

Intervention in the Occluded Vein Graft: With High Risk Can Come Great Reward. Review of Techniques With Case Examples
Abstract: Total occlusion of a saphenous vein graft (SVG) can present as abrupt thrombotic occlusion in an atherosclerotic graft with resultant acute cardiac events or chronic total occlusion (CTO) with resultant angina symptoms. The risks of percutaneous coronary intervention (PCI) within an occluded graft include not only periprocedural myocardial infarction (MI), but also the risks that come part and parcel with any CTO intervention which include an increased probability of procedural failure, vessel perforation, dissection, high radiation, and contrast exposure, and the potential for worse outcomes. PCI of a chronically occluded graft remains a class III indication in current PCI guidelines because of the increased procedural risk and modest clinical data supporting improved outcomes. Acute-type occlusions, with bulky and thrombotic obstruction, while not specifically addressed in the guidelines, are also fraught with somewhat similar risks. In this review, we describe four case scenarios with occluded SVG and discuss challenges and techniques and available evidence that support these interventions.
J INVASIVE CARDIOL 2012;24(11):612-617
Key words: total occlusion, saphenous vein graft, fractional flow reserve
__________________________________________________________________
Saphenous vein grafts (SVGs) as coronary bypass conduits are limited by longitudinal attrition, as they begin to degenerate soon after they are exposed to systemic pressures, and have a known failure rate of 50% at the 10 year mark,1 with recurrence of symptoms in up to 20% of patients even in the first year.2 Several distinct processes contribute to graft failure, including early postoperative thrombosis, followed by accelerated accumulation of smooth muscle cells and extracellular material occurring in the months after implant (so-called neointimal hyperplasia), finally setting the stage for the classic atherosclerosis that dominates throughout the remainder of the life of the graft.3 It is the latter that is responsible for the vast majority of clinical cardiac events. Vein graft pathology differs, however, from native vessel disease insofar as there is usually friable atheroma or “grummus,” often lacking organized fibrous cap4 or compensatory positive remodeling, creating a proclivity for extensive distal emboli with manipulation by interventional equipment. It is this aspect of SVG disease that is thought to have contributed to the increased adverse events in early trials of percutaneous intervention (PCI).5
Total occlusion of an SVG can take many forms. Abrupt thrombotic occlusion in an atherosclerotic graft causes the majority of acute cardiac events. With the progression of time, however, one can expect the composition of the occluded plaque to progress from relatively soft material to increasingly fibrous hard plaque.6 The risks of PCI within an occluded graft include not only the periprocedural embolism as described above, producing the “no reflow” phenomenon and myocardial infarction (MI), but also the risks that come part and parcel with any chronic total occlusion (CTO) intervention, including an increased probability of procedural failure, vessel perforation, dissection, high radiation and contrast exposure, and the potential for worse outcomes. As a result of the increased procedural risk and modest clinical data supporting improved outcomes, PCI of a chronically occluded graft remains a class III indication in current PCI guidelines. Acute-type occlusions, with bulky and thrombotic obstruction, while not specifically addressed in the guidelines, are also fraught with risk, and have been shown to have lower PCI success rates and higher major adverse cardiac event (MACE) rates when compared to intervention within acutely occluded native vessels.7-9
The decision to perform PCI in the setting of a vein graft total occlusion is thus not one that should be taken lightly. There are many scenarios, however, that may favor PCI rather than medical therapy alone. Reasons to consider percutaneous intervention upon an occluded SVG may include acute infarction, refractory angina despite optimal medical therapy, grafts that subtend myocardium with demonstrable viability and/or ischemia (when native vessel recanalization is not possible), and when collaterals are present that demonstrate a patent target vessel. In these cases, PCI of a chronically occluded SVG may be more therapeutically valuable, and the benefits may outweigh the risk. Often, this will represent the only option (other than repeat bypass) after attempts to recanalize an occluded native vessel have failed. Repeat bypass also generates diminishing marginal returns with respect to symptomatic and clinical outcomes.10 New stent technology, along with the use of protection devices, has improved technical success and outcomes in SVG PCI.
In this presentation, we describe four different case scenarios of PCI within totally occluded vein grafts, two of which are acute thrombotic occlusions and two of which occurred in chronic, degenerated grafts. All cases were successful both procedurally and clinically, and all cases underline the challenges that can occur, necessitating extreme caution and attention to detail, and rapid reaction in the event of complication. All cases employ evidence-based techniques in SVG CTO, to the extent that evidence is available.
