related complications (AUC = 0.42 ± 0.9).
Discussion
Preprocedural lesion assessment by unenhanced CT for calcium scoring and CCTA, providing information about local Agatston score, Hounsfield Units, plaque volume, plaque mass, and plaque morphology, indicates complexity of PCI in patients with extensive CAD. Hence, we suggest that in patients with suspected complex CAD, preprocedural CCTA adds important information to conventional coronary angiography for planning subsequent PCI. Local SYNTAX scores derived by CCTA were shown to be predictive for failed and complex PCI. Thus, the SYNTAX score may provide an easily applicable lesion-based scoring tool of CCTA.
Despite huge advances in the development of angioplasty equipment and technique, PCI of complex coronary artery lesions still can remain demanding and afflicted with procedural complications such as coronary artery dissection and perforation.22 Failed PCI mainly occurs due to the inability to cross the lesion with a guidewire or balloon, or to open up the lesion appropriately, frequently due to heavy calcifications. In an international, multicenter, quality-control study with a concluding panel assessment of all cases by high-profile interventional cardiologists, procedural success of PCI in type A and B lesions was reported to be more than 94%.23 In our patient cohort, complex PCI was observed in 48% of the interventions, and failed PCI in 9%, respectively, which can be attributed to the higher proportion of patients with severe and complex CAD in the patient cohort with CCTA and subsequent PCI. Indeed, even higher rates of failed and complex interventions have been described in the patient populations selected for recanalization of CTOs.7,9,10,24 Our comparisons aim at an adjudication of anticipated complex PCI based on CCTA. This retrospective cohort with an unusually high percentage of complex PCI enabled us to corroborate our hypothesis through direct comparisons. In turn, preprocedural guidance of coronary intervention is deemed unnecessary for type A lesions and thus a larger series including more cases with low-risk PCI would not have increased the impact of our data.
CCTA is not only used as a diagnostic tool,4 but has also been shown to provide prognostic information regarding death, non-fatal myocardial infarction, and the need for revascularization in patients with known or suspected CAD.25 Complex PCI did not influence patient outcome as overall in-hospital MACE rate was low and in accordance with current standards in interventional cardiology. Thus, CCTA is not suggested to improve outcome in patients with complex CAD, but rather as a tool for planning and guiding procedures. Preprocedural CCTA has been systematically assessed in PCI for CTO in a few studies.9-15 Indeed, heavy calcification and occlusion length of CTO have been reported to be independent predictors of failed PCI.7,9 The potential of CCTA for PCI planning and strategic PCI guidance has recently been a subject of discussion again with major focus on CTOs.6,8 CT-guided PCI paradigms and real-time hybrid CCTA with coronary angiography have been proposed.8,26 Coronary plaque characterization by CCTA, however with rather limited spatial and temporal resolution, has been reported for risk stratification also in conventional PCI.21 Since resolution issues for plaque characterization in sub-millimeter ranges currently do not appear to be resolved for CCTA, and thus plaque characterization still represents the domain of intravascular imaging technologies,27,28 a focus on plaque characterization alone may not be sufficient for guiding PCI.
In this patient cohort, CCTA and unenhanced CT were shown to indicate complexity of subsequent PCI. CCTA and unenhanced CT parameters used for plaque evaluation such as the local Agatston score, Hounsfield Units, plaque volume, plaque mass, lesion length, and degree of calcification were all significantly associated with PCI complexity. This additional information regarding plaque evaluation obtained by CCTA is complementary to coronary angiography. Coronary angiography represents the undisputed gold standard for evaluation of CAD for PCI, with some well-known limitations nevertheless. Atherosclerotic plaques mainly consist of a lipid-rich core, calcium deposits, cellular components, as well as a fibrous cap.29 Coronary angiography clearly displays the vessel lumen; however, it misses the detection of plaque composition and even the exact degree of calcification. Whereas for the reliable assessment of plaque composition presently only intra-luminal imaging modalities like intravascular ultrasound and optical coherence tomography provide the necessary resolution,27,28 calcification clearly can be determined preprocedurally by unenhanced CT and CCTA. Moreover, CCTA allows for delineation of three-dimensional anatomy and vessel tortuosities. Lesion length determined by CCTA was associated with PCI complexity. Also in this respect, CCTA adds additional information to coronary angiography. Indeed, measurement of lesion length by coronary angiography may be handicapped due to sampling errors, foreshortening, vessel overlap, and in CTOs, lack of visualization of distal vessels in the absence of collateral filling. Furthermore, CCTA offers a three-dimensional reconstruction of the complex anatomy of tortuous vessel segments that in conjunction with two-dimensional fluoroscopy images may facilitate complex PCI.
