

Good Efficacy of Drug-Eluting Balloons in a Mixed Population of Patients with Coronary Artery Disease
Abstract: Introduction. Drug-coated balloons (DCB) are being increasingly used in interventional cardiology and are established for the treatment of in-stent restenosis (ISR). It is unclear how effective they are in patients with de novo lesions. Methods. A prospective registry of patients treated with the In.Pact DCB at our institution was conducted. Patients with ISR and those with planned surgery or contraindication to long-term use of double-antiplatelet therapy were included. Outcome measures: 12-month rates of clinically driven target-lesion revascularization (TLR). The efficacy of DCB was compared between patients with ISR and de novo lesions and in those with reference vessel diameter (RVD) < and > 2.75 mm. Results. A total of 139 patients (222 lesions) were followed up for 12 months. The mean age was 69 ± 10 years. Ninety-five patients (68%) had stable angina and 44 patients (32%) had acute coronary syndrome. Clinically driven TLR was performed in 6/126 lesions (4.8%) in the de novo group and in 5/92 lesions (5.4 %) in the ISR group (P=1.0). In the de novo group, TLR rate was 1/45 (2.2%) in patients with vessel diameter >2.75 mm and 5/81 (6.2%) in those with diameter <2.75 (P=.42). In the ISR group, TLR was 3/71 (4.2%) in patients with vessel diameter >2.75 mm and 2/21 (9.5%) in those with diameter <2.75 mm (P=.32). Conclusions. DCB are a valuable treatment option for patients with ISR offering good rates of TLR. Additionally, DCB can be an alternative to drug-eluting stents, if the use of long-term double-antiplatelet medications is not desired.
J INVASIVE CARDIOL 2012;24(4):151-153
Key words: drug-eluting balloons, drug-coated balloons, percutaneous coronary intervention, in-stent restenosis, target lesion revascularization
__________________________________________
Drug-coated balloons (DCB) have been demonstrated to be successful for treatment of bare-metal stent (BMS) in-stent restenosis (ISR) with excellent long-term outcomes compared to standard uncoated balloon angioplasty1,2 and drug-eluting stents (DES).3
Although the results have been less impressive for treatment of small coronary arteries4 and bifurcations, they are often used for this indication.5 A very common reason to avoid stent implantation in patients undergoing coronary angioplasty is the concern regarding bleeding complications in patients with planned surgery, oral anticoagulation (atrial fibrillation or mechanical heart valves) or those with a history of previous bleeding complications on double-antiplatelet therapy with aspirin and thienopyridines.6
The aim of this study was to evaluate the safety and long-term efficacy of DCB in an unselected population of patients with stable coronary artery disease and acute coronary syndrome (ACS).
Methods
This is a single-center, non-randomized, prospective registry of patients treated in the Luzerner Kantonsspital, Luzern, Switzerland. The study was conducted from July 2009 until December 2010.
Patients. Suitable patients presenting with stable angina or ACS at our institution were included in this study. Patients with acute ST-elevation myocardial infarction and cardiogenic shock were excluded. We included patients with ISR and/or patients with planned surgery with a high risk of intraoperative bleed. Additionally, patients with relative or absolute contraindications for long-term antiplatelet treatment with aspirin and a thienopyridine (oral anticoagulation, previous history of bleeding) were included. A combination of aspirin and clopidogrel was given for 6 weeks and then clopidogrel was stopped. Consent was obtained from all patients for data gathering and regular telephone follow-up.
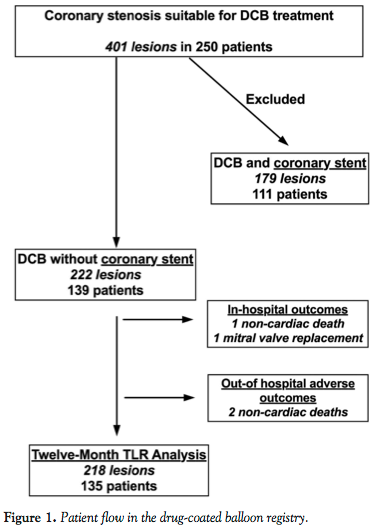 Percutaneous coronary intervention. The American Heart Association/American College of Cardiology classification was used to describe the treated lesions.7 Lesions were either pre-treated with conventional non-coated balloons or underwent direct treatment with the DCB. The In.Pact paclitaxel-coated balloon (Medtronic Vascular, Inc.) was used in all study patients. The balloons were inflated at the manufacturer-recommended pressures for 40 seconds. Patients in whom a stent was implanted during the same session (either electively or to achieve a better angiographic result) are excluded from this report (Figure 1).