Case 1. “Butterfly in his chest:” SVG perforation
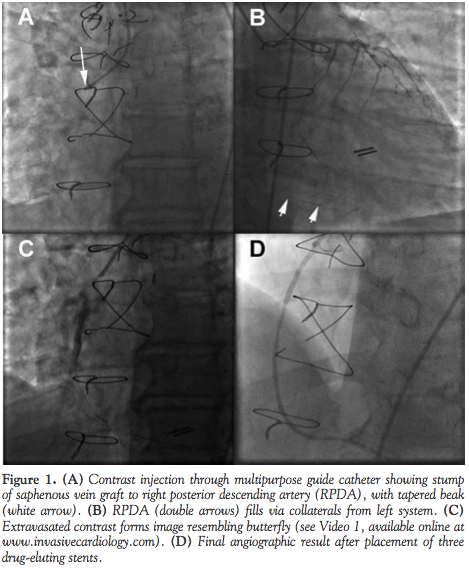 A 65-year-old man with diabetes, hypertension, chronic kidney disease (serum creatinine, 2.0 mg/dL), and history of 4-vessel coronary bypass grafting (CABG) 13 years earlier presented with non-ST segment elevation myocardial infarction (NSTEMI). Angiogram showed severe native coronary artery disease (CAD) with occluded left anterior descending (LAD), left circumflex (LCX), and right coronary artery (RCA) at their origins. The left internal mammary artery (LIMA) to LAD, and SVGs to the diagonal and obtuse marginal, were patent. The SVG to the RCA was occluded at the origin with a beak, with the right posterior descending artery (RPDA) opacifying via collaterals from the left system, suggesting it was freshly occluded and the culprit for the NSTEMI, and thus we proceeded with PCI (Figures 1A and 1B).
A 65-year-old man with diabetes, hypertension, chronic kidney disease (serum creatinine, 2.0 mg/dL), and history of 4-vessel coronary bypass grafting (CABG) 13 years earlier presented with non-ST segment elevation myocardial infarction (NSTEMI). Angiogram showed severe native coronary artery disease (CAD) with occluded left anterior descending (LAD), left circumflex (LCX), and right coronary artery (RCA) at their origins. The left internal mammary artery (LIMA) to LAD, and SVGs to the diagonal and obtuse marginal, were patent. The SVG to the RCA was occluded at the origin with a beak, with the right posterior descending artery (RPDA) opacifying via collaterals from the left system, suggesting it was freshly occluded and the culprit for the NSTEMI, and thus we proceeded with PCI (Figures 1A and 1B).
Unfractionated heparin (UFH) was used for anticoagulation. With support of an over-the-wire (OTW) 1.5 x 12 mm Apex balloon (Boston Scientific), a Pilot-150 guidewire (Abbott Vascular) was passed without difficulty through the graft into the RPDA, suggesting an acute, “soft” occlusion. Injection through the OTW balloon catheter confirmed intraluminal location. Passing the balloon catheter from the proximal to the distal end re-established TIMI 2 flow. A FilterWire EZ (Boston Scientific) was deployed at the distal portion of the graft. A 2.0 x 30 mm Trek Rx balloon (Abbott Vascular) was used to dilate the proximal graft at 13 atm. After dilatation, angiogram performed showed contrast extravasation at the inflation site (Video 1; all videos available at the end of this article and at www.invasivecardiology.com). Further contrast extravasation resulted in staining resembling a butterfly flapping its wings in the mediastinum (Figure 1C; Video 1-1). The patient developed chest pain with inferior ST elevation. Compromise to distal flow due to microembolism was suspected. The perforation was addressed by reversing UFH, and the same balloon was used to tamponade the graft at 2 atm. On brief deflation, a Balance-Middleweight (BMW) guidewire (Abbott Vascular) was passed to maintain distal access, and the filter basket was retrieved, with resolution of pain and ECG changes. Prolonged tamponade was performed for >4 minutes. Final angiography demonstrated no further extravasation, with TIMI 3 flow throughout the graft and RPDA. He remained hemodynamically stable throughout the case. Three days later, the patient was brought back for re-evaluation. His creatinine remained stable. Angiography demonstrated a patent graft with TIMI 3 flow. Fractional flow reserve (FFR) was measured at the level of the RPDA, with a baseline Pd/Pa of 0.90 and FFR of 0.65 with intracoronary adenosine. Three 2.5 x 28 mm Xience V drug-eluting stents (DESs; Abbott Vascular) were sequentially deployed proximally to distally. The final FFR was 0.87 with an excellent angiographic result (Figure 1D). The patient was discharged home 1 day later without incident, with the troponin peak of 6.31 ng/mL preceding the original intervention. On follow-up, he was free of angina.
