

Flexions of the Popliteal Artery: Technical Considerations of Femoropopliteal Stenting
Abstract: Popliteal artery morphology changes while undergoing knee motion. A main flexion (i.e., the ‘hinge point’) and other flexions (termed ‘accessory flexions’) were described as a result of popliteal artery adaptation to knee flexion. Knee dynamics challenge the outcome of popliteal artery endovascular procedures. Complications such us stent fractures were reported despite rapidly improving technology. Understanding popliteal artery dynamics allows us to develop an endovascular technique that facilitates the avoidance of the difficulties of one of the most mobile arteries in the body. Here we report two cases with a novel stent implantation technique in the popliteal artery. The method includes diagnostic angiography, lesion angioplasty, and stenting using both extended and flexed knee in lateral view. The pressure gradients were measured with knee in extension and flexion before and after each step. A successful outcome was achieved in both cases. This method allows us: 1) to identify the flexions of the popliteal artery and its relationship with the lesions; 2) to detect those obstructions not visible with an extended knee; 3) to understand that the hinge point and accessory flexions can develop undesired and unexpected artery obstruction after a stent implantation only observed in knee flexion; and 4) to identify the morphological changes caused in the popliteal artery and its subsequent solution.
J INVASIVE CARDIOL 2011;23(10):431–433
Key words: popliteal artery, stent, femoropopliteal, stent fracture
______________________________________
Stent stress and stent fractures due to the effects of the mechanical environment in peripheral arteries, particularly in the femoropopliteal territory, have been reported.1 We, and others, have described the changes that occur in the popliteal artery during knee flexion.2,3 Briefly, the popliteal artery adapts to the knee flexion developing a main flexion, known as the hinge point.2 Using dynamic angiography, we observed the hinge point moving toward the medial supracondylar tubercle in a lateral view.2 In knee extension, the medial supracondylar tubercle lies at the same level as the upper border of the patella.2 We concluded that the hinge point flexion of the popliteal artery could be predicted using the anteroposterior angiogram view during knee extension. The hinge point flexion is occasionally accompanied by accessory flexions, which can occur above or below this point.2 The accessory flexions were only observed in a lateral view angiogram in knee flexion.2,4 The number, location, and degree of the flexion angle of accessory flexions cannot be predicted with conventional angiograms performed in knee extension. In addition, the morphology of the popliteal artery may be altered due to the presence of a stent and, importantly, the stent structure and patency can be altered by flexions of the popliteal artery.1,5 Based on these findings, implanting stents in the popliteal artery with knee extension view control may help identify the appropriate area to release the stent. Here, we report two cases using a new protocol for stent implantation in the popliteal artery.
Patients and Methods
Diagnostic and therapeutic procedure. A 6 Fr sheath was introduced through femoral arterial access in antegrade fashion. Then, a 0.014˝ soft exchange guidewire was inserted through a hydrophilic 4 Fr coated catheter with a 0.038˝ lumen diameter attached to a Tuohy Borst hemostasis valve. Pressure gradients were measured and recorded with two channels in order to obtain two simultaneous pressure recordings, proximal and distal to the obstruction. The pressure proximal to the obstruction was obtained through the side arm of the introducer sheath, while the distal pressure was measured through the side arm of the Tuohy Borst hemostasis valve connected to the angiographic catheter. Pressures were measured and recorded without withdrawing the 0.014˝ guidewire. Angioplasty of the lesion was performed with adequate balloon size when necessary. Angiography and pressure gradient controls were obtained initially and in each post stent implantation; with extended and then with flexed knee in the lateral and/or anteroposterior views. Angiograms were performed using low osmolarity contrast material. Stent implantation was performed under angiographic control with the knee flexed, in a lateral position. The stents selected were either balloon-expandable or self-expandable. Institutional Ethics Committee Informed Consent form was signed in both cases.