Percutaneous coronary intervention. The American Heart Association/American College of Cardiology classification was used to describe the treated lesions.7 Lesions were either pre-treated with conventional non-coated balloons or underwent direct treatment with the DCB. The In.Pact paclitaxel-coated balloon (Medtronic Vascular, Inc.) was used in all study patients. The balloons were inflated at the manufacturer-recommended pressures for 40 seconds. Patients in whom a stent was implanted during the same session (either electively or to achieve a better angiographic result) are excluded from this report (Figure 1).
Outcomes. Outcomes were assessed by telephone or the patients were seen in the outpatient clinic. Our primary outcome was clinically driven target lesion revascularization (TLR) at 12 months. If coronary angiogram did not demonstrate an obstructive target lesion in patients with re-occurrence of angina, then this was not included in the primary outcome.
Statistics. Data are presented as means ± standard deviations (SD). The unpaired t-test was used to compare normally distributed parameters and the Mann-Whitney test was used to compared non-normally distributed parameters. P<.05 was considered significant. Statview, Version 5.0 (SAS Institute) and GraphPad PRISM, version 5 for Mac OS X were used for the statistical calculations.
Results
The study population consisted of 139 consecutive patients with a mean age of 69 ± 10 years who were treated with DCB balloons only. A total of 111 patients who additionally received a coronary stent in the same sitting were excluded from this analysis (Figure 1). In 5/111 patients (4.5%), implantation of coronary stent was necessary due to DCB-induced dissection. We did not observe other complications with use of DCB. Ninety-five patients (68%) had stable angina and 44 patients (32%) had ACS.
 De novo lesions and lesions with in-stent restenosis. In Table 1, patients with de novo lesions (n = 79, 128 lesions) are compared with ISR subjects (n = 60, 94 lesions). Age, sex, and cardiovascular risk factors were equally distributed between these two groups.
De novo lesions and lesions with in-stent restenosis. In Table 1, patients with de novo lesions (n = 79, 128 lesions) are compared with ISR subjects (n = 60, 94 lesions). Age, sex, and cardiovascular risk factors were equally distributed between these two groups.
Mean diameter stenosis was higher (77 ± 15% vs 69 ± 21%; P=.004) and reference vessel diameter lower (2.8 ± 0.5 mm vs 3.2 ± 0.4 mm; P<.0001) in the de novo group, but lesion length was longer in the ISR group (22.7 ± 9.9 mm vs 29.6 ± 12.9 mm; P<.0001). The de novo group had significantly fewer Type A lesions (5% vs 27%; P<.0001) and more lesions with B1, B2 characteristics (88% vs 70%; P=.002).
Characteristics of DCB and strategy for bifurcations. The diameter of DCB was smaller in patients with de novo lesions (2.8 ± 0.5 mm vs 3.1 ± 0.4 mm; P<.0001), but the balloons were longer in the ISR group (27.8 ± 8.0 mm vs 31.7 ± 7.7 mm; P=.0004).
The prevalence of bifurcations was higher in the de-novo group (34% vs. 16%, P=0.002) and kissing balloon technique was the preferred treatment method for both groups (73% in the de-novo and 93 % in the ISR group, P=0.15).
 12-month outcomes. The in-hospital outcome was complicated with 1 non-cardiac death and 1 patient underwent unplanned mitral-valve surgery. Data from 137 patients with 220 treated lesions were available for assessment of 12-month outcomes. At 12 months, there were 2 non-cardiac deaths, which left 135 patients with 218 lesions for analysis of TLR.
