

Endovascular Treatment of Acute Thoracic Aortic Syndromes with a Proximal Landing Zone Extension Strategy: Procedural and Follow-up Results
ABSTRACT: Purpose. To report the procedural and long-term follow-up data (mean, 43 ± 29 months; range, 12–90 months) of endovascular stent grafting (ESG) of acute thoracic aortic syndromes (ATAS) with a proximal landing zone extension strategy. Methods. From November 1999 to May 2008, 26 patients (25 males, 1 female; mean age, 57.9 ± 17 years) with ATAS underwent ESG at our institution. Underlying pathologies were: penetrating aortic ulcer (n = 7); rupture of a descending aorta aneurysm (n = 5), post-traumatic false aneurysm (n = 5); acute type B dissection (n = 6) and traumatic descending aorta transection (n = 3). Results. ESG was performed successfully in all patients. In 5 patients (19%), an extra-anatomic revascularization of the supra-aortic vessels was performed. In 19 patients (73%), overstenting of the left subclavian artery, without preliminary revascularization, was performed. The mean proximal landing zone length was 57 ± 19 mm. No intraprocedural deaths occurred; 3 patients died postoperatively (1 from an unrelated cause, 1 from a myocardial infarction and 1 for the sequelae of an ischemic stroke). One patient underwent cardiac surgery for post-procedural retrograde type-A dissection. Follow up involved a computed tomography (CT) scan at 1, 3, 6 and 12 months, then yearly thereafter. At follow up, no deaths or major complications occurred. The CT scans revealed 1 small type-IB endoleak at 1 year. Conclusion. In ATAS patients treated with ESG, the extension of the proximal landing zone, despite the need of subclavian coverage or hybrid procedures, is associated with an immediate procedural outcome and low morbidity at follow-up.
J INVASIVE CARDIOL 2011;23:187–192
____________________________________
Endovascular stent-grafting (ESG) has emerged in the last decade as a less invasive and potentially safer alternative to surgery in the treatment of diseases of the thoracic aorta.1–8 The endovascular technique avoids thoracotomy or sternotomy2,6 and is limited only by severe atherosclerosis of the ilio-femoral axes.9 The lack of aortic clamping minimizes spinal and visceral hypoperfusion4 and does not negatively affect myocardial contractility.10,11 Furthermore, a lower dosage of heparin is required, compared to standard surgical treatment, reducing the risk of bleeding complications.2 Minimal invasivity is a primary requirement in the treatment of patients affected by acute thoracic aorta syndromes (ATAS), a spectrum of clinical conditions characterized by an acute lesion of the thoracic aortic wall with involvement of the media, including aortic type-B dissection, penetrating aortic ulcer, ruptured aortic aneurysm and traumatic aortic transection.12,13 Conventional surgical treatment has a mortality rate greater than 20%, peaking at up to 50% in the elderly14–17 due to the high-risk nature of this population, and in traumatic aortic transections, where lesions of multiple organs occur.18–21 Despite promising procedural results, further data on the long-term success of endovascular stent-grafting are required. A critical procedural factor for the long-term success of endovascular thoracic aorta procedures is represented by the detection of an appropriate proximal fixation zone, which sometimes requires the coverage of the ostia of the supra-aortic vessels. In this paper, we report a retrospective analysis of ESG, in a group of consecutive ATAS patients, where a proximal landing zone extension approach was used, reporting clinical and procedural results at an average of 43 ± 29 months of follow-up.
Methods
From November 1999 to May 2008, 26 patients (average age, 57.9 ± 17 years; range, 27–80 years) with ATAS and a high surgical risk according to the criteria of the American Society of Anesthesiology, underwent ESG at our institution. All patients complained of acute  chest pain or had a history of traumatic injury within 14 days of admission. Patients’ demographic and clinical characteristics are reported in Table 1. The underlying diseases were as follows: descending aorta or arch aneurysm rupture (n = 5); post-traumatic false aneurysm (n = 5); penetrating aortic ulcer (n = 7); acute type-B dissection (n = 6); and post-traumatic descending aortic rupture (n = 3). The patients with ruptured aortic aneurysm had a mean aortic diameter of 54.8 ± 7 mm. The 5 patients who were admitted for chest pain and a diagnosis of thoracic aorta false aneurysm had an anamnestic blunt chest trauma, due to a car accident, which occurred an average of 13 ± 11 years prior. In 3 of the 7 patients with penetrating aortic ulcer, the lesion was located in the aortic arch; in the other patients, it was located in the proximal descending aorta. Four patients, who were urgently admitted with an acute type-B dissection, presented with aortic rupture and left hemothorax, while 2 had bilateral renal perfusion supplied by the false lumen and elevated creatinine levels; the mean aortic diameter in these patients was 45 ± 18 mm. One of the 3 patients referred with multiple injuries and post-traumatic aortic transection had already undergone surgery for the treatment of a descending thoracic aorta aneurysm 7 years prior. Nine patients (35%) were treated immediately on admission due to aortic rupture with hemodynamic instability. Informed consent was obtained from each patient or from relatives when the patient was unable to give it. The authors conformed to institutional guidelines and those of the American Physiological Society.
