Coronary Stent Fracture: Still a Cause of Stent Failure
Key words: cardiac computed tomography angiography, stenting, optical coherence tomography, PCI
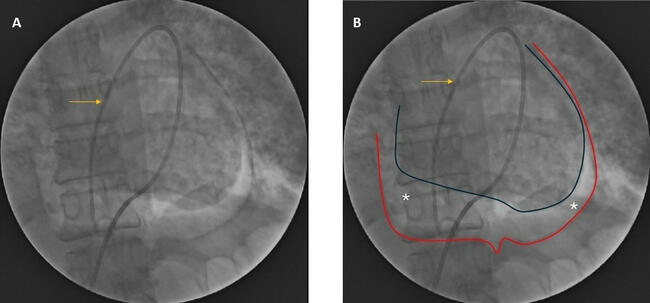
A 43-year-old man presented to his cardiologist’s office with a history of exertion-related chest pain. His past medical history included type 2 diabetes mellitus, hypercholesterolemia, smoking, and a family history of coronary artery disease. His physical examination was normal. After positive exercise-induced chest discomfort, the patient underwent coronary computed tomography angiography (CCTA), which showed marked and diffuse calcified coronary plaques (calcium score, 2011 HU; >90th percentile for age) and severe stenosis in the proximal right coronary artery (RCA) (Figure 1A). He was referred to our catheterization laboratory for an elective coronary angiogram, which confirmed proximal and mid RCA stenoses. Percutaneous coronary intervention (PCI) was performed with two overlapping everolimus-eluting stents (2.75 x 38 mm and 3.0 x 33 mm Xience Prime; Abbott) implanted from the proximal to the distal part of the vessel (Figure 1B).
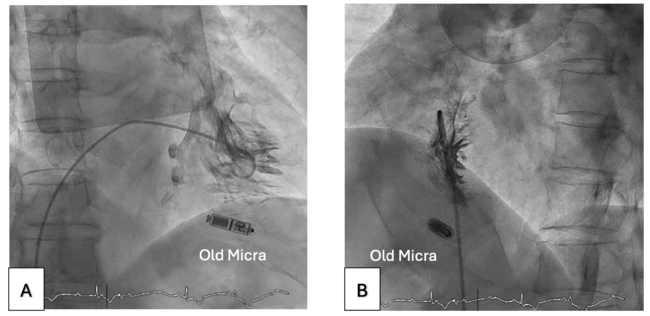
Ten months after the index procedure, the patient presented with recurrent chest pain. He underwent a novel CCTA showing an in-stent focal restenosis at the mid RCA, most likely related to a stent fracture. A second coronary angiography showed a focal restenosis and fluoroscopy also suggested a stent fracture (Figure 2). Optical coherence tomography with three-dimensional (3D) reconstruction revealed well-apposed stents and most struts covered with a thin intimal hyperplasia both proximal and distal to the restenosis. The neointimal tissue of the restenosis site showed fibrotic high-intensity homogeneous pattern. There was a circumferential and partial stent strut fracture grade III (Figure 3). The restenosis was successfully treated with zotarolimus drug-eluting stent implantation.
In the present case, multimodality images facilitated understanding of the mechanism of restenosis; the optical coherence tomography with 3D reconstruction allowed clear identification of the extent of the stent fracture and clarified its subsequent optimal treatment.
From the Hospital Israelita Albert Einstein, São Paulo, Brazil.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted November 1, 2018.
Address for correspondence: Adriano Caixeta, MD, PhD, Department of Cardiovascular Intervention, Hospital Israelita Albert Einstein, Av. Albert Einstein, 627, Morumbi, São Paulo 05652-000, Brazil. Email: adriano.caixeta@einstein.br. Twitter: @adrianocaixeta