

The Efficacy and Safety of the "Hybrid" Approach to Coronary Chronic Total Occlusions: Insights From a Contemporary Multicenter US Registry and Comparison With Prior Studies
Abstract: Background. Percutaneous coronary intervention (PCI) for chronic total occlusion (CTO) is challenging and has been associated with low success rates. However, recent advancements in equipment and the flexibility to switch between multiple technical approaches during the same procedure (“hybrid” percutaneous algorithm) have dramatically increased the success of CTO-PCI. We sought to compare the contemporary procedural outcomes of hybrid CTO-PCI with previously published CTO-PCI studies. Methods. The procedural outcomes of 497 consecutive CTO-PCIs performed between January 2012 and August 2013 at five high-volume centers in the United States were compared with the pooled success and complication rates reported in 39 prior CTO-PCI series that included ≥100 patients and were published after 2000. Results. The baseline clinical and angiographic characteristics of the study patients were comparable to those of previous studies. Technical and procedural success was achieved in 455 cases (91.5%) and 451 cases (90.7%), respectively, and were significantly higher than the pooled technical and procedural success rates from prior studies (76.5%, P<.001 and 75.2%, P<.001, respectively). Major procedural complications occurred in 9/497 patients (1.8%) overall and included death (2 patients), acute myocardial infarction (5 patients), repeat target vessel PCI (1 patient), and tamponade requiring pericardiocentesis (2 patients). The incidence of major complications was similar to that of prior studies (pooled rate 2.0%; P=.72). Conclusion. Use of the hybrid approach to CTO-PCI is associated with higher success and similar complication rates compared to prior studies, supporting its expanded use for treating these challenging lesions.
J INVASIVE CARDIOL 2014;26(9):427-432
Key words: percutaneous coronary interventions, coronary obstructions
______________________________________
Percutaneous coronary intervention (PCI) of chronic total occlusions (CTOs) has traditionally been limited by relatively low success rates,1 mainly due to failure to cross the occlusion with a guidewire.2 In the past decade, several techniques have been developed to improve CTO-PCI outcomes, such as the retrograde approach3-5 and antegrade dissection and reentry.6,7 However, most CTO operators have limited themselves to a single crossing approach per procedure mainly due to contrast and radiation exposure limitations. More recently, the “hybrid” approach to CTO-PCI (Figure 1) was described, which assesses the angiographic characteristics of the occlusion to provide a standardized and reproducible method for crossing CTOs.8-12 The hybrid algorithm uses all available techniques (antegrade, retrograde, true-to-true lumen crossing, or reentry) tailored to the specific case in the most safe, effective, and efficient way.8-10 As a result, it provides the operator with the flexibility to apply multiple modes of intervention during the same procedure, increasing chances of successful revascularization and sparing the need for subsequent hospitalization for a repeat procedure. The goal of the present study was to examine contemporary outcomes with the hybrid approach to CTO-PCI and compare them to those reported in prior published studies. We hypothesized that the hybrid approach to CTO-PCI would be associated with higher technical and procedural success rates and similar periprocedural major complications.
Methods
Hybrid CTO-PCI patients. We collected the clinical and angiographic characteristics and procedural outcomes of patients undergoing hybrid CTO-PCI between January 2012 and August 2013 at five high-volume CTO-PCI centers in the United States: Appleton Cardiology, Appleton Wisconsin; Piedmont Heart Institute, Atlanta Georgia; St Joseph Medical Center, Bellingham Washington; St Luke’s Health System’s Mid-America Heart Institute, Kansas City, Missouri; and VA North Texas Healthcare System, Dallas, Texas. A single operator performed all CTO procedures in two centers (Appleton Cardiology, St Joseph Medical Center), whereas in the other centers CTO procedures were performed by high-volume operators or operators who worked with a high-volume operator. Data from 497 CTO procedures were collected both prospectively and retrospectively using a dedicated centralized database (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention [PROGRESS CTO], Clinicaltrials.gov Identifier: NCT02061436).The study was approved by each center’s Institutional Review Board.