chest pain or had a history of traumatic injury within 14 days of admission. Patients’ demographic and clinical characteristics are reported in Table 1. The underlying diseases were as follows: descending aorta or arch aneurysm rupture (n = 5); post-traumatic false aneurysm (n = 5); penetrating aortic ulcer (n = 7); acute type-B dissection (n = 6); and post-traumatic descending aortic rupture (n = 3). The patients with ruptured aortic aneurysm had a mean aortic diameter of 54.8 ± 7 mm. The 5 patients who were admitted for chest pain and a diagnosis of thoracic aorta false aneurysm had an anamnestic blunt chest trauma, due to a car accident, which occurred an average of 13 ± 11 years prior. In 3 of the 7 patients with penetrating aortic ulcer, the lesion was located in the aortic arch; in the other patients, it was located in the proximal descending aorta. Four patients, who were urgently admitted with an acute type-B dissection, presented with aortic rupture and left hemothorax, while 2 had bilateral renal perfusion supplied by the false lumen and elevated creatinine levels; the mean aortic diameter in these patients was 45 ± 18 mm. One of the 3 patients referred with multiple injuries and post-traumatic aortic transection had already undergone surgery for the treatment of a descending thoracic aorta aneurysm 7 years prior. Nine patients (35%) were treated immediately on admission due to aortic rupture with hemodynamic instability. Informed consent was obtained from each patient or from relatives when the patient was unable to give it. The authors conformed to institutional guidelines and those of the American Physiological Society.
Assessments. All patients underwent a 16-row or 64-row multidetector contrast computed tomography scan (MDCT) (Toshiba Aquilion, Toshiba Medical System, Tokyo, Japan). The diagnosis of the disease and its extension, as well as the localization and measurement of the proximal and distal landing zone and the measurement of aortic diameter were performed, based on 1 mm axial slices in combination with MPR images and 3-dimensional images generated from 1 mm-thin slices, with a 0.5 mm reconstruction interval (Vitrea 2 workstation, Vital Images Inc, Plymouth, Minnesota). A pre-operative supra-aortic vessel color duplex sonography was performed in every patient.
Procedures. All procedures were performed in the cardiac catheterization laboratory using a C-Arm Angiographic System (Philips Integris 3000 POLI C; Phillips Medical Systems, Seattle, Washington), with digital subtraction angiography (DSA) capability.
The procedures were performed under general anesthesia and with mechanical ventilation in most patients (20/26; 77%). Neuraxial block with spinal anesthesia was reserved to 6 patients (23%) with severe impairment of pulmonary function. Vascular access was obtained by cut-down of a surgically isolated femoral artery in 16 patients (78%). In 10 patients (38%), a fully percutaneous technique was performed, with closure of the arteriotomy obtained by 2 Prostar XL vascular hemostasis systems (Perclose, Abbott Laboratory Vascular Devices, Redwood Hills, California) positioned before the procedure (Pre-Close Technique). Right radial artery access was also obtained in all patients. After systemic heparinization (60 UI/kg), a calibrated pigtail catheter was advanced from the radial artery to the ascending aorta. A diagnostic DSA aortography was performed in order to have an angiographic view of the landing zones. The stent-graft diameter was chosen according to the aortic diameter (assessed by CT scan and angiography) with a 10–15% over-sizing. Arteriotomy of the femoral artery was performed and an appropriately sized sheath (22–27 French) was inserted. Through a 0.035-inch extra-stiff guidewire (BackUp Meier, Boston Scientific Corporation, Natick, Massachusetts), the stent-graft system was advanced into the thoracic aorta to the target segment. The appropriate positioning of the stent-graft was checked by DSA aortography. After induction of controlled hypotension by nitroprusside, the device was released under fluoroscopic guidance. Additional dilations with appropriately sized balloons were performed to obtain optimal apposition of the stent-graft to the aortic wall, with particular care at the proximal and distal necks. A DSA aortography was finally performed to confirm the correct positioning of the stent-graft and the absence of endovascular leaks and to assess the maintained patency of the supra-aortic trunks.
