

CT-Reconstructed Three-Dimensional Printed Models of the Right Subclavian Artery and Aorta Define Age-Related Changes and Facilitate Benchtop Catheter Testing
Abstract: Background. Severe tortuosity of the right subclavian artery (RSCA) encountered during transradial cardiac catheterization can lead to longer procedures, increased fluoroscopy time, inability to engage the coronary artery ostia, and potentially procedural failure. Increasing age is strongly correlated with subclavian tortuosity; however, the magnitude and direction of age-related changes in aortic and subclavian artery anatomy have not been defined. Methods. Chest computed tomography (CT) angiograms of 14 patients (6 age <45 years and 8 age ≥75 years) were evaluated for RSCA tortuosity. Measurements were taken along the midline of the vessel and compared to the straight distance traveled (index of tortuosity = straight distance/midline length). One normal and one tortuous subclavian were selected for three-dimensional printing and various catheters were benchtop tested on both models. Results. The older group had longer (11.95 cm vs 9.6 cm; P<.01) and more tortuous subclavian arteries (lower index of tortuosity, 0.65 vs 0.76; P<.01) with more posterior unfolding (distance to most posterior aspect, 3.74 ± 0.77 cm vs 1.76 ± 0.58 cm; P<.001). Engagement of the coronary arteries of the normal model was significantly easier, with successful engagement of one or both coronaries with every catheter (n=7). Only 2 of 7 catheters (Radial Brachial and Extra Backup 3.0) were able to engage the coronary arteries in the tortuous model. Conclusion. Age is associated with elongation, tortuosity, and posterior unfolding of the RSCA. Three-dimensional printing of normal and tortuous arteries is feasible and shows potential to test differences between catheters.
J INVASIVE CARDIOL 2014;26(10):E141-E144
Key words: tortuosity, computed tomography, right subclavian artery
_____________________________
The transradial approach for coronary angiography and interventions is becoming increasingly popular worldwide. Transradial cardiac catheterization (TRCC) offers many advantages over the traditional transfemoral approach, including decreased costs and increased patient satisfaction.1 In addition, transradial catheterization is associated with a significant decrease in access-site complications and bleeding, which is increasingly important in patients on anticoagulation and antiplatelet therapy.2 The right radial artery is used in nearly 90% of cases, primarily due to the ease and familiarity of catheter and equipment manipulation from the patient’s right side as in the femoral approach.3,4 However, a tortuous right subclavian artery can lead to difficulties during the transradial approach, leading to prolonged manipulation of catheters, access failure, and potentially arterial dissection.5 Risk factors of severe tortuosity of the right subclavian artery have been established: systemic hypertension, female gender, older age, short stature, and high body mass index, yet there are no commercially available catheters specifically designed to overcome subclavian artery tortuosity.5 In this study, we have defined the degree of tortuosity of the right subclavian artery with increasing age, and we have used three-dimensional (3D) reconstructed models to evaluate the ability of catheters to engage the coronaries of patients with normal and tortuous subclavian arteries.
Methods
Computed tomography angiography image analysis and index of tortuosity calculation. We performed a retrospective review of 14 patients who were referred for chest computed tomography (CT) angiograms (1.25 mm slices) to rule out pulmonary embolism. Patients with positive findings on CT or significant structural abnormalities were excluded. Patients were divided into two groups: group 1 (n=6) with patients age <45 and group 2 (n=8) with patients age ≥75 years. Using OsirX version 5.7, 32-bit CT scans of each patient were reconstructed using the 3D curved multiplanar reconstruction tool and subsequently reviewed in a random order by a single observer. The software allowed the user to view the 3D reconstructed 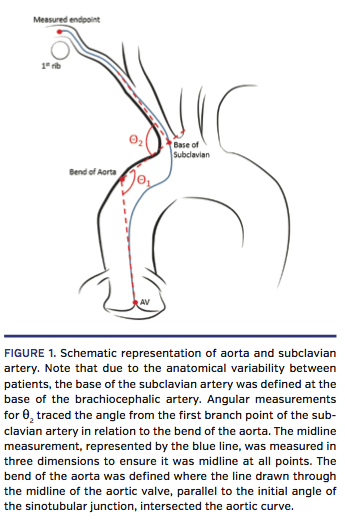 dataset in any direction and plot a path of the tortuous vessel in 3D space. The subclavian artery was evaluated from the origin of the innominate artery to where the artery passes superior to the 1st rib (Figure 1). The subclavian artery distal to the 1st rib is relatively straight, with minimal difficulty for catheter access; thus, it was not included in the investigation. In addition to this, measurements from the base of the aorta to the innominate artery and the angles of the 1st aortic bend (q2) and subclavian artery (q2) were taken. Total length of the subclavian was measured by tracing the midline of the artery as it traverses from the origin of the innominate to the end described previously at the first rib. Straight distance was defined as the linear distance between the origin of the innominate to the endpoint of the subclavian. The index of tortuosity was calculated using the formula: (straight distance/midline length). The higher the index, the straighter the vessel. We then assessed the manner in which the subclavian artery develops tortuosity with age, ie, does it unfold posteriorly, anteriorly, or both? The distance between the most posterior and anterior aspect in relation to base of the subclavian was also recorded.