12-month outcomes. The in-hospital outcome was complicated with 1 non-cardiac death and 1 patient underwent unplanned mitral-valve surgery. Data from 137 patients with 220 treated lesions were available for assessment of 12-month outcomes. At 12 months, there were 2 non-cardiac deaths, which left 135 patients with 218 lesions for analysis of TLR.
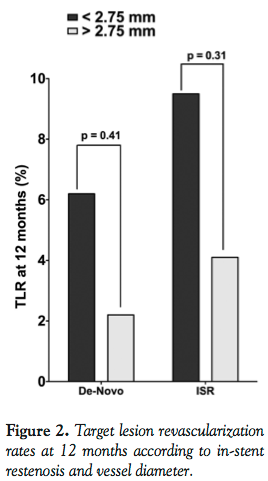
Clinically driven TLR was performed in 6/126 lesions (4.8%) in the de novo group and in 5/92 lesions (5.4%) in the ISR group (P=1.0). The 12-month TLR rates according to vessel diameter (< or > 2.75 mm) are shown in Figure 2. In the de novo group, TLR rate was 1/45 (2.2%) in patients with vessel diameter >2.75 mm and 5/81 (6.2%) in those with diameter <2.75 (P=.42). In the ISR group, TLR was 3/71 (4.2%) in patients with vessel diameter >2.75 mm and 2/21 (9.5%) in those with diameter <2.75 mm (P=.32).
There was no statistical difference in TLR rates between patients with diabetes and those without (2/43 [4.7%] vs 9/175 [5.1%]; P=1.0).
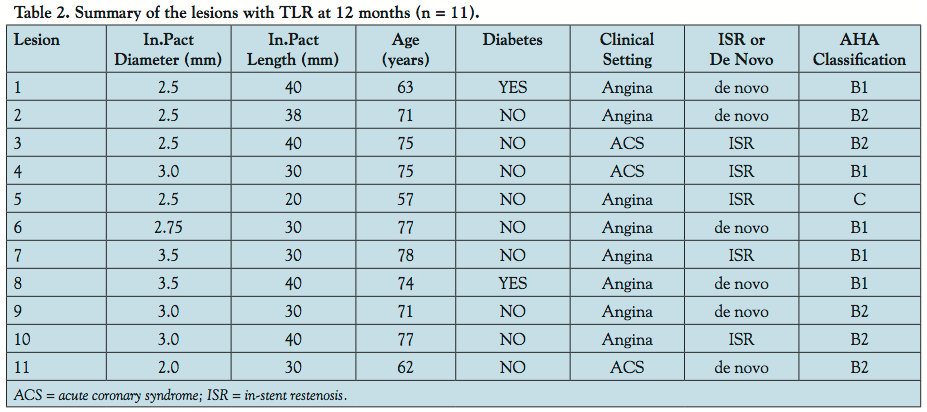 Clinical and lesions characteristics of those patients with TLR at 12 months (n = 11) are summarized in Table 2. None of the lesions was a type A lesion and most of the In.Pact balloons used had a diameter <3.0 mm (n = 9, 82%). Two patients with In.Pact balloons >3.0 mm had TLR; both had fairly long lesions (30 and 40 mm), and in 1, the lesion was an ISR.
Clinical and lesions characteristics of those patients with TLR at 12 months (n = 11) are summarized in Table 2. None of the lesions was a type A lesion and most of the In.Pact balloons used had a diameter <3.0 mm (n = 9, 82%). Two patients with In.Pact balloons >3.0 mm had TLR; both had fairly long lesions (30 and 40 mm), and in 1, the lesion was an ISR.
Angina status at 12 months. At 12 months, a total of 11 patients (8.1%) complained of angina, which was managed medically. In 5 patients (3.7%), an angiogram was performed but demonstrated non-obstructive coronary arteries. Five patients (3.7%) complained of atypical chest pain and 3 patients (2.2%) complained of shortness of breath. All these patients were successfully managed medically and none of them had a serious event (including major bleed) during the follow-up period.