Supra-aortic vessel debranching. Five patients underwent an extra-anatomic revascularization of the brachiocephalic trunk and of the left common carotid artery before the endovascular procedure. In 2 patients with penetrating ulcer of the aortic arch, a carotid-carotid bypass with an 8-mm diameter Dacron graft through a bilateral latero-cervical incision was performed. After systemic heparinization (70 IU/kg), a bilateral latero-cervical incision on the medial border of the sternochleidomastoid muscle was performed and the common carotid arteries were isolated. The right common carotid artery was clamped and an end-to-side anastomosis with an 8 mm Gore-Tex conduit (W. L. Gore and Associates, Flagstaff, Arizona) was performed using a running suture. The left common carotid artery was consecutively clamped and transversely divided. The proximal part was sutured with 5-0 Prolene (Ethicon, Inc., Somerville, New Jersey). An end-to-end anastomosis of the left common carotid artery with the conduit was performed using a running suture with 6-0 Gore-Tex (W. L. Gore and Associates). The clamp was then removed; after hemostasis, the wound was closed in layers. One patient with penetrating ulcer of the arch and 2 patients with acute type-B dissection complicated by visceral malperfusion underwent supra-aortic vessel debranching by reimplantation of the brachiocephalic trunk and the left common carotid artery on a bifurcated Dacron graft anastomosed to the proximal descending aorta, with a mini-sternotomic approach. A bifurcated prosthesis was assembled by performing an end-to-side anastomosis of an 8 mm Intervascular prosthesis (W. L. Gore and Associates) on a 10 mm prosthesis, with a 5-0 Prolene running suture. A reverse-T ministernotomy in the second intercostal space was performed; the pericardium was opened and the epiaortic vessels isolated. After administration of heparin (60 IU/kg), the ascending aorta was tangentially clamped and a circular arteriotomy was performed. A proximal end-to-side anastomosis between the ascending aorta and the 10 mm prosthesis was performed with a 5-0 Prolene running suture. Next, a distal end-to-side anastomosis of the 10 mm prosthesis with the brachiocephalic trunk and an end-to-end anastomosis of the 8 mm prosthesis with the left common carotid artery were performed, using a 5-0 Prolene running suture. Finally, the brachiocephalic trunk and the left common carotid artery were ligated proximal to the anastomoses. In 1 patient, a revascularization of the left subclavian artery was performed using a trifurcated prosthesis (fabricated with an end-to-side anastomosis of two 8 mm Intervascular conduits to a 10 mm graft), with an additional end-to-side anastomosis to the left axillary artery. After hemostasis, the wound was closed in layers. All patients underwent AngioCT scan at discharge. The follow-up diagnostics included an AngioCT scan at 1, 3, 6 and 12 months, and once a year thereafter.
Results

All procedures were successfully performed. A total of 37 stent grafts were deployed: 22 Talent (Medtronic Vascular, Santa Rosa, California), 6 Valiant (Medtronic Vascular), 6 Relay (Bolton Medical España, Barcelona, Spain), 3 TAG (W. L. Gore and Associates). The procedural characteristics are reported in Table 2. Table 3 presents the characteristics of the stent-grafts employed in this study, including type, proximal landing zones,22 proximal landing zone length, and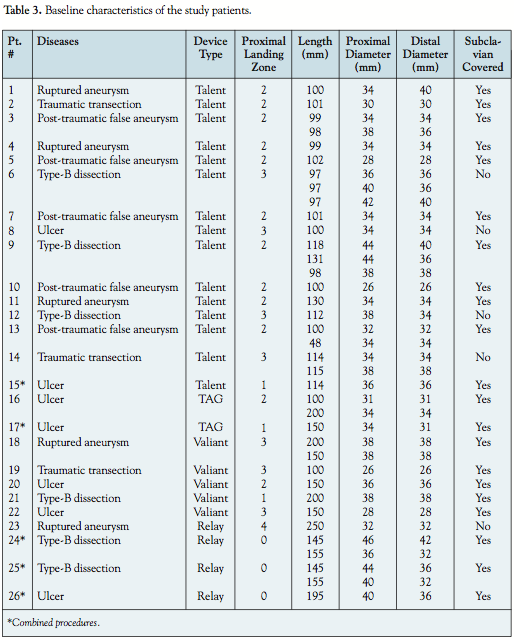 dimensions. Mean intensive care unit stay was 3.0 ± 4 days and mean hospital stay was 12 ± 7 days. In 9 patients (35%), hemo-transfusion was necessary. No intraprocedural deaths occurred. There were 3 post-operative deaths (hospital mortality, 11%). The first patient had a traumatic thoracic aortic transsection following a car accident, having reported multiple fractures and cranial trauma; he died in the first post-procedural day due to intracerebral bleeding. The second patient, treated for an acute type-B dissection with aortic rupture, died on post-procedural