dataset in any direction and plot a path of the tortuous vessel in 3D space. The subclavian artery was evaluated from the origin of the innominate artery to where the artery passes superior to the 1st rib (Figure 1). The subclavian artery distal to the 1st rib is relatively straight, with minimal difficulty for catheter access; thus, it was not included in the investigation. In addition to this, measurements from the base of the aorta to the innominate artery and the angles of the 1st aortic bend (q2) and subclavian artery (q2) were taken. Total length of the subclavian was measured by tracing the midline of the artery as it traverses from the origin of the innominate to the end described previously at the first rib. Straight distance was defined as the linear distance between the origin of the innominate to the endpoint of the subclavian. The index of tortuosity was calculated using the formula: (straight distance/midline length). The higher the index, the straighter the vessel. We then assessed the manner in which the subclavian artery develops tortuosity with age, ie, does it unfold posteriorly, anteriorly, or both? The distance between the most posterior and anterior aspect in relation to base of the subclavian was also recorded.
3D model catheterization. Two subjects, one from each group, were selected for 3D reconstruction. They were specifically chosen to represent the most tortuous and the straightest subclavian arteries. Using 3D model volume rendering with ITK-SNAP,6 models of the patients’ subclavian arteries and aortas (including left and right coronary ostia) were created. These models were commercially 3D printed using a photopolymer resin that is cured with ultraviolet light as it is building. The wall thickness of the models was between 1.9 and 2.1 mm (Figure 2). The two models were flushed with saline and various cardiac catheters (Table 1) were placed through the subclavian artery to engage the left or right coronary artery. After each  attempt, the models were flushed again with saline and a new catheter was used. All trials of catheter engagement and assessment of difficulty were performed by two cardiologists. The assessment was based on the ease of the catheters to navigate the right subclavian artery and the ability to engage the targeted coronary ostia, which was visually confirmed, as the models are translucent.
attempt, the models were flushed again with saline and a new catheter was used. All trials of catheter engagement and assessment of difficulty were performed by two cardiologists. The assessment was based on the ease of the catheters to navigate the right subclavian artery and the ability to engage the targeted coronary ostia, which was visually confirmed, as the models are translucent.
Statistical analysis. Continuous variables obtained from CT scans were analyzed between groups using non-paired student’s t-test. Analyses were performed using STATA version 11.0. A P-value <.05 was considered statistically significant.
Results
Baseline patient characteristics are listed in Table 2. In addition to older age, group 2 had a higher average body mass index and blood pressure, although a lower percentage of females. As expected, older patients had more tortuous arteries than young patients. Group 1 had a higher index of tortuosity compared to group 2 (0.76 vs 0.65, respectively; P<.01). While the length from the base of the aorta to the base of the subclavian was similar between the two groups, (9.21 cm vs 9.58 cm), 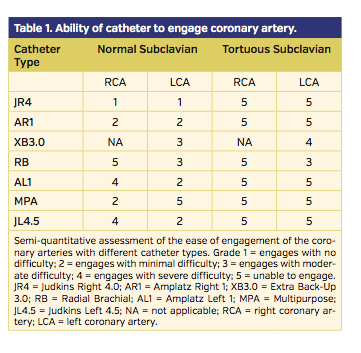 group 2 had a significantly longer subclavian artery (11.95 cm vs 9.6 cm; P<.01). The subclavian artery appears to unfold posteriorly with age, as evidenced by an increased distance to the most posterior aspect (3.74 ± 0.77 cm vs 1.76 ± 0.58 cm; P<.001), with no difference in the distance to the most anterior aspect of the artery (0.16 ± 0.32 vs 0.20 ± 0.21 cm; P=.80).
group 2 had a significantly longer subclavian artery (11.95 cm vs 9.6 cm; P<.01). The subclavian artery appears to unfold posteriorly with age, as evidenced by an increased distance to the most posterior aspect (3.74 ± 0.77 cm vs 1.76 ± 0.58 cm; P<.001), with no difference in the distance to the most anterior aspect of the artery (0.16 ± 0.32 vs 0.20 ± 0.21 cm; P=.80).
The 3D printed models were able to discriminate between easy coronary engagement and difficult coronary engagement. Successful engagement of one or both coronaries was achieved with every catheter in the normal subclavian model, with the JR4 catheter engaging both the left and right coronary most reliably. Engagement of the coronary arteries was substantially more difficult in the 3D model from group 2 (Table 2). In the severely tortuous subclavian model, we were not able to engage the right coronary with any catheter and were only able to engage the left coronary with the Extra Backup 3.0 and Radial Brachial catheters.