All procedures were performed by operators with significant expertise in CTO PCI using the hybrid approach. The first step in the hybrid algorithm is the performance of dual injection to assess four key angiographic characteristics: (1) proximal cap ambiguity; (2) quality of the vessel distal to the occlusion; (3) lesion length; and (4) presence of adequate collateral vessels. Initial antegrade wire escalation is favored for <20 mm-long lesions, whereas antegrade dissection and reentry is favored for ≥20 mm-long lesions. An initial retrograde (primary retrograde) approach is favored for lesions with ambiguous proximal cap, diffuse distal disease, and bifurcation at the distal cap, when appropriate collateral vessels are present. Early change of crossing strategy is recommended if the initially selected crossing strategy is unsuccessful or if no significant progress is achieved within a short period of time.8-12
Literature review. We performed a comprehensive search of the Pubmed and Cochrane Library databases for manuscripts on CTO-PCI. Bibliographies of the retrieved studies were searched by hand for other relevant studies. Human studies in English published between January 2000 and August 2013 were included if they reported technical or procedural success and complication rates from ≥100 consecutive CTO-PCI cases. Series that included non-consecutive CTO-PCI cases based on the use of a specialized technique (such as retrograde or dissection/reentry only) were excluded. Review articles, letters to the editor, case reports, and studies in which procedural complications could not be accurately assessed from the published manuscript were also excluded. A list of the included studies is shown in Supplemental Table 1 (available online at www.invasivecardiology.com). The pooled technical and procedural success and complication rates were calculated from the above studies in accordance to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines.13 Baseline clinical and angiographic characteristics as well as CTO-PCI efficiency data (fluoroscopy times, radiation exposure, and contrast administration) could not be pooled due to the lack of raw data. The authors of the present manuscript developed the hybrid approach and have published all related literature to date; hence, we are fairly certain that the hybrid approach was not used in prior reports. Moreover, each published study was carefully evaluated to ascertain that the hybrid approach was not used.
Definitions. Chronic total occlusions were defined as coronary obstructions with Thrombolysis in Myocardial Infarction (TIMI) flow grade 0 of at least 3-month duration. Estimation of the occlusion duration was based on first onset of anginal symptoms, prior history of myocardial infarction in the target vessel territory, or comparison with a prior angiogram. Technical success was defined as angiographic evidence of <30% residual stenosis with restoration of TIMI 3 antegrade flow in the CTO target vessel.14 Procedural success was defined as technical success with no procedural major adverse cardiac event (MACE), including death, Q-wave myocardial infarction (troponin or creatine kinase leak was not classified as a major complication as it often occurs transiently post CTO-PCI and resolves spontaneously), recurrent cardiac symptoms requiring repeat target vessel PCI or coronary artery bypass surgery (CABG), cardiac tamponade requiring pericardiocentesis or surgery, and stroke before hospital discharge. Major bleeding was defined as bleeding causing hemoglobin drop ≥3 g/dL or bleeding requiring transfusion or surgical intervention. Vascular access complications included major bleeding from the access site (see above) or other complication requiring surgical intervention.
Statistical analysis. Continuous data were summarized as mean ± standard deviation for normally distributed data or median and interquartile range (IQR) for non-normally distributed data, and compared using t-test or Wilcoxon rank-sum test as appropriate. Categorical data were presented as frequencies or percentages and compared using chi square or Fisher’s exact test, as appropriate. A two-sided P-value of <.05 was considered statistically significant. Analyses were performed using JMP version 9.0 (SAS Institute).
Results
Clinical and angiographic characteristics. Between January 2012 and August 2013, a total of 497 patients underwent hybrid CTO-PCI at the 5 participating centers. The clinical and baseline angiographic characteristics 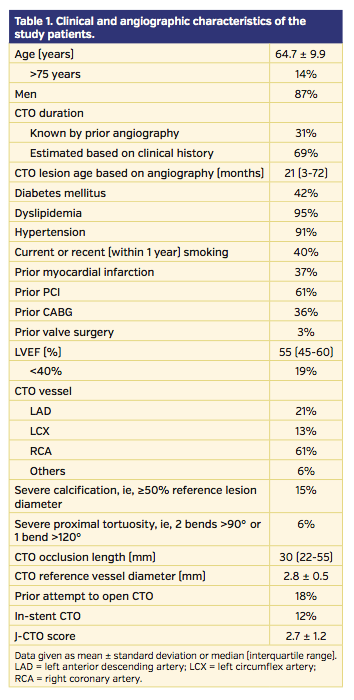 are presented in Table 1. Mean age was 64.7 ± 9.9 years and most patients (87%) were men, with high frequency of diabetes mellitus (42%), prior myocardial infarction (37%), and prior CABG (36%). All CTO target vessels (except one in a saphenous vein graft) were in a native coronary vessel. A prior CTO-PCI attempt had been performed in 18% of cases. The target CTO vessel was the right coronary artery in 61% of patients, followed by the left anterior descending (21%) and left circumflex artery (13%). The median visually estimated CTO occlusion length was 30 mm (IQR, 22-55 mm) and CTO reference vessel diameter was 2.8 ± 0.5 mm. Median occlusion duration was 21 months (IQR, 3 to 72 months).