day 5 due to an acute myocardial infarction complicated by cardiogenic shock. Another patient, treated for a ruptured ulcer of the proximal descending aorta, died 27 days after the procedure due to the consequences of an ischemic stroke (the patient was already affected by lacunar ischemic encephalopathy), probably related to embolization of atherosclerotic debris from the aortic arch. A patient who underwent endovascular stent grafting of the arch and descending aorta due to an acute type-B dissection with aortic rupture and massive left pleural bleeding was complicated by a retrograde type-A dissection, requiring surgical treatment with ascending aorta and aortic root replacement with a composed valved conduit. In 1 patient, previously treated with bilateral common iliac artery stenting, during endograft advance, the left iliac stent was displaced in the abdominal aorta. The stent was recovered by contralateral arterial approach using a Goose Neck retrieval catheter (Boston Scientific). After placement of the endograft, the procedure was successfully completed with implantation of a peripheral polytetrafluoroethylene-covered stent (Jostent, Jomed International AB, Helsingborg, Sweden) in the left common iliac artery.
dimensions. Mean intensive care unit stay was 3.0 ± 4 days and mean hospital stay was 12 ± 7 days. In 9 patients (35%), hemo-transfusion was necessary. No intraprocedural deaths occurred. There were 3 post-operative deaths (hospital mortality, 11%). The first patient had a traumatic thoracic aortic transsection following a car accident, having reported multiple fractures and cranial trauma; he died in the first post-procedural day due to intracerebral bleeding. The second patient, treated for an acute type-B dissection with aortic rupture, died on post-procedural day 5 due to an acute myocardial infarction complicated by cardiogenic shock. Another patient, treated for a ruptured ulcer of the proximal descending aorta, died 27 days after the procedure due to the consequences of an ischemic stroke (the patient was already affected by lacunar ischemic encephalopathy), probably related to embolization of atherosclerotic debris from the aortic arch. A patient who underwent endovascular stent grafting of the arch and descending aorta due to an acute type-B dissection with aortic rupture and massive left pleural bleeding was complicated by a retrograde type-A dissection, requiring surgical treatment with ascending aorta and aortic root replacement with a composed valved conduit. In 1 patient, previously treated with bilateral common iliac artery stenting, during endograft advance, the left iliac stent was displaced in the abdominal aorta. The stent was recovered by contralateral arterial approach using a Goose Neck retrieval catheter (Boston Scientific). After placement of the endograft, the procedure was successfully completed with implantation of a peripheral polytetrafluoroethylene-covered stent (Jostent, Jomed International AB, Helsingborg, Sweden) in the left common iliac artery.
Long-term follow-up. During a mean follow-up time of 43 ± 29 months (range, 12–90 months), no deaths or major complications occurred. A follow up longer than 36 months was available in 13 patients (50%). The follow-up data are shown in Table 4. 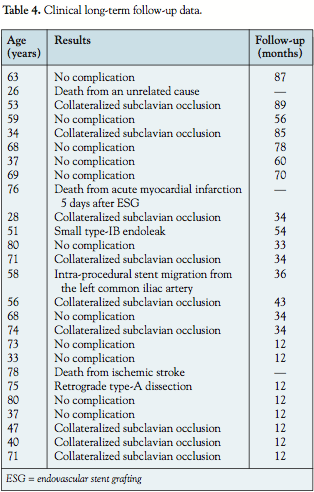 In 9 patients (35%), a collateralized occlusion of the left subclavian artery was observed; however, all patients were asymptomatic. We did not experience any cases of paraplegia. The patients who underwent combined procedures with extra-anatomic revascularization of the supra-aortic vessel had no neurological symptoms after the procedure. The imaging follow up showed a persistently good procedural result in the majority of cases; only 1 patient who was treated for a symptomatic post-traumatic false aneurysm had a small type-IB endoleak that was found at follow-up, without increase of the aneurysmatic sack; a conservative strategy was adopted, without further intervention, but with a closer follow up.