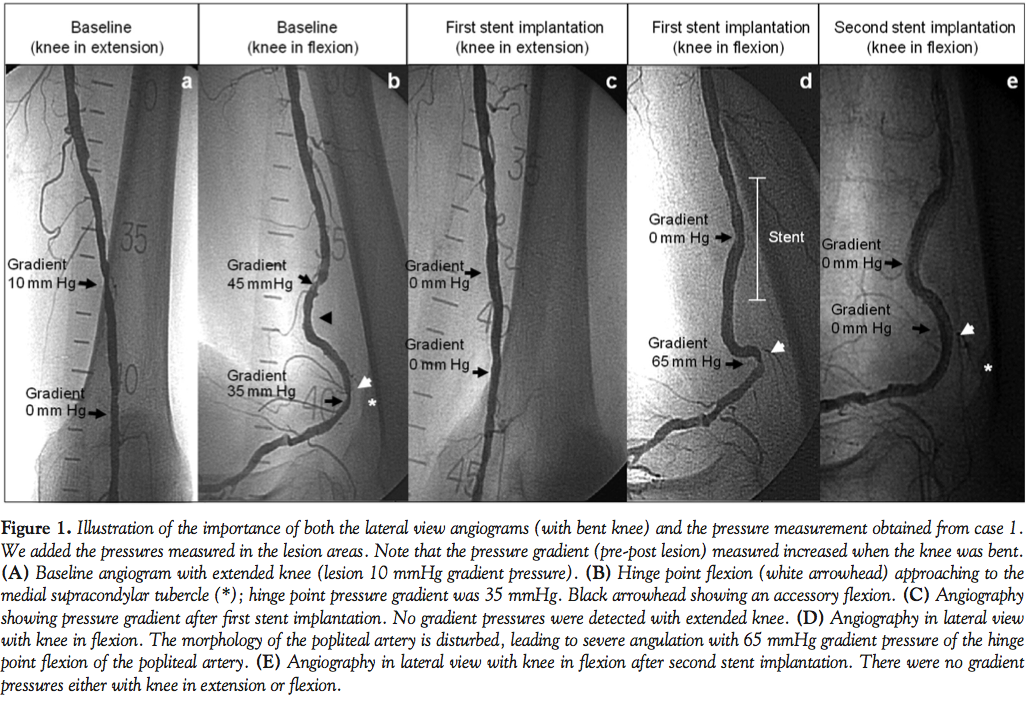 Case 1. A 78-year-old Caucasian male patient with history of ischemic heart disease, hypertension, and smoking was diagnosed with severe ischemia of the left lower limb with dry ulcerative lesions (Rutherford category 5, Fontaine 4). A conventional left leg angiogram revealed a severe lesion in the popliteal artery at the level of the abductor canal; posterior tibial and peroneal arteries were occluded; anterior tibial artery was seen through collateral circulations. Popliteal artery initial pressure gradient was 10 mmHg (Figure 1A). In knee flexion, the pressure gradient increased to 45 mmHg (Figure 1B); a lesion was also visible at the hinge point in flexion with a 35 mmHg pressure gradient, but not visible with an extended leg. An upper accessory flexion was also noticeable (Figure 1B). Balloon angioplasty was performed in the upper popliteal artery lesion and then a 7.0 x 78 mm self-expandable Sentinol nitinol vascular stent was implanted (Boston Scientific, Inc.). The control angiogram with an extended knee revealed neither obstructions nor pressure gradients (Figure 1C). However, angiography with flexed knee in lateral view showed a severe 65 mmHg gradient due to the popliteal artery anatomy modified by the stent (Figure 1D). A 6.0 x 30 mm self-expandable Protegé nitinol stent (ev3, Inc.) was successfully implanted at the hinge point flexion and no pressure gradient was detected in knee flexion (Figure 1E). The patient was discharged home on clopidogrel 75 mg, aspirin 100 mg/day and cilostazol 100 mg/day. Forty-five days after the procedure, the patient was readmitted to the hospital with a subendocardial infarction, requiring a coronary angiography. Left leg angiogram in knee flexion and extension showed a patent popliteal artery. The patient died during the hospital admission.