Discussion
This reports describes characteristics and outcomes of a mixed population of patients who underwent treatment with the In.Pact DCB at our institution. DCB were used either to treat ISR or to avoid stent implantation because the patient needed urgent non-cardiac surgery or had a relative or absolute contraindication to long-term double antiplatelet therapy.
The results of this study demonstrate good overall outcomes of patients in whom the lesions were treated using DCB without the use of coronary stents. Clinically driven TLR was performed in 4.8% of the patients in the group with de novo lesions and in 5.4% of those with ISR. The rate of TLR in our population is slightly lower than the rate published in the PEPCAD II trial,3 but it is important to recognize that this was a mixed population including patients without a “classical” indication for the use of DCB (ISR or small vessels).
As previously demonstrated in other studies and shown in Figure 2, the rate of TLR is dependent on the presence of ISR and the diameter of the vessel. Although the results in our study are not statistically significant, the rates of TLR are highest in those patients with ISR and vessel diameter <2.75 mm.
The characteristics of the patients and lesions with TLR at 12 months are summarized in Table 2. Interestingly, none of the patients had a type A lesion and only 2 of them had diabetes. The diameter of the In.Pact balloon was rather small and most of them had a length >30 mm. Only 2 patients with In.Pact balloons >3.0 mm had a TLR and both had fairly long lesions (30 and 40 mm). Additionally, in 1 patient, the lesion was an ISR.
Study limitations. We are presenting the results of a registry and not a prospective randomized trial. The major limitations of this study are its single-center character and the small sample size. Additionally, the rates of TLR are low in our population compared to other studies, possibly due to the mix of the patients in this unselected group of patients. No significant difference in TLR rates was reached, possibly due to small sample size.
Conclusions
DCB are a good treatment option for patients with ISR and offer acceptable rates of TLR. Additionally, DCB can be an alternative to drug-eluting stents, if the use of long-term dual-antiplatelet medications is not desired.
References
- Scheller B, Hehrlein C, Bocksch W, et al. Treatment of coronary in-stent restenosis with a paclitaxel-coated balloon catheter. N Engl J Med. 2006;355(20):2113-2124.
- Tepe G, Zeller T, Albrecht T, et al. Local delivery of paclitaxel to inhibit restenosis during angioplasty of the leg. N Engl J Med. 2008;358(7):689-699.
- Unverdorben M, Vallbracht C, Cremers B, et al. Paclitaxel-coated balloon catheter versus paclitaxel-coated stent for the treatment of coronary in-stent restenosis. Circulation. 2009;119(23):2986-2994.
- Cortese B, Micheli A, Picchi A, et al. Paclitaxel-coated balloon versus drug-eluting stent during PCI of small coronary vessels, a prospective randomised clinical trial. The PICCOLETO study. Heart. 2010;96(16):1291-1296.
- Banning AP, Lim CC. Drug-eluting balloons: what is their place on the interventionalist’s shelf? Heart. 2010;96(16):1257-1258.
- Pfisterer M, Nietlispach F, Jeger R, Kaiser C. Drug-eluting coronary stents in clinical practice: lessons from the <<BAsel Stent Kosten-Effektivitats Trials>> (BASKET). A review of the BASKET trials. Swiss Med Wkly. 2011;141:W13263.
- Ryan TJ, Faxon DP, Gunnar RM, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association task force on assessment of diagnostic and therapeutic cardiovascular procedures (subcommittee on percutaneous transluminal coronary angioplasty). Circulation. 1988;78(2):486-502.
__________________________________________
From the 1Department of Cardiology, Luzerner Kantonsspital, Luzern, Switzerland and the 2Division of Geriatrics, Department of General Internal Medicine, Inselspital, Bern University Hospital and University of Bern, Switzerland.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 7, 2011, provisional acceptance given December 13, 2011, final version accepted January 20, 2012.
Address for correspondence: Paul Erne, MD, Professor of Cardiology, Department of Cardiology, Luzerner Kantonsspital, 6000 Luzern 16, Switzerland. Email: Paul.Erne@ksl.ch