In 9 patients (35%), a collateralized occlusion of the left subclavian artery was observed; however, all patients were asymptomatic. We did not experience any cases of paraplegia. The patients who underwent combined procedures with extra-anatomic revascularization of the supra-aortic vessel had no neurological symptoms after the procedure. The imaging follow up showed a persistently good procedural result in the majority of cases; only 1 patient who was treated for a symptomatic post-traumatic false aneurysm had a small type-IB endoleak that was found at follow-up, without increase of the aneurysmatic sack; a conservative strategy was adopted, without further intervention, but with a closer follow up.
Discussion
ESG has replaced conventional surgery as the elective treatment for acute diseases of the thoracic aorta. The high procedural success rates and low mortality and morbidity rates associated with this technique, along with an acceptable incidence of paraplegia, have been reported in previous studies.1–8,23–35 The findings of our study confirmed these favorable outcomes and, importantly, long-term follow-up data over a mean period greater than 3 years demonstrated lasting results. Immediate success of the endovascular procedure in acute aortic syndromes relies on sealing the aortic rupture, exclusion of the aneurysm or ulcer or obliteration and thrombosis of a false lumen of dissection. In our series of patients, these goals were accomplished in 100% of the cases, without procedure-related deaths. Our in-hospital mortality rate of 11% is comparable with a mean mortality rate of about 10%, (range, 0–40%) which arises from different studies, with different patient populations,23–35 and with the 8% mortality rate reported in the Talent Thoracic Retrospective Registry.36 It should be noted that in the Eurostar and United Kingdom Thoracic Endograft Registries,37 a higher mortality rate was reported for emergency endovascular repair of degenerative aneurysms (28%) compared to acute type-B dissections (12%) or traumatic aortic lesions (6%). Interestingly, 20% of the participants in our study were found to have a ruptured descending aortic aneurysm, and none of these patients had died at the latest follow-up. Optimal anchoring of the stent-graft is a key factor for immediate and long-term success of endovascular procedures. The cranial extension of the proximal landing zone was the main technical feature of our experience, since even an apparently “healthy” aortic segment in these patients is not spared by disease and a longer neck could offer a more stable fixation of the stent-graft. As a result of this approach, the mean proximal landing zone length in this series of patients was 57 ± 20 mm, much longer than the minimum required length recommended by most manufacturers for the proximal fixation of the device. In the treatment of diseases of the descending aorta, the proximal extension of the landing zone was accomplished by intentional coverage of the left subclavian artery. Despite the lack of definitive agreement about this approach, with some reports validating its safety,38–42 and other authors recommending a preliminary subclavian revascularization,43,44 in our series of patients no clinical events occurred, though a subclavian occlusion was found in 9 patients (43%) at follow up. A good collateralization, provided by the contralateral vertebral artery, probably prevented vertebro-basilar ischemia and subclavian-steal symptoms; hence, the need for a pre-procedural evaluation of vertebral circulation, which in these acute patients was obtained by color duplex sonography. The proximal fixation at zone 2 (between the subclavian artery and the left common carotid artery)22 is associated in the literature with a low rate of type-I endoleak and device migration.45,46 The treatment of disease of the aortic arch is made troublesome by the multi-planar tortuosity of this aortic segment, which hinders an appropriate apposition of the endograft to the vascular wall. Oversizing of the device and aggressive post-dilatation could be possible solutions, but since the aortic wall is diffusely diseased, and also where it appears normal, this strategy could lead to retrograde dissections or pseudoaneurysms. Extension of the proximal landing zone is another possible strategy; in this case, an extra-anatomic revascularization of the supra-aortic vessels is mandatory. In 2 patients with symptomatic aortic ulcer located in the lesser curve of the aortic arch (zone 2), despite the high instability of this clinical condition, which leads to aortic rupture in 40% of the cases,47 we decided to revascularize the supra-aortic vessels prior to the endovascular procedure, in order to extend the proximal landing zone to zone 1 (proximal to the left common carotid artery).22 A carotid-carotid bypass was performed through a bilateral latero-cervical incision, avoiding a double (carotid-carotid-subclavian) transposition. At 