Case 1. A 78-year-old Caucasian male patient with history of ischemic heart disease, hypertension, and smoking was diagnosed with severe ischemia of the left lower limb with dry ulcerative lesions (Rutherford category 5, Fontaine 4). A conventional left leg angiogram revealed a severe lesion in the popliteal artery at the level of the abductor canal; posterior tibial and peroneal arteries were occluded; anterior tibial artery was seen through collateral circulations. Popliteal artery initial pressure gradient was 10 mmHg (Figure 1A). In knee flexion, the pressure gradient increased to 45 mmHg (Figure 1B); a lesion was also visible at the hinge point in flexion with a 35 mmHg pressure gradient, but not visible with an extended leg. An upper accessory flexion was also noticeable (Figure 1B). Balloon angioplasty was performed in the upper popliteal artery lesion and then a 7.0 x 78 mm self-expandable Sentinol nitinol vascular stent was implanted (Boston Scientific, Inc.). The control angiogram with an extended knee revealed neither obstructions nor pressure gradients (Figure 1C). However, angiography with flexed knee in lateral view showed a severe 65 mmHg gradient due to the popliteal artery anatomy modified by the stent (Figure 1D). A 6.0 x 30 mm self-expandable Protegé nitinol stent (ev3, Inc.) was successfully implanted at the hinge point flexion and no pressure gradient was detected in knee flexion (Figure 1E). The patient was discharged home on clopidogrel 75 mg, aspirin 100 mg/day and cilostazol 100 mg/day. Forty-five days after the procedure, the patient was readmitted to the hospital with a subendocardial infarction, requiring a coronary angiography. Left leg angiogram in knee flexion and extension showed a patent popliteal artery. The patient died during the hospital admission.
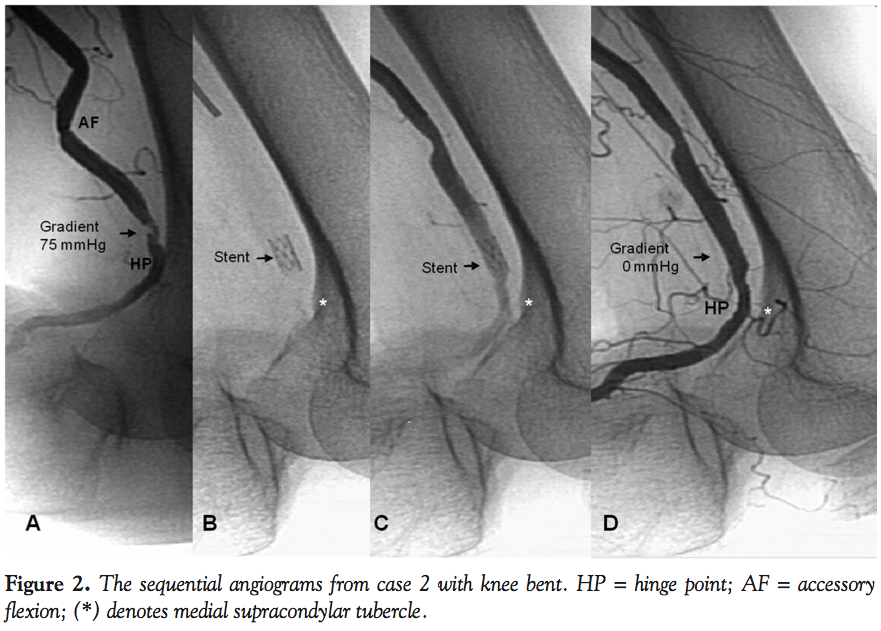 Case 2. An 88-year-old Caucasian female with a history of hypertension, breast cancer, and right mastectomy 11 years before was admitted for severe chronic left lower limb ischemia (Rutherford category 5, Fontaine 4). Angiogram showed a short and severe lesion in the straight segment above the hinge point flexion (Figure 2A), anterior tibial artery occluded in the distal segment, ostial occlusion of the posterior tibial artery, and proximal occlusion of the peroneal artery. Popliteal artery angioplasty was decided. The baseline pressure gradient measured across the popliteal artery lesion was 75 mmHg. A 5.0 x 13 mm balloon-expandable stent (Lacteba SA) (Figure 2B) was successfully implanted in knee flexion, avoiding the hinge point flexion (Figures 2C and 2D). There was no gradient pressure after the procedure. The patient was discharged on clopidogrel 75 mg/day and aspirin 100 mg/day. Fifteen days later, the patient was readmitted because of ischemia of the left limb. Angiography confirmed patency of the implanted stent.
