

Entrapment of Rotational Atherectomy Burrs in Freshly Implanted Stents: First Illustration of the Rolled-Up Phenomenon
Abstract: Objectives. We aimed to illustrate one of the mechanisms of rotational atherectomy burr entrapment in a coronary stent where the burr was rolled up in the stent’s struts. Methods. We report a case where the treatment of a mid right coronary artery (RCA) lesion using a rotational atherectomy device was attempted. During the procedure, the burr suddenly got stuck in a freshly implanted stent in the distal RCA. Despite several attempts and maneuvers, we were unable to pull back the burr. Results. The patient was transferred for emergency surgery. The length of the RCA from its proximal third to the crux, including the stuck burr and the freshly implanted stent, had to be extracted. Conclusions. Physicians performing rotational atherectomy should be aware of this complication and know the principal endovascular maneuvers to extract the stuck burr. Operators should also be aware of roll-up burr entrapment, like this case, where most maneuvers to retrieve the burr will fail and should be managed, to our point of view, with surgery.
J INVASIVE CARDIOL 2016;28(11):E132-E133
Key words: complications, rotational atherectomy
Case Presentation
Despite the continual development of more supportive materials, such as guiding catheters and balloons with higher inflation pressures, debulking a heavily calcified lesion may still require rotational atherectomy in certain situations. We present the case of a 75-year-old patient with past medical history of three coronary artery bypass grafts (CABGs) and bare-metal stent implantation in the proximal right coronary artery (RCA) who was admitted to our institution with an acute non-ST segment myocardial infarction.
At coronary angiogram, the culprit lesions were found to be the mid and distal segments of the RCA (Figure 1A). The mid segment lesion was highly calcified and attempts at predilation using scoring balloons, cutting balloons, and high-pressure non-compliant balloons all failed. Therefore, no stenting was performed and only the distal segment lesion was treated using a 3.0 x 28 mm everolimus-eluting stent after predilation (Figure 1B). The next day, the patient presented with recurrent chest pain, and treatment of the mid RCA lesion using a rotational atherectomy device was attempted. A 1.25 mm burr crossed the lesion with some difficulty, and suddenly got stuck in the freshly