3-year follow-up, neither endoleaks nor neurological events occurred. With our growing experience, in 3 patients (2 with acute type-B dissection and 1 with a penetrating ulcer of the arch), we decided to extend the proximal landing zone to the ascending aorta (zone 0).22 The brachiocephalic trunk and left common carotid artery were reimplanted to a Dacron tube, which was anastomosed to the proximal part of the ascending aorta with a mini-sternotomic approach. This minimally invasive surgical act, not charged with the same risks as the conventional surgical treatment of aortic disease, allowed for the lengthening of the proximal landing zone and a more stable fixation of the device. The proximal extension strategy determined a significantly longer mean stent-graft length in our patients (160 ± 82 mm) compared to a mean length ranging from 100–140 mm reported by other authors.23–36 In 35% of the patients, multiple overlapping stent-grafts were needed due to the emergency setting of the procedures and the lack of customized devices of proper length. Longer stent-grafts were used in acute type-B dissections, which in contrast to other experiences3,4 were treated by excluding not only the primary intimal tear, but also the multiple distal re-entries, in order to definitively obliterate the false lumen, preventing an aneurysmatic evolution at follow-up. Despite the risk of spinal cord ischemia due to the exclusion of multiple intercostal arteries,48 in our series paraplegia did not occur even in patients who underwent stenting of the distal aorta. A circulatory remuneration from the lumbar arteries, furnishing a suitable support of blood to the spinal cord, could justify the lack of morbidity. Nevertheless, whenever clinical signs of impaired perfusion occur, cerebrospinal fluid drainage has been reported to be an effective technique in decompressing the spinal cord from ischemia-related edema and in reversing paraplegia.49–51 In patients treated for complicated type-B dissection, neither aortic expansion nor endoleaks were detected at follow up.
Study limitations. There are some limitations inherent to our study that should be acknowledged. Our study involved a small cohort of patients, and our results should therefore be confirmed in larger, controlled studies. Other limitations are the retrospective nature of the study and the lack of a control group.
Conclusion
Our experience of ESG in patients with acute thoracic aorta syndromes showed an acceptably low mortality and morbidity. The proximal landing zone extension strategy resulted in a very low rate of endoleaks (only 1 small type-IB endoleak) at a long-term follow up (mean duration, 43 months; all patients longer than 12 months), confirming the initial expectation of an improved long-term procedural result. Debranching procedures of the brachiocephalic trunk and left common carotid artery can eventually be performed in selected patients; revascularization of the left subclavian artery is not necessary if there is good blood supply to the basilar circulation from the contralateral vertebral artery.
References
- Dake MD, Miller DC, Semba CP, et al. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med 1994;33:1729–1734.
- Dake MD, Miller DC, Mitchell RS, et al. The “first generation” of endovascular stent-grafts for patients with aneurysms of the descending thoracic aorta. J Thorac Cardiovasc Surg 1998;116:689–703.
- Dake MD, Kato N, Mitchell RS, et al. Endovascular stent-graft placement for the treatment of acute aortic dissections. N Engl J Med 1999;340:1546–1552.
- Nienhaber CA, Fattori R, Lund G, et al. Nonsurgical reconstruction of thoracic aortic dissection by stent-graft placement. N Engl J Med 1999;340:1539–1545.
- Czerny M, Cejna M, Hutschala D, et al. Stent-graft placement in atherosclerotic descending thoracic aorta aneurysms: Midterm results. J Endovasc Ther 2004;11:26–32.
- Jones LE. Endovascular stent grafting of thoracic aortic aneurysms: Technological advancements provide an alternative to traditional surgical repair. J Cardiovasc Nurs 2005;20:376–384.
- Baumgart D, Eggebrecht H, Herold U, et al. Underlying aortic pathology and clinical health status determine success of endovascular stent-grafting for descending thoracic aortic disease. Catheter Cardiovasc Interv 2006;67:527–534.
- Chaer RA, Makaroun MS, Chedrawy EG, et al. Endovascular treatment of aortic aneurysms: Techniques and clinical update. Cardiology 2007;109:145–153.
- Semba CP, Mitchell RS, Miller DC, et al. Thoracic aortic aneurysm repair with endovascular stent-grafts. Vasc Med 1997;2:98–103.
- Falk JL, Rackow EC, Blumenberg R, et al. Hemodynamic and metabolic effects of abdominal aortic crossclamping. Am J Surg 1981;142:174–177.
- Imagawa H, Takano H, Kato M, et al. Evaluation of left ventricular function utilizing transesophageal echocardiography during and after thoracic aortic aneurysm repair. Eur J Cardiothorac Surg 1993;7:371–375.