Case 2. An 88-year-old Caucasian female with a history of hypertension, breast cancer, and right mastectomy 11 years before was admitted for severe chronic left lower limb ischemia (Rutherford category 5, Fontaine 4). Angiogram showed a short and severe lesion in the straight segment above the hinge point flexion (Figure 2A), anterior tibial artery occluded in the distal segment, ostial occlusion of the posterior tibial artery, and proximal occlusion of the peroneal artery. Popliteal artery angioplasty was decided. The baseline pressure gradient measured across the popliteal artery lesion was 75 mmHg. A 5.0 x 13 mm balloon-expandable stent (Lacteba SA) (Figure 2B) was successfully implanted in knee flexion, avoiding the hinge point flexion (Figures 2C and 2D). There was no gradient pressure after the procedure. The patient was discharged on clopidogrel 75 mg/day and aspirin 100 mg/day. Fifteen days later, the patient was readmitted because of ischemia of the left limb. Angiography confirmed patency of the implanted stent.
Discussion
Stent fractures have been described in the popliteal artery.1,6 It is due to material fatigue in flexion zones. We have previously described a main flexion in the popliteal artery, termed the ‘hinge point,’ and other flexions, termed the ‘accessory flexions,’ as a result of popliteal artery adaptation to knee flexion.2 Flexions of the popliteal artery have been involved in stent material fatigue.1 The occurrence of flexions in the popliteal artery is due to multiple factors. The popliteal artery has two fixed points, one proximal to the adductor canal and the other distal to the origin of the anterior tibial artery.7 The popliteal artery elongates and increases its rigidity due to aging;8 stent implantation also increases the rigidity of the artery.9 Arterial flexions, vessel elongation, and increased rigidity ultimately contribute to undesired and unexpected artery obstruction during knee flexion.7 Hence, information on individual flexion points for each patient is fundamental to improve success rates of popliteal artery stenting.2,10
The lateral angiogram view with popliteal artery in flexion position and the measurement of pressure gradients, which provide accurate information regarding the lesion, were essential to decide the treatment strategy and assess the results in the cases presented here. In case 1 (Figure 1), the type of stent used modified the angle degree of the accessory flexion, making the hinge point angle more acute and increasing the pressure gradient. Lateral angiography with the knee in flexion was useful to identify the changes caused by the stent and their subsequent solution.
In case 2 (Figure 2), with the knee in a flexed position, a straight landing zone was identified to implant a balloon-expandable stent, avoiding the area of flexion. Studies with balloon-expandable stents have shown unfavorable outcomes.11 Implanting stents in the popliteal artery in knee flexion may help to identify a safe area to deploy a stent and then prevent stent exposure to flexions unnecessarily. Endovascular treatment offers a low complication rate, high success rates, and excellent short-term results, but long-term results may be affected by fractures and restenosis.12 Self-expandable stents adapt to the dynamics of the femoropopliteal territory, but they may undergo stress and fracture when subjected to axial compression and flexion movements.1 This has been confirmed by in vitro studies1,13 and clinical trials, with an incidence of fractures that may vary between 2% and 37.2%, depending on the stent used.5,14 The number of flexions while waking and certain cultural habits such as kneeling down most of the day15 may cause structural damage to the stent, leading to fractures and restenosis.12,13 To understand the “dynamic anatomy” during knee flexion of the popliteal artery is the key to determine a correct strategy for an endovascular procedure.
The use of self-expandable, drug-eluting stents appears to be promising in an unprotected environment at the popliteal fossa. However, further investigation is still needed.16,17 The technique proposed in this manuscript may be used to overcome the mechanical forces affecting the popliteal artery during knee movements.1,2,15 In addition, our technique may be a viable option when considering research and development efforts surrounding stent technology for treatment of infrainguinal disease.
Conclusions
We present our technical considerations in spite of the short-term follow-up, which is a main limitation of this work. We believe that this technique has allowed us:
- To observe the dynamic variation in the flexion of the popliteal artery with pressure measurement in order to assess the severity of the obstructions pre- and post-stent implantation.
- To detect those obstructions not visible with an extended knee.
- To visualize severe obstructions caused by stents due to the changes in the architecture of the basal artery that occurs with a flexed knee.
- To use balloon-expandable stents in the femoropopliteal territory, identifying an appropriate landing zone and avoiding flexion areas.