Discussion
The transradial approach for cardiac catheterization is becoming increasingly popular due to reduced cost, increased patient comfort, and earlier patient discharge when compared to the femoral approach.7 One of the major drawbacks to the 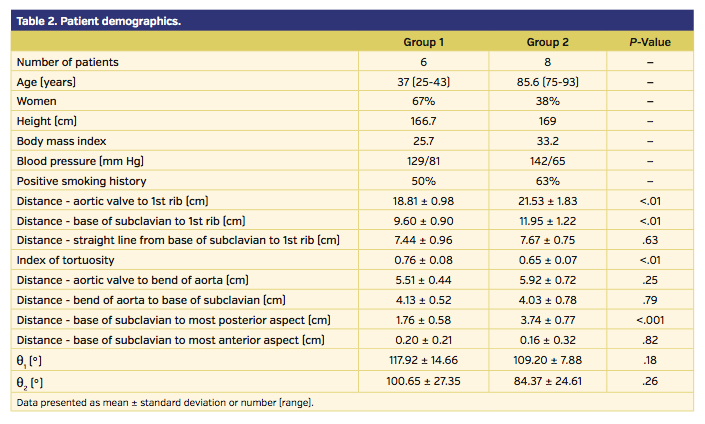 transradial approach is the increased procedure length, which is further prolonged by severely tortuous right subclavian artery.5,8 While the risk factors for tortuous right subclavian artery have been established, for the first time we have defined the degree of increased tortuosity seen in elderly patients. Our data demonstrated that the right subclavian artery in elderly patients was longer and more tortuous than young patients and unfolded posteriorly, resulting in difficulty maneuvering catheters.
transradial approach is the increased procedure length, which is further prolonged by severely tortuous right subclavian artery.5,8 While the risk factors for tortuous right subclavian artery have been established, for the first time we have defined the degree of increased tortuosity seen in elderly patients. Our data demonstrated that the right subclavian artery in elderly patients was longer and more tortuous than young patients and unfolded posteriorly, resulting in difficulty maneuvering catheters.
Currently, cardiac catheterization is performed without knowing the extent of tortuosity of the right subclavian artery. In elderly patients with extremely tortuous right subclavian artery, TRCC can be very difficult, often requiring the use of several catheters prior to finding one that can successfully engage the coronary ostia. This leads to prolonged procedure time, increased contrast use, increased radiation exposure for the patient and operator, and increased overall cost.7,9 There are a number of dedicated radial catheter shapes currently available and these engage the coronary ostia well from the radial approach. However, there are no catheters currently available that address the issue of subclavian tortuosity. Herein, we define the shape changes in the subclavian and aorta that occur with age, and demonstrate the utility of the emerging technology of 3D printing in assessing novel catheter designs. Our model shows significant differences between the normal and tortuous right subclavian artery in the ability of catheters to engage the coronary, and therefore allows testing of improved catheter designs on the benchtop. This was not an exhaustive study of all available catheter types, but a demonstration of feasibility of the concept. Future catheter designs should be optimized in such a system before proceeding to clinical trials.
Conclusion
Age is associated with elongation and tortuosity of the right subclavian artery and aorta, and the tortuosity is largely due to posterior unfolding. Dedicated benchtop catheter testing for the transradial approach using CT-reconstructed 3D printed models is a promising and viable method for studying catheters for transradial use.
References
- Mitchell MD, Hong JA, Lee BY, Umscheid CA, Bartsch SM, Don CW. Systematic review and cost-benefit analysis of radial artery access for coronary angiography and intervention. Circ Cardiovasc Qual Outcomes. 2012;5(4):454-462.
- Bertrand OF, Belisle P, Joyal D. Comparison of transradial and femoral approaches for percutaneous coronary interventions: a systematic review and hierarchical Bayesian meta-analysis. Am Heart J. 2012;163(4):632-648.
- Bertrand OF, Rao SV, Pancholy S, et al. Transradial approach for coronary angiography and interventions: results of the first international transradial practice survey. JACC Cardiovasc Interv. 2010;3(10):1022-1031.
- Wu CJ, Lo PH, Chang KC, Fu M, Lau KW, Hung JS. Transradial coronary angiography and angioplasty in Chinese patients. Cathet Cardiovasc Diagn. 1997;40(2):159-163.
- Cha KS, Kim MH, Kim HJ. Prevalence and clinical predictors of severe tortuosity of right subclavian artery in patients undergoing transradial coronary angiography. Am J Cardiol. 2003;92(10):1220-1222.
- Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006;31(3):1116-1128.
- Louvard Y, Lefevre T, Allain A, Morice M. Coronary angiography through the radial or the femoral approach: the CARAFE study. Catheter Cardiovasc Interv. 2001;52(2):181-187.
- Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J. 2009;157(1):132-140.
- Mercuri M, Mehta S, Xie C, Valettas N, Velianou JL, Natarajan MK. Radial artery access as a predictor of increased radiation exposure during a diagnostic cardiac catheterization procedure. JACC Cardiovasc Interv. 2011;4(3):347-352.
________________________________
From the 1University of California, San Francisco, California; and 2the University of Newcastle, Newcastle, Australia.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 18, 2014, final version accepted May 5, 2014.
Address for correspondence: Andrew J. Boyle, MBBS, PhD, FRACP, University of Newcastle Department of Medicine, Division of Cardiology, John Hunter Hospital, Lookout Rd, New Lambton Heights, Newcastle, NSW 2905, Australia. Email: andrewboyle500@gmail.com











