

Entrapment of a Looped/Kinked Catheter in the Brachial Artery and its Successful Retrieval During Transradial Coronary Catheterization
Abstract: Transradial access for cardiac catheterization is widely accepted as a safe and viable approach with markedly decreased incidence of major access-related complications compared to the transfemoral approach. Minor catheter looping or kinking during catheter manipulation is common and can be managed with gentle rotation, and thus goes unnoticed without complications. Rarely, this looped/kinked catheter can get entrapped and require an invasive approach for retrieval. To our knowledge, there is only one such case described for the transradial approach, where the authors had to use a 6 Fr Amplatz gooseneck snare kit via right femoral approach to remove the entrapped catheter. We present a case of entrapped looped/kinked 5 Fr catheter during transradial catheterization in the brachial artery and describe a novel approach of removing this entrapped catheter through the same radial access without any complications.
J INVASIVE CARDIOL 2012;24(9):471-472
Key words: transradial catheterization, complications, kinked catheter, looped catheter
_______________________________________________
Transradial access is rapidly becoming the most popular vascular access for cardiac catheterization. It is widely accepted to be a very safe and viable approach, with significantly less incidence of major access-related complications compared to the transfemoral approach.1,2
In some cases, catheters can become entrapped looped/kinked during transradial catheterization in the brachial artery. Regular maneuvers and manipulations in an attempt to disengage the catheter are often successful. We describe a novel approach of removing this entrapped catheter through the same radial access without any complications.
Case Report
 A 58-year-old male with past medical history of paroxysmal atrial fibrillation was scheduled for an elective left heart catheterization. The wrist was prepared in the usual manner with local anesthesia using lidocaine in addition to adjunctive use of intravenous fentanyl and midazolam. A cocktail made of verapamil, heparin, and nitroglycerin was also injected into the sheath. After engaging and imaging the right coronary artery (RCA) and performing a left ventriculogram using a 5 Fr JR4 catheter, a long exchange J-tipped wire was used to place a 5
A 58-year-old male with past medical history of paroxysmal atrial fibrillation was scheduled for an elective left heart catheterization. The wrist was prepared in the usual manner with local anesthesia using lidocaine in addition to adjunctive use of intravenous fentanyl and midazolam. A cocktail made of verapamil, heparin, and nitroglycerin was also injected into the sheath. After engaging and imaging the right coronary artery (RCA) and performing a left ventriculogram using a 5 Fr JR4 catheter, a long exchange J-tipped wire was used to place a 5 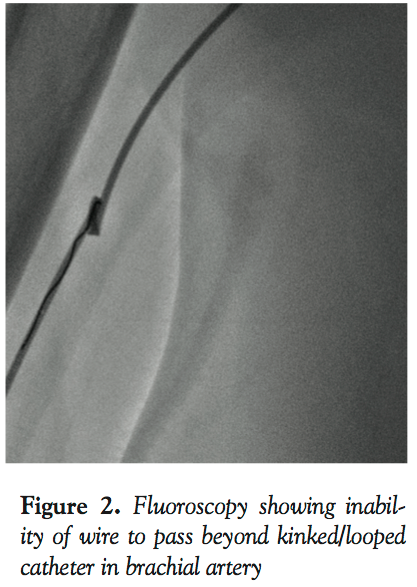 Fr JL4 catheter. Some spasm was encountered going up with the JL4. While clocking and advancing the catheter, we noticed damping of the arterial wave paralleled with inability to further manipulate the catheter. On fluoroscopy, the JL was found looped and kinked on itself in the brachial segment (Figure 1). Different maneuvers to de-loop it failed, including external fixation of the distal part of the catheter at the arm level both by putting circumferential pressure on the arm with our hands as well as by inflating the blood pressure cuff to a different level at the arm so it forms an anchor for us to untwist the loop. We could not even advance a coronary wire into that loop (Figure 2). Another cocktail was used in vain. To resolve our problem, we used the scalpel to cut the proximal part of the JL catheter. Next, we exchanged the 6 Fr 12 cm sheath with a 5 Fr long sheath while the severed and trapped JL4 catheter served as a guidewire. We advanced the sheath up to the anticubital fossa (Figure 3). Under fluoroscopy, we gently pulled the trapped catheter. It smoothly unfolded its loop while slipping into the long sheath, hence freeing the catheter. It is important to mention here that complete inability of the catheter to move due to kink/loop can be a limitation of this technique. Dye was then injected in the catheterless sheath to confirm patency of the brachial artery. We had contemplated using a larger French sheath in lieu of the 5 Fr one based on the fact that the loop has a better chance of slipping into the wider lumen of the larger sheath. The problem was that the introducer of the 6, 7, or 8 Fr sheaths would not go over the 5 Fr catheter, which was thicker than the wire. Also, it would have been incautious to push any of these sheaths without their respective introducer directly over the trapped catheter, which would, at the least, risk stripping the arterial intima. Because of the resulting spasm in the radial artery, the procedure was switched to femoral. Three months later, the patient still has his radial and ulnar pulses in his right hand and no long-term complications were noted. To our knowledge, this is the first description of this method in removing the looped cardiac catheter from the radial access.