Case 2. “Catch me if you can:” Large thrombus burden in an acute occlusion
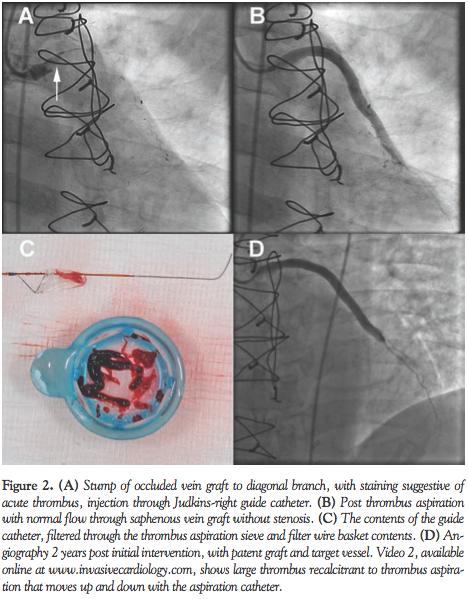 A 61-year-old man with a history of hypertension, hyperlipidemia, and 4-vessel CABG 1 year prior, presented with NSTEMI. Angiography demonstrated severe proximal LAD disease with the distal vessel filling from a patent LIMA graft, a 100% occluded major obtuse marginal and proximal RCA. The SVG to OM and SVG to RPDA were patent with good flow. The SVG to the diagonal-1 branch had 100% ostial thrombotic occlusion with persistence of contrast (Figure 2A).
A 61-year-old man with a history of hypertension, hyperlipidemia, and 4-vessel CABG 1 year prior, presented with NSTEMI. Angiography demonstrated severe proximal LAD disease with the distal vessel filling from a patent LIMA graft, a 100% occluded major obtuse marginal and proximal RCA. The SVG to OM and SVG to RPDA were patent with good flow. The SVG to the diagonal-1 branch had 100% ostial thrombotic occlusion with persistence of contrast (Figure 2A).
PCI commenced to the SVG to diagonal-1, as the course of the native vessel was not certain. UFH was used for anticoagulation. A 6 Fr Judkins right guide was used to intubate the SVG. A Pilot-50 guide wire (Abbott Vascular) passed easily to the distal part of the graft. Because of the significant thrombus burden, a Quick-Cat aspiration catheter (Spectranetics) was passed for multiple runs. A very large thrombus was visualized within the SVG (Figure 2B, Video 2) that moved up and down with passes of the aspiration catheter, but could not be aspirated. A FilterWire EZ was then placed, and further aspiration runs were utilized. The open basket was then carefully withdrawn through the proximal segment of the graft with the intent to capture the thrombus, and then withdrawn into the sheath and removed. To ensure that none of the contents of the basket remained in the guide, aspiration was performed to clear the guide catheter of any debris/thrombus. Aspiration resulted in sudden cessation of flow from the guide to the syringe. The guide catheter was disengaged, but still could not be aspirated, so the entire system was withdrawn. The catheter contents were filtered through the sieve (Figure 2C). A new guide was then placed, and final views were obtained, demonstrating a patent graft and target vessel, with TIMI 2 flow. After several doses of IC adenosine, TIMI 3 flow was restored, and stenting was not required. Dual antiplatelet therapy with aspirin and clopidogrel commenced. On follow-up angiogram 2 years later, the graft remained widely patent (Figure 2D).
Case 3. “My chest still hurts, Doc:” Large thrombus burden in a chronic occlusion
 An 80-year-old man with a history of 3-vessel CABG 12 years prior to PCI had Class III angina and dyspnea on minimal exertion. He had a defibrillator for ischemic cardiomyopathy (ejection fraction, 30%). Six months earlier, he had undergone PCI with DES for a focal stenosis in his SVG to the ramus intermedius, but angina was not relieved. Repeat angiogram re-demonstrated an occluded LAD at its origin, with patent LIMA retrogradely filling the LAD with an 80% ostially stenosed diagonal-1, a patent SVG to ramus, an occluded SVG to diagonal-1 branch (stable from 6 months prior), with minimal disease in the RCA (Figure 3A). As the diagonal territory remained the only distribution without adequate flow, we proceeded with antegrade PCI of the diagonal via the LAD, which was occluded prior to the diagonal branch.