are presented in Table 1. Mean age was 64.7 ± 9.9 years and most patients (87%) were men, with high frequency of diabetes mellitus (42%), prior myocardial infarction (37%), and prior CABG (36%). All CTO target vessels (except one in a saphenous vein graft) were in a native coronary vessel. A prior CTO-PCI attempt had been performed in 18% of cases. The target CTO vessel was the right coronary artery in 61% of patients, followed by the left anterior descending (21%) and left circumflex artery (13%). The median visually estimated CTO occlusion length was 30 mm (IQR, 22-55 mm) and CTO reference vessel diameter was 2.8 ± 0.5 mm. Median occlusion duration was 21 months (IQR, 3 to 72 months).
Procedural techniques and outcomes. Technical success and procedural success were 455/497 (91.5%) and 451/497 (90.7%), respectively (Table 2). The final successful CTO crossing strategy was antegrade in 41%, retrograde in 32%, and antegrade dissection/reentry in 28%. The retrograde approach was used in 218 patients (44%) with 86% technical and 85% procedural success and 3.2% incidence of MACE. Stents were 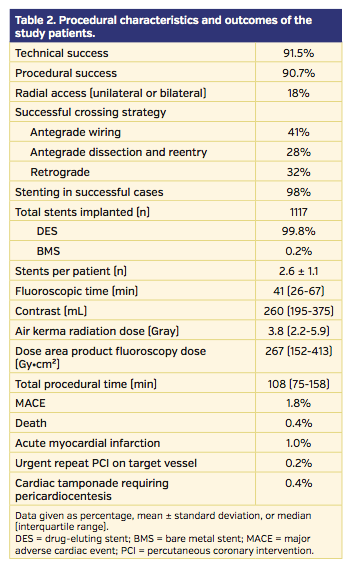 implanted in 98% of successful cases, and were mainly drug-eluting stents (99.8%). Median contrast volume and fluoroscopy time were 260 mL (IQR, 195-375 mL) and 41 min (IQR, 26-67 min), respectively. Radial access (unilateral or bilateral) was used in 18% of the CTO-PCI cases.
implanted in 98% of successful cases, and were mainly drug-eluting stents (99.8%). Median contrast volume and fluoroscopy time were 260 mL (IQR, 195-375 mL) and 41 min (IQR, 26-67 min), respectively. Radial access (unilateral or bilateral) was used in 18% of the CTO-PCI cases.
Major adverse cardiac events occurred in 8 patients (1.8%), as follows: death (2 patients), acute myocardial infarction (5 patients), urgent target vessel revascularization with PCI (1 patient) and cardiac tamponade requiring pericardiocentesis (2 patients). No patient experienced a stroke and no patient required emergency coronary artery bypass graft surgery. Perforation (not resulting in MACE) was the most common procedural adverse effect (3.2%), followed by dissection (2.4%) and vascular access complications (1.6%).
Comparison with prior studies. Database and bibliography search retrieved 448 publications, of which 409 were excluded because they did not directly report success and complication rates or only studied a specific interventional approach (such as retrograde), thus leaving 39 studies that were included in the present analysis. Overall success ranged between 54.3% and 88.9% (Supplemental Table 1).