The local SYNTAX score assessed by CCTA correlates with the angiography-derived score, and was predictive for failed, and to a lesser extent for complex PCI. This correlation suggests that CT-generated local SYNTAX scores may provide an easily applicable tool for advance lesion characterization prior to PCI. Interestingly, CCTA-derived SYNTAX scores were not useful in predicting procedure-related complications such as dissection, perforation, and plaque shift. Indeed, many procedure-related complications can be considered as operator-dependent as well as related to strategy, technique, and material chosen by the operator.
Study limitations. The limitation of this study is the relatively small patient population explained by the retrospective and hypothesis-generating design. Prospective studies with larger patient cohorts are needed to assess the impact of non-invasive lesion characterization, and in particular individual lesion characteristics integrated into the CCTA-derived SYNTAX score, on PCI strategy selection and on short- and long-term patient outcome after PCI. Furthermore, preprocedural CCTA might be tailored to patients with expected complex CAD, and additional radiation, contrast volume, and costs of CCTA have to be balanced versus potential economies in these respects during PCI due to advance information generated by CCTA.
Conclusion
The proposed preprocedural CCTA parameters indicate complexity of PCI. Thus, we suggest that in patients with suspected complex coronary anatomy, prior CCTA adds important complementary information to coronary angiography for planning subsequent PCI strategy.
References
- Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972.
- Valgimigli M, Serruys PW, Tsuchida K, et al. Cyphering the complexity of coronary artery disease using the syntax score to predict clinical outcome in patients with three-vessel lumen obstruction undergoing percutaneous coronary intervention. Am J Cardiol. 2007;99(8):1072-1081.
- Capodanno D, Capranzano P, Di Salvo ME, et al. Usefulness of SYNTAX score to select patients with left main coronary artery disease to be treated with coronary artery bypass graft. JACC Cardiovasc Interv. 2009;2(8):731-738.
- von Ballmoos MW, Haring B, Juillerat P, Alkadhi H. Meta-analysis: diagnostic performance of low-radiation-dose coronary computed tomography angiography. Ann Intern Med. 2011;154(6):413-420.
- Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005;1(2):219-227.
- Magro M, Schultz C, Simsek C, et al. Computed tomography as a tool for percutaneous coronary intervention of chronic total occlusions. EuroIntervention. 2010;6(Suppl G):G123-G131.
- Yokoyama N, Yamamoto Y, Suzuki S, et al. Impact of 16-slice computed tomography in percutaneous coronary intervention of chronic total occlusions. Catheter Cardiovasc Interv. 2006;68(1):1-7.
- Hecht HS. Applications of multislice coronary computed tomographic angiography to percutaneous coronary intervention: how did we ever do without it? Catheter Cardiovasc Interv. 2008;71(4):490-503.
- Mollet NR, Hoye A, Lemos PA, et al. Value of preprocedure multislice computed tomographic coronary angiography to predict the outcome of percutaneous recanalization of chronic total occlusions. Am J Cardiol. 2005;95(2):240-243.
- Li P, Gai LY, Yang X, et al. Computed tomography angiography-guided percutaneous coronary intervention in chronic total occlusion. J Zhejiang Univ Sci B. 2010;11(8):568-574.
- Garcia-Garcia HM, van Mieghem CA, Gonzalo N, et al. Computed tomography in total coronary occlusions (CTTO registry): radiation exposure and predictors of successful percutaneous intervention. EuroIntervention. 2009;4(5):607-616.
- Soon KH, Cox N, Wong A, et al. CT coronary angiography predicts the outcome of percutaneous coronary intervention of chronic total occlusion. J Interv Cardiol. 2007;20(5):359-366.
- Ehara M, Terashima M, Kawai M, et al. Impact of multislice computed tomography to estimate difficulty in wire crossing in percutaneous coronary intervention for chronic total occlusion. J Invasive Cardiol. 2009;21(11):575-582.
- Hsu JT, Kyo E, Chu CM, et al. Impact of calcification length ratio on the intervention for chronic total occlusions. Int J Cardiol. 2011;150(2):135-141. Epub 2010 Mar 30.