- Vilacosta I, Román JA. Acute aortic syndrome. Heart 2001;85:365–368.
- Macura KJ, Corl FM, Fishman EK, et al. Pathogenesis in acute aortic syndromes: Aortic dissection, intramural hematoma, and penetrating atherosclerotic aortic ulcer. AJR Am J Roentgenol 2003;181:309–316.
- Crawford ES, Hess KR, Cohen ES, et al. Ruptured aneurysm of the descending thoracic and thoracoabdominal aorta: Analysis according to size and treatment. Ann Surg 1991;213:417–425.
- Mastroroberto P, Chello M. Emergency thoracoabdominal aortic aneurysm repair: Clinical outcome. J Thorac Cardiovasc Surg 1999;118:477–482.
- Kouchoukos NT, Masetti P, Rokkas CK, et al. Hypothermic cardiopulmonary bypass and circulatory arrest for operations on the descending thoracic and thoraco abdominal aorta. Ann Thorac Surg 2002;74(Suppl):S1885–S1887.
- Huynh TTT, Miller CC, Estrera AL, et al. Thoracoabdominal and descending thoracic aortic aneurysm surgery in patients aged 79 years or older. J Vasc Surg 2002;36:469–475.
- Jamieson WR, Janusz MT, Gudas VM, et al. Traumatic rupture of the thoracic aorta: Third decade of experience. Am J Surg 2002;183:571–575.
- Gammie JS, Shah AS, Hattler BG, et al. Traumatic aortic rupture: Diagnosis and management. Ann Thorac Surg 1998;66:1295–1300.
- Cowley RA, Turney SZ, Hankins JR, et al. Rupture of thoracic aorta caused by blunt chest trauma: A fifteen year experience. J Thorac Cardiovasc Surg 1990;100:652–661.
- von Oppell UO, Dunne TT, De Groot MK, et al. Traumatic aortic rupture: Twenty-year meta analysis of mortality and risk of paraplegia. Ann Thorac Surg 1994;58:585–593.
- Mitchell RS, Ishimaru S, Ehrlich MP, et al. First international summit on thoracic aortic endografting: Roundtable on thoracic aortic dissection as an indication for endografting. J Endovasc Ther 2002;9(Suppl 2):98–105.
- Melnitchouk S, Pfammatter T, Kadner A, et al. Emergency stent-graft placement for hemorrhage control in acute thoracic aortic rupture. Eur J Cardiothorac Surg 2004;25:1032–1038.
- Grabenwoger M, Fleck T, Czerny M, et al. Endovascular stent graft placement in patients with acute thoracic aortic syndromes. Eur J Cardiothorac Surg 2003;23:788–793.
- Doss M, Balzer J, Martens S, et al. Surgical versus endovascular treatment of acute thoracic aortic rupture: A single-center experience. Ann Thorac Surg 2003;76:1465–1469.
- Shimono T, Kato N, Yasuda F, et al. Transluminal stent-graft placements for the treatment of acute onset and chronic aortic dissections. Circulation 2002;106(12 Suppl 1):I241–I247.
- Scheinert D, Krankenberg H, Schmidt A, et al. Endoluminal stent-graft placement for acute rupture of the descending thoracic aorta. Eur Heart J 2004;25:694–700.
- Czermak BV, Waldenberger P, Perkmann R, et al. Placement of endovascular stent-grafts for emergency treatment of acute disease of the descending thoracic aorta. AJR Am J Roentgenol 2002;179:337–345.
- Lachat M, Pfammatter T, Witzke H, et al. Acute traumatic aortic rupture: Early stent-graft repair. Eur J Cardiothorac Surg 2002;21:959–963.
- Demers P, Miller DC, Mitchell RS, et al. Stent-graft repair of penetrating atherosclerotic ulcers in the descending thoracic aorta: Mid-term results. Ann Thorac Surg 2004;77:81–86.
- Hutschala D, Fleck T, Czerny M, et al. Endoluminal stent-graft placement in patients with acute aortic dissection type B. Eur J Cardiothorac Surg 2002;21:964–969.
- Marty-Ane CH, Berthet JP, Branchereau P, et al. Endovascular repair for acute traumatic rupture of the thoracic aorta. Ann Thorac Surg 2003;75:1803–1807.
- Morishita K, Kurimoto Y, Kawaharada N, et al. Descending thoracic aortic rupture: Role of endovascular stent-grafting. Ann Thorac Surg 2004;78:1630–1634.