The technical and procedural success rates in our study were significantly higher than the pooled success rates reported in prior studies (technical success 91.5% vs 76.5%, P<.001 and procedural success 90.7% vs 75.2%, P<.001). Technical success continued to be higher, even when analyses were limited to the most recent studies published between 2010 and 2013 (91.5% vs 76.4%; P<.001).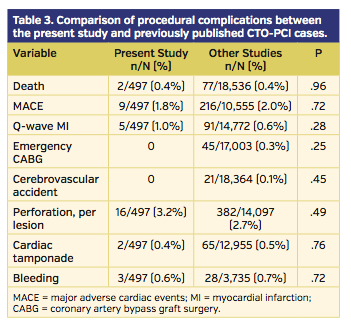
Complication rates from previous studies were similar to our study (Table 3): MACE occurred in 2.0% of patients, 0.6% of patients had Q-wave myocardial infarction, 0.3% required emergent coronary artery bypass graft surgery, and 1.2% had a stroke. Perforations occurred in 2.7% of the lesions and were the most common procedural adverse effect.
Discussion
The main finding of our multicenter registry is that the hybrid approach to CTO-PCI is associated with significantly higher success and similar complication rates compared to published CTO-PCI series.
The hybrid approach was developed through the combined experiences of high-volume North American CTO-PCI operators aiming to open the occluded vessel, using all feasible techniques (antegrade, retrograde, true-to-true lumen crossing or reentry) in the most safe, effective, and efficient way.8 The basic underlying principle of the hybrid approach is that no single procedural crossing strategy should be pursued to exhaustion, but an alternative strategy should be attempted if a given crossing strategy does not progress.10 Hence, the hybrid CTO-PCI strategy places emphasis not only on procedural success, but also on procedural efficiency and forms the basis of contemporary CTO program development.15 The optimal techniques and technologies are applied during the specific time of the procedure when they are most likely to be effective. The practical ramifications of this method are that changes of strategy should occur very early, and often cycle rapidly, to maximize the likelihood of early successful crossing.
To the best of our knowledge, this is the first published series of the hybrid approach to CTO-PCI. A “hybrid registry” of 144 cases performed at CTO-PCI workshops between January 2011 and October 2012 was 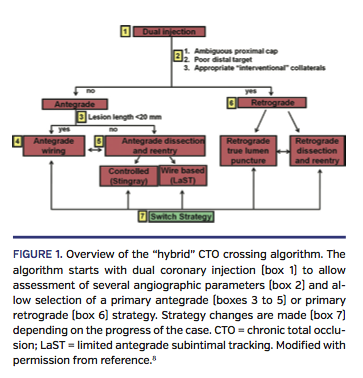 presented at the 2013 CTO Summit (New York, New York) demonstrating 94% procedural success, although lesion complexity was high (average J-CTO score was 2.3 and 46% of lesions had a J-CTO score >3). Similar to that registry, our technical and procedural success rates were 91.5% and 90.7%, respectively.
presented at the 2013 CTO Summit (New York, New York) demonstrating 94% procedural success, although lesion complexity was high (average J-CTO score was 2.3 and 46% of lesions had a J-CTO score >3). Similar to that registry, our technical and procedural success rates were 91.5% and 90.7%, respectively.
This is the first all-comer publication reporting >90% success rates in CTO-PCI (Supplemental Table 1 and Figure 1). Such high success rates have thus far only been reported for retrograde CTO-PCI series in Japan. Kimura et al reported technical and procedural success of 92.4% and 90.6%, respectively, among 224 patients treated with the retrograde approach in 43 centers.16 Tsuchikane et al reported 98.9% success (in 92/93 cases) in a two-operator series.17 Rathore et al reported 100% success among 31 patients treated with intravascular-ultrasound guided reverse controlled antegrade and retrograde tracking and dissection (CART).18 Our results extend the high success rates to an unselected, highly complex CTO-PCI population with very high frequency of prior coronary artery bypass graft surgery (36%), which has been associated with lower CTO-PCI success rates.19
The prior collective experience of many of the centers participating in the current registry was recently published, showing 85.4% technical success among 1361 patients who were treated before the routine application of the hybrid approach.20 Hence, although overall CTO-PCI success rates have been modestly increasing over time (Figure 1), use of the hybrid approach to CTO-PCI has resulted in a significant and clinically meaningful increase in procedural success. Importantly, this was achieved without incurring a penalty in terms of procedural complications. 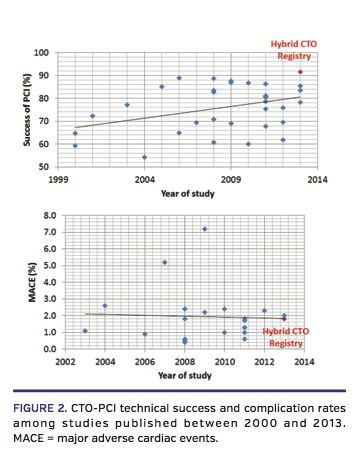
Study limitations. Our study has important limitations. It was observational without independent review of the coronary angiograms by an angiographic core laboratory and without adjudication of the clinical outcomes by a clinical events committee. However, adjudication would be unlikely to affect reporting of death, urgent repeat revascularization, and the need for pericardiocentesis. Serial cardiac biomarker measurements were not performed and only Q-wave myocardial infarction was recorded as part of the study. All participating centers have established CTO-PCI programs15 with expertise in all crossing techniques that are part of the hybrid algorithm; hence, the outcomes observed in the study may not be achievable by less experienced centers. Furthermore, operator experience can significantly increase success rates of CTO-PCI and this relation has been previously described.4 Finally, long-term clinical or angiographic follow-up was not performed.