Acknowledgments. The authors would like to thank the nursing, secretarial, and technical staff of the catheterization laboratory of Hospital Nacional Alejandro Posadas for their enthusiasm and their belief that our efforts were worthwhile and useful.
References
- Early M, Lally C, Prendergast PJ, Kelly DJ. Stresses in peripheral arteries following stent placement: a finite element analysis. Comput Methods Biomech Biomed Engin. [Research Support, Non-U.S. Gov’t]. 2009;12(1):25-33.
- Diaz JA, Villegas M, Tamashiro G, et al. Flexions of the popliteal artery: dynamic angiography. J Invasive Cardiol. 2004;16(12):712-715.
- Klein AJ, Chen SJ, Messenger JC, et al. Quantitative assessment of the conformational change in the femoropopliteal artery with leg movement. Catheter Cardiovasc Interv. 2009;74(5):787-798.
- Arena FJ. Arterial kink and damage in normal segments of the superficial femoral and popliteal arteries abutting nitinol stents — a common cause of late occlusion and restenosis? A single-center experience. J Invasive Cardiol. 2005;17(9):482-486.
- Scheinert D, Scheinert S, Sax J, et al. Prevalence and clinical impact of stent fractures after femoropopliteal stenting. J Am Coll Cardiol. 2005;45(2):312-315.
- Lewitton S, Babaev A. Superficial femoral artery stent fracture that led to perforation, hematoma, and deep venous thrombosis. J Invasive Cardiol. 2008;20(9):479-481.
- Avisse C, Marcus C, Ouedraogo T, Delattre JF, Menanteau B, Flament JB. Anatomo-radiological study of the popliteal artery during knee flexion. Surg Radiol Anat. 1995;17(3):255-262.
- Mozersky DJ, Sumner DS, Hokanson DE, Strandness DE Jr. Transcutaneous measurement of the elastic properties of the human femoral artery. Circulation. 1972;46(5):948-955.
- Zocholl G, Zapf S, Schild H, Thelen M. [Functional angiography of the arteries near the knee joint: consequences for stent implantation?]. Rofo. 1990;153(6):658-662.
- Kroger K, Santosa F, Goyen M. Biomechanical incompatibility of popliteal stent placement. J Endovasc Ther. 2004;11(6):686-694.
- Grimm J, Muller-Hulsbeck S, Jahnke T, Hilbert C, Brossmann J, Heller M. Randomized study to compare PTA alone versus PTA with Palmaz stent placement for femoropopliteal lesions. J Vasc Interv Radiol. 2001;12(8):935-942.
- Schillinger M, Minar E. Past, present, and future of femoropopliteal stenting. J Endovasc Ther. 2009;16(Suppl 1):I147-I152.
- Nikanorov A, Smouse HB, Osman K, Bialas M, Shrivastava S, Schwartz LB. Fracture of self-expanding nitinol stents stressed in vitro under simulated intravascular conditions. J Vasc Surg. 2008;48(2):435-440.
- Schlager O, Dick P, Sabeti S, et al. Long-segment SFA stenting — the dark sides: in-stent restenosis, clinical deterioration, and stent fractures. J Endovasc Ther. 2005;12(6):676-684.
- Diaz JA, Miceli MH, Tamashiro A. Dynamic anatomy of the popliteal artery: might culture affect the outcome of endovascular therapy? J Endovasc Ther. 2005;12(5):623-625.
- Minar E. Drug-eluting stents above the knee. J Cardiovasc Surg (Torino). 2011;52(2):225-229.
- Bosiers M, Deloose K, Callaert J, Keirse K, Verbist J, Peeters P. Drug-eluting stents below the knee. J Cardiovasc Surg (Torino). 2011;52(2):231-234.
______________________________________
From the Department of Cardiology, Section of Hemodinamia, Hospital Nacional Alejandro Posadas, Buenos Aires, Argentina.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 6, 2011, provisional acceptance given July 15, 2011, final version accepted August 15, 2011.
Address for correspondence: Jose Antonio Diaz, MD, Pte. Illia s/n y Marconi - El Palomar (1684), Buenos Aires, Argentina. Email: jadhemosurg@hotmail.com