- Kaya A, Heijmen RH, Overtoom TT, et al. Thoracic stent grafting for acute aortic pathology. Ann Thoracic Surg 2006;82:560–565.
- Iyer VS, Mackenzie KS, Tse LW, et al. Early outcomes after elective and emergent endovascular repair of the thoracic aorta. J Vasc Surg 2006;43:677–683.
- Kaya A, Heijmen RH, Rousseau H, et al. Emergency treatment of the thoracic aorta: Results in 113 consecutive acute patients (The Talent Thoracic Retrospective Registry) Eur J Cardiothor Surg 2009;35:276–281.
- Leurs LJ, Bell R, Degrieck Y, et al. EUROSTAR: UK Thoracic Endograft Registry Collaborators. Endovascular treatment of thoracic aortic diseases: Combined experience from the EUROSTAR and United Kingdom Thoracic Endograft Registries. J Vasc Surg 2004;40:670–679.
- Weigang E, Luehr M, Harloff A, et al. Incidence of neurological complications following overstenting of the left subclavian artery. Eur J Cardiothorac Surg 2007;31:628–636.
- Riesenman PJ, Farber MA, Mendes RR, et al. Coverage of the left subclavian artery during thoracic endovascular aortic repair. J Vasc Surg 2007;45:90–94.
- Rehders TC, Petzsch M, Ince H, et al. Intentional occlusion of the left subclavian artery during stent-graft implantation in the thoracic aorta: Risk and relevance. J Endovasc Ther 2004;11:659–666.
- Gorich J, Asquan Y, Seifarth H, et al. Initial experience with intentional stent-graft coverage of the subclavian artery during endovascular thoracic aortic repairs. J Endovasc Ther 2002;9(Suppl II):II39–II43.
- Woo EY, Carpenter JP, Jackson BM, et al. Left subclavian artery coverage during thoracic endovascular aortic repair: A single center experience. J Vasc Surg 2008;48:555–560.
- Reece TB, Gazoni LM, Cherry KJ, et al. Reevaluating the need for left subclavian artery revascularization with thoracic endovascular aortic repair. Ann Thorac Surg 2007;84:1201–1205.
- Cooper DG, Walsh SR, Sadat U, et al. Neurological complications after left subclavian artery closure during thoracic endovascular aortic repair. A systematic review and meta-analysis. J Vasc Surg 2009;49:1594–1601.
- Tse LW, MacKenzie KS, Montreuil B, et al. The proximal landing zone in endovascular repair of the thoracic aorta. Ann Vasc Surg 2004;18:178–185.
- Burks JA Jr, Faries PL, Gravereaux EC, et al. Endovascular repair of thoracic aortic aneurysms: Stent-graft fixation across the aortic arch vessels. Ann Vasc Surg 2002;16:24–28.
- Coady MA, Rizzo JA, Hammond GL, et al. Penetrating ulcer of the thoracic aorta: What is it? How do we recognize it? How do we manage it? Vasc Surg 1998;27:1006–1015.
- Gravereaux EC, Faries PL, Burks JA, et al. Risk of spinal cord ischemia after endograft repair of thoracic aortic aneurysms. J Vasc Surg 2001;31:997–1003.
- Tiesenhausen K, Amann W, Koch G, et al. Cerebrospinal fluid drainage to reverse paraplegia after endovascular thoracic aortic aneurysm repair. J Endovasc Ther 2000;7:132–135.
- Greenberg R, Resch I, Nyman U, et al. Endovascular repair of descending thoracic aortic aneurysm: An early experience with intermediate-term follow-up. J Vasc Surg 2000;31:147–156.
- Chiesa R, Melissano G, Marrocco-Trischitta MM, et al. Spinal cord ischemia after elective stent-graft repair of the thoracic aorta. J Vasc Surg 2005;42:11–17.
_____________________________
From the Departments of *Cardiology, §Cardiac Surgery and †Imaging Diagnos- tic, Pasquinucci Heart Hospital, Toscana Gabriele Monasterio Foundation, Massa, Italy; and the £Department of Vascular Surgery, Toscana, Carrara, Italy.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 24, 2010, provisional acceptance given Decem- ber 14, 2010, final version accepted February 1, 2011.
Address for correspondence: Marco Vaghetti, MD, Department of Cardiology, Pasquinucci Heart Hospital, Gabriele Monasterio Foundation, Via Aurelia Sud 54100 Massa Italy. E-mail: vaghetti@ifc.cnr.it