An 80-year-old man with a history of 3-vessel CABG 12 years prior to PCI had Class III angina and dyspnea on minimal exertion. He had a defibrillator for ischemic cardiomyopathy (ejection fraction, 30%). Six months earlier, he had undergone PCI with DES for a focal stenosis in his SVG to the ramus intermedius, but angina was not relieved. Repeat angiogram re-demonstrated an occluded LAD at its origin, with patent LIMA retrogradely filling the LAD with an 80% ostially stenosed diagonal-1, a patent SVG to ramus, an occluded SVG to diagonal-1 branch (stable from 6 months prior), with minimal disease in the RCA (Figure 3A). As the diagonal territory remained the only distribution without adequate flow, we proceeded with antegrade PCI of the diagonal via the LAD, which was occluded prior to the diagonal branch.
UFH was used for anticoagulation. The attempt to access the ostial diagonal disease through the LAD CTO was not successful, with the wire ultimately entering the grafted ramus. PCI in the occluded SVG to diagonal commenced. A 6 Fr Amplatz left-1 guide was seated in the stump of the SVG to diagonal. An Asahi Miracle Bros 4 gram guidewire (Abbott Vascular) was carefully advanced through the stump, following the apparent curve of the vessel, and reaching the distal graft. A Pilot-150 guidewire was then advanced alongside the Miracle Bros, which was then removed. A 2.75 x 30 mm Apex balloon was used to perform multiple inflations to low pressure in the proximal body of the graft. Repeat views demonstrated restoration of TIMI 3 flow, with large thrombus burden (Figure 3B). Angiography captured an embolus migrating distally (Figure 3B; Video 3). A Guardwire distal protection device (Medtronic) was placed. With the Guardwire deployed, multiple aspiration passes were performed, removing a large amount of thrombus (Figure 3C) from the bulbous portion of distal segment of graft. Finally, a 2.75 x 18 mm Xience V DES was deployed in the proximal aspect of the vein graft at 20 atm (Figure 3D). Optical coherence tomography (OCT) was performed, demonstrating complete stent apposition in the newly deployed stent. Laminated as well as friable thrombus-like material was noted in both the bulbous portion of the graft and in the previous stent (Figures 3E and 3F). Postprocedurally, there was no troponin rise. The patient had resolution of angina at 1-month follow-up and increased exercise tolerance.
Case 4. Which vessel to treat? Using FFR to guide CTO SVG PCI
 A 64-year-old diabetic man with a history of hypertension, hyperlipidemia, 4-vessel CABG 17 years prior, and multiple PCIs presented with disabling angina with minimal exertion. Symptoms were refractory to an aggressive anti-anginal regimen, including beta-blockers, long-acting nitrates, and ranolazine. Angina progressed to rest angina, and he was admitted to the hospital. A nuclear stress test demonstrated inferior infarct with lateral wall ischemia. Angiogram demonstrated 100% occlusion of the proximal LAD and RCA, 30% in-stent restenosis of stent from LM into LCX, and 100% OM1 occlusion, the latter filling from collaterals from the OM2. The LIMA to LAD was patent, the SVGs to RPDA and D1 were patent, and the graft to the OM1 was occluded (Figure 4A), stable from angiography 6 years prior. Given severe, medical refractory angina, and ischemia in the lateral wall, the LM-LCX in-stent restenosis was interrogated with FFR, which was found to be in the normal range at 0.92. PCI in the occluded SVG to OM1 then commenced.
A 64-year-old diabetic man with a history of hypertension, hyperlipidemia, 4-vessel CABG 17 years prior, and multiple PCIs presented with disabling angina with minimal exertion. Symptoms were refractory to an aggressive anti-anginal regimen, including beta-blockers, long-acting nitrates, and ranolazine. Angina progressed to rest angina, and he was admitted to the hospital. A nuclear stress test demonstrated inferior infarct with lateral wall ischemia. Angiogram demonstrated 100% occlusion of the proximal LAD and RCA, 30% in-stent restenosis of stent from LM into LCX, and 100% OM1 occlusion, the latter filling from collaterals from the OM2. The LIMA to LAD was patent, the SVGs to RPDA and D1 were patent, and the graft to the OM1 was occluded (Figure 4A), stable from angiography 6 years prior. Given severe, medical refractory angina, and ischemia in the lateral wall, the LM-LCX in-stent restenosis was interrogated with FFR, which was found to be in the normal range at 0.92. PCI in the occluded SVG to OM1 then commenced.