Conclusion
Our findings have important implications for everyday clinical practice. First, they suggest that the efficacy of CTO-PCI has significantly improved; hence, the presence of a CTO may not necessarily need to be linked with lower level recommendation for PCI in the appropriateness use criteria for coronary revascularization.21 Second, they suggest that such results can be achieved across various hospitals and operators. Third, they demonstrate that high success can be achieved without incurring more complications,1 which is important for an elective procedure, such as CTO-PCI.
References
- Patel VG, Brayton KM, Tamayo A, et al. Angiographic success and procedural complications in patients undergoing percutaneous coronary chronic total occlusion interventions: a weighted meta-analysis of 18,061 patients from 65 studies. JACC Cardiovasc Interv. 2013;6(2):128-136.
- Garcia S, Abdullah S, Banerjee S, Brilakis ES. Chronic total occlusions: patient selection and overview of advanced techniques. Curr Cardiol Rep. 2013;15(2):334.
- Brilakis ES, Grantham JA, Thompson CA, et al. The retrograde approach to coronary artery chronic total occlusions: a practical approach. Catheter Cardiovasc Interv. 2012;79(1):3-19.
- Thompson CA, Jayne JE, Robb JF, et al. Retrograde techniques and the impact of operator volume on percutaneous intervention for coronary chronic total occlusions an early U.S. experience. JACC Cardiovasc Interv. 2009;2(9):834-842.
- Karmpaliotis D, Michael TT, Brilakis ES, et al. Retrograde coronary chronic total occlusion revascularization: procedural and in-hospital outcomes from a multicenter registry in the United States. JACC Cardiovasc Interv. 2012;5(12):1273-1279.
- Michael TT, Papayannis AC, Banerjee S, Brilakis ES. Subintimal dissection/reentry strategies in coronary chronic total occlusion interventions. Circ Cardiovasc Interv. 2012;5(5):729-738.
- Whitlow PL, Burke MN, Lombardi WL, et al. Use of a novel crossing and re-entry system in coronary chronic total occlusions that have failed standard crossing techniques: results of the FAST-CTOs (Facilitated Antegrade Steering Technique in Chronic Total Occlusions) trial. JACC Cardiovasc Interv. 2012;5(4):393-401.
- Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5(4):367-379.
- Thompson CA. The hybrid approach for percutaneous revascularization of coronary chronic total occlusions. Interv Cardiol Clin. 2012;1:349-353.
- Sabbagh AE, Banerjee S, Brilakis ES. Illustration of the “hybrid” approach to chronic total occlusion crossing. Interv Cardiol. 2012;4:639-643.
- Michael TT, Mogabgab O, Fuh E, et al. Application of the “hybrid approach” to chronic total occlusion interventions: a detailed procedural analysis. J Interv Cardiol. 2014;27(1):36-43.
- Brilakis ES, ed. Manual of Coronary Chronic Total Occlusion Interventions. A Step-By-Step Approach. Waltham, MA: Elsevier; 2013.
- Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012.
- Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58(24):2550-2583.
- Karmpaliotis D, Lembo N, Kalynych A, et al. Development of a high-volume, multiple-operator program for percutaneous chronic total coronary occlusion revascularization: procedural, clinical, and cost-utilization outcomes. Catheter Cardiovasc Interv. 2013;82(1):1-8.
