

Dislocation of an Infected and Abandoned Pacemaker Lead
ABSTRACT: We present a case of pacemaker lead dislodgment in an 83-year-old patient with a pacemaker infection. Initially, the generator and the proximal part of the leads were removed, and the remaining leads were severed and abandoned. Twenty-five days later, dislodgment of both abandoned leads and systemic infection were documented. The leads were then surgically removed without further complications.
J INVASIVE CARDIOL 2012;24(11):E297-E299
___________________________________________________________
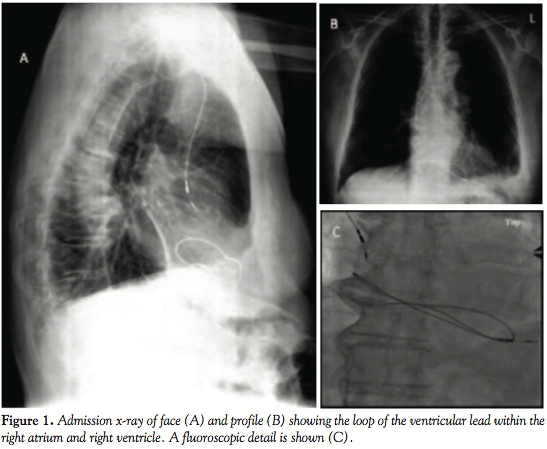 Case Report. An 83-year-old hypertensive man who had undergone implantation of a dual-chamber pacemaker due to symptomatic sinus bradycardia presented with local inflammation in the generator pocket 2 years after the implantation. At presentation the patient was asymptomatic, afebrile and had no signs of systemic infection. The C-reactive protein levels, the erythrocyte sedimentation rate, and the white blood cell count were normal and blood cultures were negative. Partial removal of the device was decided at the first referral center. Debridement of the infected area was performed, the generator and the proximal part of the leads were removed, and the remaining leads were severed from the infected area and abandoned. Cultures of the debrided tissue revealed Staphylococcus epidermidis infection, and the patient was treated with 15 days of intravenous antistaphylococcal antibiotics and subsequent oral therapy. The patient at presentation was in sinus rhythm, was non-pacemaker dependent, and was not receiving anticoagulants. Twenty-five days after the device extraction and with good healing of the wound, the patient had a transient ischemic attack (TIA). The patient was therefore referred to our cardiology department, where an emergency thoracotomy was performed for further evaluation and fluoroscopic lead extraction. The chest x-ray performed at admission (Figures 1A and 1B) showed that the distal part of the right ventricular lead had been dislodged and formed a loop within the right atrium and right ventricle and that the atrial lead had “fallen” out of the appendage. A detailed view of the loop based on the fluoroscopic study is shown in Figure 1C.
Case Report. An 83-year-old hypertensive man who had undergone implantation of a dual-chamber pacemaker due to symptomatic sinus bradycardia presented with local inflammation in the generator pocket 2 years after the implantation. At presentation the patient was asymptomatic, afebrile and had no signs of systemic infection. The C-reactive protein levels, the erythrocyte sedimentation rate, and the white blood cell count were normal and blood cultures were negative. Partial removal of the device was decided at the first referral center. Debridement of the infected area was performed, the generator and the proximal part of the leads were removed, and the remaining leads were severed from the infected area and abandoned. Cultures of the debrided tissue revealed Staphylococcus epidermidis infection, and the patient was treated with 15 days of intravenous antistaphylococcal antibiotics and subsequent oral therapy. The patient at presentation was in sinus rhythm, was non-pacemaker dependent, and was not receiving anticoagulants. Twenty-five days after the device extraction and with good healing of the wound, the patient had a transient ischemic attack (TIA). The patient was therefore referred to our cardiology department, where an emergency thoracotomy was performed for further evaluation and fluoroscopic lead extraction. The chest x-ray performed at admission (Figures 1A and 1B) showed that the distal part of the right ventricular lead had been dislodged and formed a loop within the right atrium and right ventricle and that the atrial lead had “fallen” out of the appendage. A detailed view of the loop based on the fluoroscopic study is shown in Figure 1C.
 The brain CT scan showed two old ischemic lesions in the left cerebellum hemisphere and right frontal lobe; hemorrhage and mycotic aneurysms were excluded. Transesophageal cardiac echocardiography (Figure 2) revealed a large echogenic mass (13 mm x 18 mm) that was thought to be vegetation on the ventricular lead loop and showed that the lead was tangled within the tricuspid valve generating valve insufficiency. Paradoxical embolism was excluded in the absence of a patent foramen ovale. The left atrium appendage was also clear for thrombi and “smoke.” Carotid and vertebrobasilar ultrasound did not detect significant stenosis or soft lesions. Although echocardiography did not reveal an embolic source, the patient’s TIA was considered unrelated to the lead mass and was attributed to silent atrial fibrillation. Systemic anticoagulation with low-molecular-weight heparin was therefore initiated. Blood cultures were negative, and the patient remained afebrile. Because of the size of the mass and the peculiar loop within the valve, percutaneous removal was considered to be high risk for ventricular arrhythmias and mechanical damage to the valve during extraction;1,2 therefore, the patient was scheduled for surgical removal of the mass. Vegetations, which were found on both lead fragments, were culture positive for the same organism that was found in pocket debridement. The patient received appropriate antibiotic medication and was discharged in a stable clinical condition.
