

Early Stenosis in a Gore-Tex Graft Connected to the Left Main: An Emergency Transradial Angioplasty for a Complication in a Cabrol Procedure
Abstract: This is a case report of a successful transradial percutaneous intervention in a stenosis in a Cabrol graft. Very few reports have been published about percutaneous interventional solutions to complications in this kind of graft, and none have used the transradial approach. The Cabrol technique is used to re-implant coronary arteries after aortic root replacement using a Dacron or Gore-Tex graft interposed between the aortic root graft and the native coronary artery. Due to the dearth of reports on interventional solutions to complications in Cabrol-Grafts, most interventional cardiologists have little to no experience in approaching postsurgical aortic composite graft-coronary (ostial, body, or distal) lesions percutaneously, when the anatomy has been altered by a Cabrol graft. This article will elaborate on the anatomical considerations essential for performing this type of angioplasty procedures in this type of grafting and it will present the transradial approach as feasible and an excellent option for this type of procedure. We report on a case of an emergency angioplasty to rescue a patient who had persisted with hemodynamic instability after 48 hours of a Cabrol procedure which had been performed to repair an aortic type A dissection, caused during an aortic valve replacement.
J INVASIVE CARDIOL 2012;24(10):539-542
Key words: Cabrol procedure, left main, Gore-Tex graft, angioplasty
_________________________________________________________
The treatment of acute dissection of the ascending thoracic aorta involves the reconstruction of the aorta and revascularization by reimplantation of the coronary ostia. The original technique was described by Bentall and de Bono in 1968.1 However, a number of postoperative complications such as ostial coronary stenosis can develop as a consequence of the tension at the site of the coronary aorta anastomosis; because of this, several alternative surgical techniques including the Cabrol repair have been developed to try to minimize these complications.2,3 Nowadays, the Cabrol technique is still used, albeit less frequently; in the case of our patient, it was an emergency procedure and it is very important to recognize that the development of stenosis at the coronary-Cabrol graft anastomotic site or a diffuse stenosis secondary to retraction of the material is potentially catastrophic.3 Occlusion and stenosis at the coronary-Cabrol graft anastomosis have been reported and managed surgically.4,5 However, very few cases of percutaneous intervention of stenosis through the Cabrol graft have been performed,6-8 and no reports exist of the feasibility of the radial approach, as in the current case report.
 The Cabrol technique involves connecting a separate Dacron or Gore-Tex tube, in a side-to-side fashion from the main ascending aortic graft to the separated opening of the coronary ostia (Figure 1).2,9 We report on the case of an emergency percutaneous intervention to rescue a Cabrol graft-left main in a patient who persisted with hemodynamic instability for 48 hours after surgery for an aortic valve replacement complicated with an aortic dissection.
The Cabrol technique involves connecting a separate Dacron or Gore-Tex tube, in a side-to-side fashion from the main ascending aortic graft to the separated opening of the coronary ostia (Figure 1).2,9 We report on the case of an emergency percutaneous intervention to rescue a Cabrol graft-left main in a patient who persisted with hemodynamic instability for 48 hours after surgery for an aortic valve replacement complicated with an aortic dissection.
Case Report
 A 67-year-old male presented with a history of smoking, aortic valve replacement in 1995, and dyspnea on exertion beginning in 2010. In April 2011, the dyspnea progressed to appear during even low levels of exertion. Echocardiogram detected prosthetic aortic valve stenosis with an ejection fraction of 50%. The patient underwent aortic valve replacement in May 2011. During surgery, the patient had an aortic dissection with loss of both coronary ostia as a complication. Aortic valve replacement was performed and a Bentall and Bono procedure was implemented to reconstruct the aorta. The orifices of the coronary ostia were covered by the aortic tube and additional revascularization was performed by placing a saphenous vein graft to the right coronary artery and a 5 mm Gore-Tex graft to the left main (the Cabrol procedure). After 48 hours of surgery, due to persisting hemodynamic instability, the patient was taken to the cath lab to check the status of both coronary grafts.