Fr JL4 catheter. Some spasm was encountered going up with the JL4. While clocking and advancing the catheter, we noticed damping of the arterial wave paralleled with inability to further manipulate the catheter. On fluoroscopy, the JL was found looped and kinked on itself in the brachial segment (Figure 1). Different maneuvers to de-loop it failed, including external fixation of the distal part of the catheter at the arm level both by putting circumferential pressure on the arm with our hands as well as by inflating the blood pressure cuff to a different level at the arm so it forms an anchor for us to untwist the loop. We could not even advance a coronary wire into that loop (Figure 2). Another cocktail was used in vain. To resolve our problem, we used the scalpel to cut the proximal part of the JL catheter. Next, we exchanged the 6 Fr 12 cm sheath with a 5 Fr long sheath while the severed and trapped JL4 catheter served as a guidewire. We advanced the sheath up to the anticubital fossa (Figure 3). Under fluoroscopy, we gently pulled the trapped catheter. It smoothly unfolded its loop while slipping into the long sheath, hence freeing the catheter. It is important to mention here that complete inability of the catheter to move due to kink/loop can be a limitation of this technique. Dye was then injected in the catheterless sheath to confirm patency of the brachial artery. We had contemplated using a larger French sheath in lieu of the 5 Fr one based on the fact that the loop has a better chance of slipping into the wider lumen of the larger sheath. The problem was that the introducer of the 6, 7, or 8 Fr sheaths would not go over the 5 Fr catheter, which was thicker than the wire. Also, it would have been incautious to push any of these sheaths without their respective introducer directly over the trapped catheter, which would, at the least, risk stripping the arterial intima. Because of the resulting spasm in the radial artery, the procedure was switched to femoral. Three months later, the patient still has his radial and ulnar pulses in his right hand and no long-term complications were noted. To our knowledge, this is the first description of this method in removing the looped cardiac catheter from the radial access.
Discussion
 Transradial access is presently the most popular vascular access for cardiac catheterization. It is widely accepted to be a very safe and viable approach, with significantly less incidence of major access-related complications compared to the transfemoral approach.1,2 The majority of interventional cardiologists prefer right radial access, since it is easy to manipulate catheters and devices through this approach. As per survey data, 90% of interventional cardiologists chose the right radial artery as the first access route during transradial procedures.3 Minor catheter looping or kinking during catheter manipulation is common; it usually can be managed with gentle rotation in the opposite direction, and thus goes unnoticed without complications. Rarely, this looped/kinked catheter can get entrapped4 and can require an invasive approach for retrieval. To our knowledge, there is only one such case described via transradial approach, where the authors used a 6 Fr Amplatz gooseneck snare kit via right femoral approach to remove the entrapped catheter.4 Rarely, a looped catheter may actually represent an underlying anatomic variation like a brachial loop,5 which can be confirmed with a pre- or postprocedure angiogram. In our patient, postprocedure angiogram did not reveal any anomalous loop in the brachial artery.
Transradial access is presently the most popular vascular access for cardiac catheterization. It is widely accepted to be a very safe and viable approach, with significantly less incidence of major access-related complications compared to the transfemoral approach.1,2 The majority of interventional cardiologists prefer right radial access, since it is easy to manipulate catheters and devices through this approach. As per survey data, 90% of interventional cardiologists chose the right radial artery as the first access route during transradial procedures.3 Minor catheter looping or kinking during catheter manipulation is common; it usually can be managed with gentle rotation in the opposite direction, and thus goes unnoticed without complications. Rarely, this looped/kinked catheter can get entrapped4 and can require an invasive approach for retrieval. To our knowledge, there is only one such case described via transradial approach, where the authors used a 6 Fr Amplatz gooseneck snare kit via right femoral approach to remove the entrapped catheter.4 Rarely, a looped catheter may actually represent an underlying anatomic variation like a brachial loop,5 which can be confirmed with a pre- or postprocedure angiogram. In our patient, postprocedure angiogram did not reveal any anomalous loop in the brachial artery.
 We describe the case of an entrapped looped/kinked 5 Fr catheter during transradial catheterization in the brachial artery. Regular maneuvers and manipulations could not un-loop or disengage the catheter and we could not even advance a coronary wire into that loop. We describe a novel approach of removing this entrapped catheter through the same radial access without any complications.
We describe the case of an entrapped looped/kinked 5 Fr catheter during transradial catheterization in the brachial artery. Regular maneuvers and manipulations could not un-loop or disengage the catheter and we could not even advance a coronary wire into that loop. We describe a novel approach of removing this entrapped catheter through the same radial access without any complications.
Acknowledgment. We personally acknowledge Dr Rubin Kandov and Dr Fouad Ghavami for their help in the management of this patient and Dr Sumaya Teli for her help in preparing this manuscript.
References
- Brueck M, Bandorski D, Kramer W, et al. A randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty. JACC Cardiovasc Interv. 2009;2(11):1047-1054.
- Jolly SS, Amlani S, Hamon M, et al. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J. 2009;157(1):132-140.
- Bertrand OF, Rao SV, Pancholy S, et al. Transradial approach for coronary angiography and interventions: results of the first international transradial practice survey. JACC Cardiovasc Interv. 2010;3(10):1022-1031.
- Kim JY, Moon KW, Yoo KD. Entrapment of a kinked catheter in the radial artery during transradial coronary angiography. J Invasive Cardiol. 2012;24(1):E3-E4.
- Wang HJ, Lee KW, Hsieh DJ. Brachial loop: transradial technique to overcome this rare anatomic variation. Catheter Cardiovasc Interv. 2006;68(2):260-262.
_______________________________________________
From the 1Division of Cardiology and 2Department of Internal Medicine, Staten Island University Hospital, Staten Island, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 8, 2012, provisional acceptance given April 23, 2012, final version accepted April 30, 2012.
Address for correspondence: Tariq Bhat, MD, 475 Seaview Ave, Staten Island NY 10305. Email: mohiuddin_bhat@yahoo.com