The brain CT scan showed two old ischemic lesions in the left cerebellum hemisphere and right frontal lobe; hemorrhage and mycotic aneurysms were excluded. Transesophageal cardiac echocardiography (Figure 2) revealed a large echogenic mass (13 mm x 18 mm) that was thought to be vegetation on the ventricular lead loop and showed that the lead was tangled within the tricuspid valve generating valve insufficiency. Paradoxical embolism was excluded in the absence of a patent foramen ovale. The left atrium appendage was also clear for thrombi and “smoke.” Carotid and vertebrobasilar ultrasound did not detect significant stenosis or soft lesions. Although echocardiography did not reveal an embolic source, the patient’s TIA was considered unrelated to the lead mass and was attributed to silent atrial fibrillation. Systemic anticoagulation with low-molecular-weight heparin was therefore initiated. Blood cultures were negative, and the patient remained afebrile. Because of the size of the mass and the peculiar loop within the valve, percutaneous removal was considered to be high risk for ventricular arrhythmias and mechanical damage to the valve during extraction;1,2 therefore, the patient was scheduled for surgical removal of the mass. Vegetations, which were found on both lead fragments, were culture positive for the same organism that was found in pocket debridement. The patient received appropriate antibiotic medication and was discharged in a stable clinical condition.
Discussion. Infection is a serious complication of device implantation. The most common clinical presentation is pocket infection. Late infections are usually more indolent without systemic manifestations.1 Patients with device infection should undergo complete device removal regardless of clinical presentation.2 We present a case of pocket infection treated with partial removal of the implanted pacemaker that led to dislodgment of lead remnants and systemic infection.
This case illustrates the dislodgment of abandoned and infected pacing leads, and several important clinical considerations can be highlighted. In the PASE trial, erosion and pocket infection were the most common types of pacemaker infections and occurred in 0.5% of pacemaker implantations.2 Late infections are frequently caused by Staphylococcus epidermidis,1 which is more indolent without systemic manifestations and explains the delayed presentation of infection in our case. A previous study by Margey et al has shown that partial removal or conservative therapy is followed by relapses in 67% of cases, with mortality occurring in 8.4% of the cases.3 An additional problem to partial removal of a device is that abandoned leads have the potential to migrate, especially if no adequate lead stabilization in the pocket is employed. The first large series of abandoned pacemaker leads reported a 20% complication rate and an 8% lead migration rate.4 The apparent cause of migration in our case was that the proximal ends were severed quite deeply, leading to inadequate stabilization of the lead remnants. Lead extraction in our patient was considered mandatory due to the documentation of endocarditis and lead migration. Lead extractions in current practice are usually carried out in the cardiac catheterization laboratory and only 4% of patients are led to surgery5 when fluoroscopic extraction is considered as high risk. Lead extraction in general should be taken seriously and performed cautiously based on indications since it may have potential risks, including death. However, in high-volume experienced centers, lead extraction has high success with low complication rates. Indications of extraction have been applied by the Heart Rhythm Society policy statement in order to help clinicians’ decision making.6 In cases with pocket infection, total extraction of the system is a class I, level of evidence B indication.6
Another important issue in our case report is the differential diagnosis of our patient’s thrombotic episode. Paradoxical septic embolism was excluded and the TIA was attributed to silent atrial fibrillation based on history of sick sinus syndrome, age and the brain CT scan findings suggesting older embolic/ischemic lesions. Previous studies have shown that atrial fibrillation is found incidentally in about 25% of admissions for a stroke. Complication risk increases significantly with age but seems to be the same for symptomatic and asymptomatic patients.7 Other risk factors that increased the thrombotic risk were hypertension and limited mobilization due to prolonged hospitalization.7
Another challenging issue is the presence of systemic infection in the absence of clinical signs of systemic infection and negative blood tests. This could be explained by prior antibiotic use and by the more indolent course of Staphylococcus epidermidis infections.
Conclusion
Pacemaker infection is a very serious complication that is potentially life threatening, and management must be in accordance with accepted guidelines. In cases of pacemaker pocket infection, even those without any signs of systemic infection, incomplete hardware removal is an unacceptable approach. Total removal of the device with appropriate duration of antimicrobial therapy often results in the best patient outcomes.
References
- Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by the American Heart Association (AHA). Heart Rhythm. 2009;6(7):1085-1104.
- Link MS, Estes NA 3rd, Griffin JJ, et al. Complications of dual chamber pacemaker implantation in the elderly. Pacemaker Selection in the Elderly (PASE) Investigators. J Interv Card Electrophysiol. 1998;2(2):175-179.
- Margey R, McCann H, Blake G, et al. Contemporary management of and outcomes from cardiac device related infections. Europace. 2010;12(1):64-70.
- Böhm A, Pintér A, Duray G, et al. Complications due to abandoned noninfected pacemaker leads. Pacing Clin Electrophysiol. 2001;24(12):1721-1724.
- Kennergren C, Bjurman C, Wiklund R, Gäbel J. A single centre experience of over one thousand lead extractions. Europace. 2009;11(5):612-617.
- Love CJ, Wilkoff BL, Byrd CL, et al. Recommendations for extraction of chronically implanted transvenous pacing and defibrillator leads: indications, facilities, training. North American Society of Pacing and Electrophysiology Lead Extraction Conference Faculty. Pacing Clin Electrophysiol. 2000;23(4):544-551.
- Savelieva I, Camm AJ. Clinical relevance of silent atrial fibrillation: prevalence, prognosis, quality of life, and management. J Interv Card Electrophysiol. 2000;4(2):369-382.
- Furie KL, Kasner SE, Adams RJ, et al. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:227-276.
___________________________________________________________
From the Second Department of Cardiology, Onassis Cardiac Surgery Center, Athens, Greece.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 23, 2012, provisional acceptance given May 22, 2012, final version accepted July 16, 2012.
Address for correspondence: Anna G. Kostopoulou, MD, Onassis Cardiac Surgery Center, Syngrou 356, Kallithea, 17674, Athens, Greece. Email: annapanagi@hotmail.com