A 67-year-old male presented with a history of smoking, aortic valve replacement in 1995, and dyspnea on exertion beginning in 2010. In April 2011, the dyspnea progressed to appear during even low levels of exertion. Echocardiogram detected prosthetic aortic valve stenosis with an ejection fraction of 50%. The patient underwent aortic valve replacement in May 2011. During surgery, the patient had an aortic dissection with loss of both coronary ostia as a complication. Aortic valve replacement was performed and a Bentall and Bono procedure was implemented to reconstruct the aorta. The orifices of the coronary ostia were covered by the aortic tube and additional revascularization was performed by placing a saphenous vein graft to the right coronary artery and a 5 mm Gore-Tex graft to the left main (the Cabrol procedure). After 48 hours of surgery, due to persisting hemodynamic instability, the patient was taken to the cath lab to check the status of both coronary grafts.
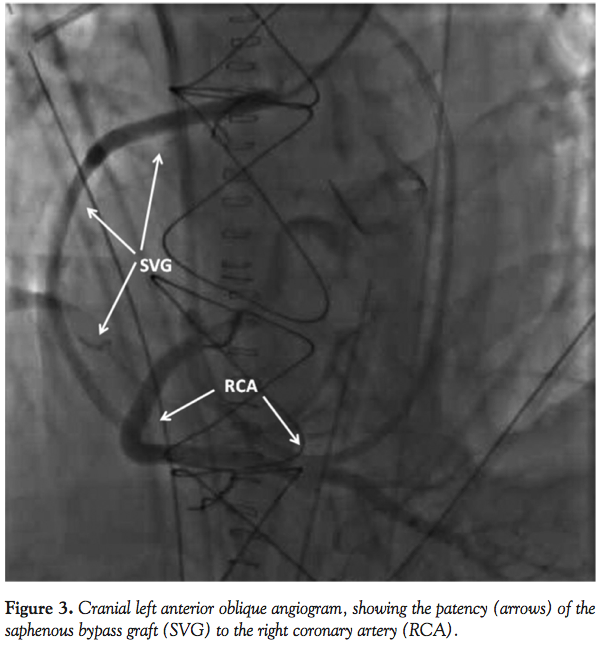 At the time of his presentation, the patient was found to have a blood pressure of 90/50 mm Hg and a heart rate of 110 bpm in sinus rhythm. Vasopressors and inotropes were adjusted and we started the procedure by placing a right radial artery 6 Fr sheath. During coronary angiography, the standard 5 Fr Judkins left (JL) 3.5 catheter failed to selectively engage the ostium of the Cabrol conduit, so we changed to an Amplatz left (AL) 2 catheter, which enabled a better cannulation. After extensive catheter manipulation, the 6 Fr AL 2 catheter engaged the Cabrol conduit ostium slightly better and the first angiograms showed a diffuse stenosis of the Gore-Tex graft to the left main starting at the site of the coronary aorta-anastomosis with impaired distal flow around the left coronary system (Figures 2A and 2B). Then, the saphenous bypass graft to the right coronary artery was cannulated, showing its patency (Figure 3).
At the time of his presentation, the patient was found to have a blood pressure of 90/50 mm Hg and a heart rate of 110 bpm in sinus rhythm. Vasopressors and inotropes were adjusted and we started the procedure by placing a right radial artery 6 Fr sheath. During coronary angiography, the standard 5 Fr Judkins left (JL) 3.5 catheter failed to selectively engage the ostium of the Cabrol conduit, so we changed to an Amplatz left (AL) 2 catheter, which enabled a better cannulation. After extensive catheter manipulation, the 6 Fr AL 2 catheter engaged the Cabrol conduit ostium slightly better and the first angiograms showed a diffuse stenosis of the Gore-Tex graft to the left main starting at the site of the coronary aorta-anastomosis with impaired distal flow around the left coronary system (Figures 2A and 2B). Then, the saphenous bypass graft to the right coronary artery was cannulated, showing its patency (Figure 3).
A detailed discussion was immediately held with the patient’s family members and a cardiac surgeon. His surgical risk was judged to be preclusive given the hemodynamic instability and the past thoracic surgery. Therefore, after weighing all of the risks and benefits, the decision was made to proceed with emergency percutaneous intervention (PCI) to rescue the Cabrol graft.