- Kimura M, Katoh O, Tsuchikane E, et al. The efficacy of a bilateral approach for treating lesions with chronic total occlusions the CART (controlled antegrade and retrograde subintimal tracking) registry. JACC Cardiovasc Interv. 2009;2(11):1135-1141.
- Tsuchikane E, Katoh O, Kimura M, Nasu K, Kinoshita Y, Suzuki T. The first clinical experience with a novel catheter for collateral channel tracking in retrograde approach for chronic coronary total occlusions. JACC Cardiovasc Interv. 2010;3(2):165-171.
- Rathore S, Katoh O, Tuschikane E, Oida A, Suzuki T, Takase S. A novel modification of the retrograde approach for the recanalization of chronic total occlusion of the coronary arteries intravascular ultrasound-guided reverse controlled antegrade and retrograde tracking. JACC Cardiovasc Interv. 2010;3(2):155-164.
- Michael TT, Karmpaliotis D, Brilakis ES, et al. Impact of prior coronary artery bypass graft surgery on chronic total occlusion revascularisation: insights from a multicentre US registry. Heart. 2013;99(20):1515-1518.
- Michael TT, Karmpaliotis D, Brilakis ES, et al. Procedural outcomes of revascularization of chronic total occlusion of native coronary arteries (from a Multicenter United States Registry). Am J Cardiol. 2013;112(4):488-492.
- Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 Appropriate use criteria for coronary revascularization focused update: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2012;59(9):857-881.
______________________________________
From 1VA North Texas Healthcare System and UT Southwestern Medical Center, Dallas, Texas; 2Columbia University, New York, New York; 3Appleton Cardiology, Appleton, Wisconsin; 4PeaceHealth Cardiology, Bellingham, Washington; 5Mid America Heart Institute, Kansas City, Missouri; 6Piedmont Hospital, Atlanta, Georgia; 7Minneapolis VA Healthcare System and University of Minnesota, Minneapolis, Minnesota; and 8Yale University School of Medicine, New Haven, Connecticut.
Acknowledgment: Study data were collected and managed using REDCap electronic data capture tools hosted at University of Texas Southwestern Medical Center.1 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources.
1Paul A. Harris, Robert Taylor, Robert Thielke, Jonathon Payne, Nathaniel Gonzalez, Jose G. Conde, Research electronic data capture (REDCap) - A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381.
Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award NumberUL1TR001105. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Karmpaliotis is on the speaker’s bureau for Abbott Vascular, Boston Scientific, Asahi, and Medtronic. Dr Alaswad reports consulting fees from Terumo and Boston Scientific; consultant (non-financial capacity) for Abbott Laboratories. Dr Lombardi reports stock with Bridgepoint Medical; honoraria from Abbott Vascular, Medtronic, and Terumo; consultancy with Abbott Vascular, Bridgepoint Medical, and Medtronic. Dr Grantham reports speaking fees, consulting, and honoraria from Boston Scientific, Asahi Intecc; research grants from Boston Scientific, Asahi Intecc, Abbott Vascular, Medtronic. Dr Lembo is a member of the speaker’s bureau at Medtronic; advisory board for Abbott Vascular and Medtronic. Dr Kandzari reports research/grant support and consulting honoraria from Boston Scientific and Medtronic Cardiovascular; research/grant support from Abbott Vascular. Dr Garcia reports consulting fees from Medtronic. Dr Banerjee reports research grants from Gilead and the Medicines Company; consultant/speaker honoraria from Covidien and Medtronic; ownership in MDCare Global (spouse); intellectual property in HygeiaTel. Dr Thompson is a consultant for Abbott Vascular, Bridgepoint, Terumo, Volcano; reports equity in Bridgepoint Medical. Dr Brilakis reports consulting honoraria/speaker fees from Sanofi, Janssen, St Jude Medical, Terumo, Asahi, Abbott Vascular, Elsevier, and Boston Scientific; research grant from Guerbet; spouse is an employee of Medtronic. The remaining authors report no disclosures.
Manuscript submitted February 10, 2014, provisional acceptance given February 19, 2014, final version accepted March 18, 2014.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Dallas VA Medical Center (111A), 4500 South Lancaster Road, Dallas, TX 75216. Email: esbrilakis@gmail.com