implanted stent in the distal RCA (Figure 1C). Despite several removal attempts using force, we were unable to pull back the burr. In order to disengage it, a second guiding catheter was placed through a separate femoral sheath. A wire-twisting technique using three guides was attempted, followed by dilation using non-compliant balloons (1.25 x 15 mm, 1.50 x 15 mm, and 2.0 x 15 mm) by the burr, but was unsuccessful. Finally, a deep intubation of the guiding catheter was performed, but the burr remained stuck.
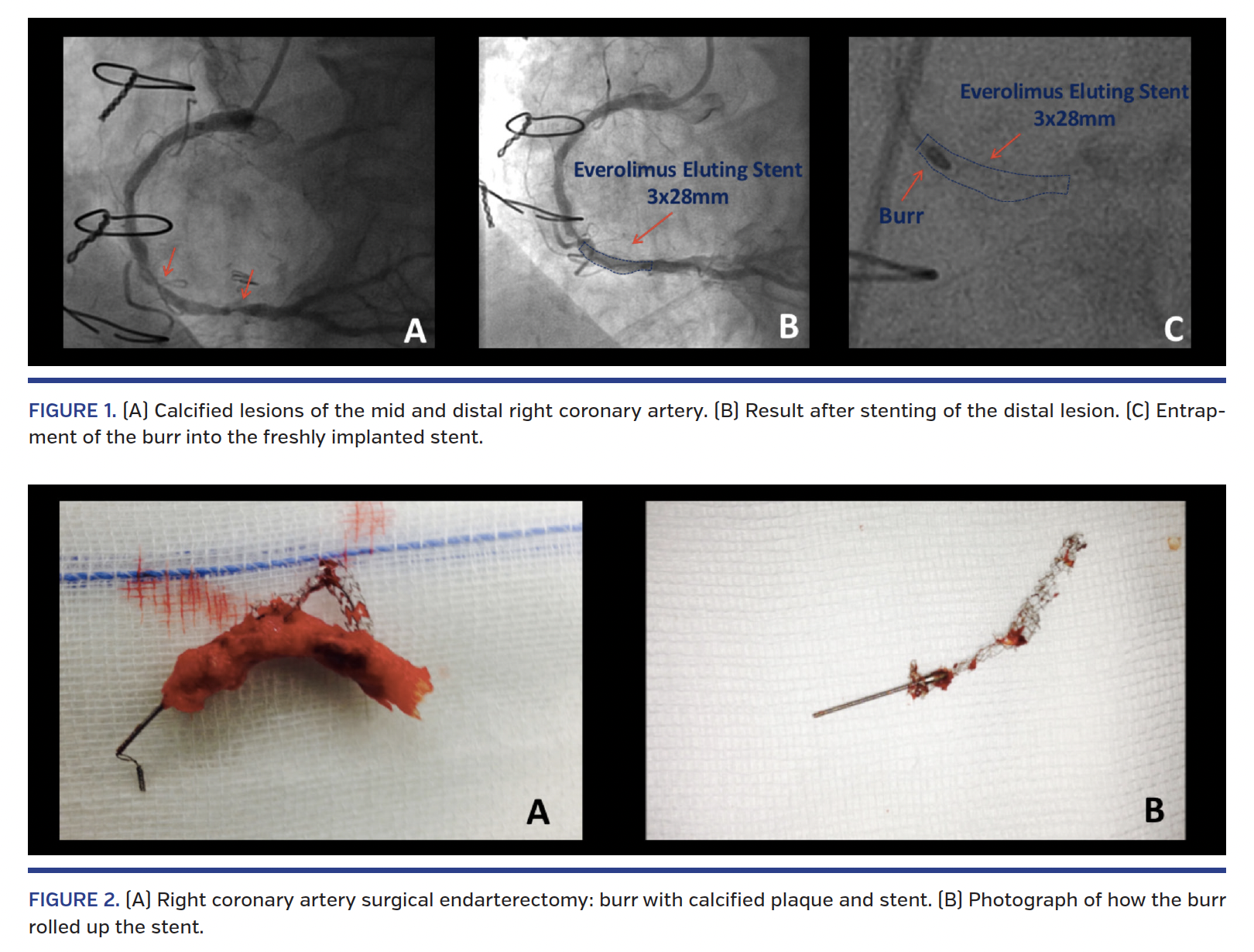
The patient then became unstable, with decreased flow in the distal RCA. Accordingly, the patient was transferred for emergency surgery. The length of the RCA from its proximal third to the crux, including the stuck rotablator and the freshly implanted stent, had to be extracted (Figure 2A). A new CABG was then performed using the right internal mammary artery. After careful dissection of the extracted length of RCA (Figure 2B), we observed that the burr was tightly rolled up in the freshly implanted stent.
Rotational atherectomy burr entrapment is a rare but dramatic complication. In contrast to rotational atherectomy for in-stent restenosis, a freshly implanted underexpanded stent is a known risk factor for stent entrapment, eg, rota- wire placed under the stent’s struts. Here we illustrated one of the mechanisms of rotational atherectomy burr entrapment in a coronary stent where the burr is rolled up in the stent’s struts. Physicians performing rotational atherectomy should be aware of this complication and know the principal endovascular maneuvers to extract the stuck burr.1 Operators should also be aware of roll-up burr entrapment, as in this case, where most maneuvers to retrieve the burr will fail and should be managed, to our point of view, with surgery.
References
1. Sulimov DS, Abdel-Wahab M, Toelg R, Kassner G, Geist V, Richardt G. Stuck rotablator: the nightmare of rotational atherectomy. EuroIntervention. 2013;9:251-258.
From the 1University Hospital Center Vaudois (CHUV), Department of Cardiology, Lausanne, Switzerland; and 2University Hospital Centre Vaudois (CHUV), Department of Cardiovascular Surgery, Lausanne, Switzerland.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted May 17, 2016, and accepted June 1, 2016.
Address for correspondence: Olivier Muller, MD/PhD, Department of Cardiology, Rue du Bugnon 46, CH-1011 Lausanne, Switzerland. Email: Olivier.Muller@chuv.ch