 We chose to undertake a PCI using a standard Extra Back-Up 3 guide catheter and a Pilot 50 wire (Abbott) to cross the lesion. A second Pilot 50 wire for a buddy-wire technique was used to improve support. Predilatation was performed using a semi-compliant 3.0 x 15 mm Apex balloon (Boston Scientific) prior to the insertion of two bare-metal stents (5.0 x 20 mm and 4.0 x 8 mm Liberte; Boston Scientific) that were overlapped and postdilated using a 4.5 x 10 mm Dura Star non-compliant balloon (Cordis). At the time of the procedure, neither intravascular ultrasound (IVUS) nor optical coherence tomography (OCT) were available, so the stent size was selected according to the 5 mm graft diameter reported by the surgical team in the postsurgical notes and the reference diameter measured by quantitative coronary angiography (QCA). Unfortunately, optimal stent apposition and sizing couldn’t be determined by an imaging modality. An excellent angiographic result was achieved post procedure, with no residual stenosis and a TIMI grade 3 flow (Figures 4A and 4B). The patient was transferred to the intensive care unit in a hemodynamically stable condition. At the time of catheterization, only aspirin had been administered as antiplatelet therapy; as a result, the patient was loaded with 600 mg of clopidogrel. Given the uncertain etiology for the stenosis, our patient was placed on the standard medical regimen for atherosclerotic coronary artery disease, including aspirin, clopidogrel, atorvastatin, and a beta-blocker. The patient evolved satisfactorily and was extubated 2 weeks post procedure; unfortunately, he died 2 months after the procedure secondary to infectious lung disease.
We chose to undertake a PCI using a standard Extra Back-Up 3 guide catheter and a Pilot 50 wire (Abbott) to cross the lesion. A second Pilot 50 wire for a buddy-wire technique was used to improve support. Predilatation was performed using a semi-compliant 3.0 x 15 mm Apex balloon (Boston Scientific) prior to the insertion of two bare-metal stents (5.0 x 20 mm and 4.0 x 8 mm Liberte; Boston Scientific) that were overlapped and postdilated using a 4.5 x 10 mm Dura Star non-compliant balloon (Cordis). At the time of the procedure, neither intravascular ultrasound (IVUS) nor optical coherence tomography (OCT) were available, so the stent size was selected according to the 5 mm graft diameter reported by the surgical team in the postsurgical notes and the reference diameter measured by quantitative coronary angiography (QCA). Unfortunately, optimal stent apposition and sizing couldn’t be determined by an imaging modality. An excellent angiographic result was achieved post procedure, with no residual stenosis and a TIMI grade 3 flow (Figures 4A and 4B). The patient was transferred to the intensive care unit in a hemodynamically stable condition. At the time of catheterization, only aspirin had been administered as antiplatelet therapy; as a result, the patient was loaded with 600 mg of clopidogrel. Given the uncertain etiology for the stenosis, our patient was placed on the standard medical regimen for atherosclerotic coronary artery disease, including aspirin, clopidogrel, atorvastatin, and a beta-blocker. The patient evolved satisfactorily and was extubated 2 weeks post procedure; unfortunately, he died 2 months after the procedure secondary to infectious lung disease.
Discussion
We report on the first case of a successful transradial percutaneous intervention though a Cabrol graft. Successful stenting of the graft-coronary anastomosis has been performed in 4 previously reported cases.3,7-9 However, all of them were performed through the femoral approach. Nowadays, the transradial approach has proven to decrease bleeding complications and therefore mortality attributable to them in experienced series. In our center, the transradial approach is routinely performed in 80% of cases and this case was no exception.
Engaging the Cabrol graft through the radial approach is similar to that used for saphenous vein grafts, and the location of the graft in an individual patient will determine the catheter used. In this case, we chose the Extra Back-Up catheter because it is easier to manipulate when attempting to reach high and anterior anatomical locations through the radial approach. Once you cannulate selectively the ostium of the graft, this catheter gives you more support, facilitating the advancement of the material, which is one important factor in a transradial angioplasty.