- Cho JR, Kim YJ, Ahn CM, et al. Quantification of regional calcium burden in chronic total occlusion by 64-slice multi-detector computed tomography and procedural outcomes of percutaneous coronary intervention. Int J Cardiol. 2010;145(1):9-14.
- Smith SC Jr, Dove JT, Jacobs AK, et al. ACC/AHA guidelines for percutaneous coronary intervention (revision of the 1993 PTCA guidelines) — executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (committee to revise the 1993 guidelines for percutaneous transluminal coronary angioplasty) endorsed by the Society for Cardiac Angiography and Interventions. Circulation. 2001;103(24):3019-3041.
- Saur SC, Cattin PC, Desbiolles L, et al. Prediction rules for the detection of coronary artery plaques: evidence from cardiac CT. Invest Radiol. 2009;44(8):483-490.
- Anderson HV, Shaw RE, Brindis RG, et al. Relationship between procedure indications and outcomes of percutaneous coronary interventions by American College of Cardiology/American Heart Association Task Force Guidelines. Circulation. 2005;112(18):2786-2791.
- Silber S, Albertsson P, Aviles FF, et al. Guidelines for percutaneous coronary interventions. The task force for percutaneous coronary interventions of the European Society of Cardiology. Eur Heart J. 2005;26(8):804-847.
- King SB 3rd, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 Focused Update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association task force on practice guidelines: 2007 writing group to review new evidence and update the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention, writing on behalf of the 2005 writing committee. Circulation. 2008;117:261-295.
- Kinohira Y, Akutsu Y, Li HL, et al. Coronary arterial plaque characterized by multislice computed tomography predicts complications following coronary intervention. Int Heart J. 2007;48(1):25-33.
- Werner GS, Gitt AK, Zeymer U, et al. Chronic total coronary occlusions in patients with stable angina pectoris: impact on therapy and outcome in present day clinical practice. Clin Res Cardiol. 2009;98(7):435-441.
- Maier W, Mini O, Antoni J, et al. ABC stenosis morphology classification and outcome of coronary angioplasty: reassessment with computing techniques. Circulation. 2001;103(9):1225-1231.
- Qu XK, Fang WY, Ye JD, et al. [Values in preoperative assessment of occlusion and intra-operative guidance of 64 row spiral CT in percutaneous coronary intervention for chronic coronary occlusion]. Zhonghua Yi Xue Za Zhi. 2008;88(46):3268-3271.
- Buechel RR, Pazhenkottil AP, Herzog BA, et al. Prognostic performance of low-dose coronary CT angiography with prospective ECG triggering. Heart. 2011;97(17):1385-1390. Epub 2011 Apr 12.
- Roguin A, Abadi S, Engel A, Beyar R. Novel method for real-time hybrid cardiac CT and coronary angiography image registration: visualising beyond luminology, proof-of-concept. EuroIntervention. 2009;4(5):648-653.
- Kang SJ, Mintz GS, Akasaka T, et al. Optical coherence tomographic analysis of in-stent neoatherosclerosis after drug-eluting stent implantation. Circulation. 2011;123(25):2954-2963.
- Wu X, Maehara A, Mintz GS, et al. Virtual histology intravascular ultrasound analysis of non-culprit attenuated plaques detected by grayscale intravascular ultrasound in patients with acute coronary syndromes. Am J Cardiol. 2010;105(1):48-53.
- Libby P. Atherosclerosis: disease biology affecting the coronary vasculature. Am J Cardiol. 2006;98(12A):3Q-9Q.
____________________________________________
From the 1Department of Cardiology, Cardiovascular Center, 2Institute of Diagnostic and Interventional Radiology, 3Cardiac Imaging, University Hospital Zurich, Switzerland, 3FB Mathematics and Computer Science, University of Bremen, Germany.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. Lüscher is a consultant for St Jude, Medtronic Biosensors, and has received travel reimbursements from St Jude and Phillips.
Manuscript submitted November 18, 2011, provisional acceptance given December 20, 2011, final version accepted February 7, 2012.
Address for correspondence: Willibald Maier, MD, Department of Cardiology, Cardiovascular Center, University Hospital Zürich, Rämistrasse 100, 8091 Zürich, Switzerland. Email: karmaiew@usz.uzh.ch