Even still, the technical challenges of the approach itself and the special cases such as this one involve more patience and skill. To increase our chances of technical success, we took into account several important considerations:
- Cabrol graft is typically attached to the aortic graft anteriorly and near the coronary that is involved.8 During cardiac catheterization, an initial aortogram sometimes helps locate the graft and select the best catheter for cannulation. However, in this particular case, it did not turn out to be very useful.
- We employed the buddy-wire technique10 to increase support and firm up the trajectory of the artery graft junction.
- The anchoring balloon technique11 was used to increase the coaxiality of the catheter and graft, which enabled an easier advancement of the first stent.
- Finally, we used the antegrade trapping-wire technique12 to stabilize the advancement of the second stent, thus satisfactorily completing the procedure.
We reiterate that, even though the Cabrol technique is only rarely used in contemporary surgical repair of the thoracic ascending aorta, when encountering a patient who has undergone coronary reimplantation using the Cabrol technique, clinicians should be aware of possible postoperative complications (such as stenosis), because development of stenosis at the coronary-Cabrol site graft is potentially catastrophic.
Due to the patient’s surgical risk after a Cabrol procedure, percutaneous revascularization of Cabrol-coronary lesions may be safer with much lower periprocedural risks than a repeat surgical intervention, perhaps making it the procedure of choice. Cardiologists should be familiar with this anatomic correction as well as the feasibility of a percutaneous intervention through the Cabrol graft.
References
- Bentall H, De Bono A. A technique for complete replacement of the ascending aorta. Thorax. 1968;23(4):338-339.
- Cabrol C, Pavie A, Gandjbakhch I, et al. Complete replacement of the ascending aorta with reimplantation of the coronary arteries: new surgical approach. J Thorac Cardiovasc Surg. 1981;81(2):309-315.
- Wells T, Kapoor A. Percutaneous coronary intervention through a Cabrol composite graft. Int J Cardiol. 2007;116(2):E44-E45.
- Mestres CA, Betriu A, Pomar JL. Occlusion of the coronary perfusion graft: an exceptional complication after reconstruction of the ascending aorta with the Cabrol technique. J Thorac Cardiovasc Surg. 1989;98(2):302-303.
- Madhusoodanan KP, Prakash MN, Chawla S, et al. Images in cardiology: Cabrol perfusion graft. Clin Cardiol. 2000;23(3):216-217.
- Coram R, George Z, Breall J. Percutaneous intervention through a Cabrol composite graft. Catheter Cardiovasc Interv. 2005;66(3):356-359.
- Hussain F, Ducas J, Gosal T. Emergent percutaneous intervention with a drug-eluting stent of a Cabrol graft-to-left main anastomosis during a non-ST elevation infarction in a patient with Marfan’s syndrome. J Invasive Cardiol. 2006;18(9):E250-E252.
- Hoskins MH, Kacharava AG, Green TF, et al. Percutaneous intervention of Cabrol graft-left main anastomosis during acute myocardial infarction. Int J Cardiol. 2010;140(2):E27-E29.
- Hagspiel K, Spinosa D, Angle J, et al. CT findings following the Cabrol composite graft procedure. Comput Assist Tomogr. 2001;25(4):563-568.
- Rigattieri S, Hamon M, Grollier G. The buddy wire technique is useful in transradial coronary stenting of complex, calcified lesions: report of three cases. J Invasive Cardiol. 2005;17(7):376-377.
- Wagatsuma K. Anchor balloon technique for very tortuous lesions by transradial coronary intervention. Ind Heart J. 2008;60(1 Suppl A):A42-A44.
- Liu SC, Tseng CD. Trap wire technique — A new technique improves device deliverability during complex percutaneous coronary intervention. J Taiwan Cardiovasc Interv. 2011;2:36-40.
_________________________________________________________
From the Interventional Cardiology Department, Instituto Nacional de Cardiología “Ignacio Chávez,” México City, Mexico.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 26, 2012, provisional acceptance given May 10, 2012, final version accepted May 16, 2012
Address for correspondence: Dr Jhonathan Uribe González, Interventional Cardiology Department, Instituto Nacional de Cardiología “Ignacio Chávez,” Juan Badiano No. 1 Colonia Sección XVI, Delegación Tlalpan, CP 14080, México City, Mexico. Email: ljhonathanug@hotmail.com