The SVG to OM1 was intubated with an AL1 guide catheter. With support of a 1.5 x 12 mm Apex OTW balloon, a Pilot-150 wire was advanced carefully through the chronically occluded graft. Contrast injection through the balloon catheter confirmed distal intravascular location. A 300 cm BMW wire was exchanged, and further balloon angioplasty was performed using a 2.0 x 30 mm Apex balloon. FFR was now performed upon the graft with the pressure wire in the native OM1, demonstrating a value of 0.72. Two Cypher DESs (2.5 x 28 mm and 3.0 x 23 mm; Cordis Corporation) were then placed (Figure 4B). Final FFR was 0.92. The patient noted relief of angina. Two years later, he had recurrence of angina and repeat angiography demonstrated diffuse in-stent restenosis of the most proximal stent (Figure 4C). FFR was again reduced to 0.70. After repeat PCI with DES (Figure 4D), his angina was relieved.
Discussion and Review
When proceeding with intervention of an acutely occluded vein graft, as exemplified by Cases 1 and 2, there are many technical considerations that will improve success rates. A favorable lesion is one with an identifiable stump and a tapered end, with a staining pattern suggesting fresh thrombus, ideally with evidence for target vessel patency through either native vessel injection or collaterals. It is suggested that UFH without adjunctive glycoprotein IIb/IIIa inhibition be used to allow for anticoagulation reversal, should perforation develop. Despite the intuitive benefit of heightened anti-platelet therapy in heavy thrombus, it has not been shown to be helpful in vein graft cases, and IIb/IIIa use is currently a class III indication in SVG.7,11 Wire selection must also reflect the risk of perforation. Atraumatic, hydrophilic wires are ideal to first probe the graft, and can cross relatively easily in many cases. Examples of such wires include the Pilot series (Abbott Vascular), the ChoICE PT Floppy (Boston Scientific), and the Fielder family (Asahi Vascular).
Once the graft has been wired, ensuring intraluminal position is of paramount importance before further advancement of equipment and ballooning. In Case 1, before inflation, intraluminal position was confirmed with unresistive dottering throughout the length of the graft, and contrast injection through the OTW balloon catheter opacifying the distal vessel. Other strategies include gentle aspiration of arterial blood through a transit catheter or balloon, and obtaining an arterial waveform from a pressure wire, which can be exchanged distally once the lesion is crossed.
Embolic protection using Filterwire EZ was also employed in both acute cases, a strategy that is widely supported by data for both distal occlusion/thrombus-aspiration devices such as the GuardWire system,12 and distal filter devices such as the FilterWire or Spider Fx (eV3).13 We believe the impetus to use distal protection in occluded grafts, given the extensive thrombotic nature of the lesion, is very high. In non-occluded grafts, these devices have been shown to reduce 30-day MACE, including significant reductions in the individual endpoints of procedural myocardial infarction and no-reflow, and are a class I indication in the PCI guidelines.7 The Spider Fx may be of particular utility in the occluded graft, as it allows crossing of the lesion using the 0.014˝ wire of the operator’s choice, and delivery of the device with a proprietary delivery catheter. Case 2 is an extreme example of the amount of thrombus that can be extracted from an acutely occluded graft.
Once an adequate channel has been created to deliver stents, aggressive lesion modification with balloon angioplasty before placing stents is not recommended, in order to minimize the chance for emboli. When embolic events occur, resulting in slow or no-reflow, the operator should be facile in the use of pharmacologic treatment of no-reflow, including the use of intracoronary adenosine (as in Case 2), verapamil, and nitroprusside. The studies supporting use of verapamil in SVG interventions are in general small, but did in fact indicate improved TIMI flow and myocardial blush grades.14,15 In addition, intragraft administration of nicardipine has also been shown to ameliorate the no-reflow phenomenon.16
Case 1 was complicated by vein graft perforation, in an interesting butterfly pattern. Perforation is a rare but anticipated complication, which can be successfully treated in most cases by swift reversal of anticoagulation and use of prolonged balloon inflation, as it was in this case. An effective and reported next step would be the deployment of a covered stent.17 As the SVG diameter was <2.75 mm, Jostent Graftmaster (Abbott Vascular) was not used as an initial strategy in our case. It should be noted that vessel perforation in an SVG may actually be less prone to hemodynamic effects due to prior pericardectomy, and extrapericardial location of the SVG. However, the risk of acute blood loss remains significant, thus requiring immediate tamponade of the vessel. Sometimes following surgery, the pericardium is repaired with the notion that it will reduce the formation of adhesions, though this is not routinely performed. In case of unrepaired pericardium, there is a pseudo-space between the heart and pericardium laterally and posteriorly, and chest wall anteriorly. In this scenario, extravasated blood may still cause a compression of the cardiac chambers, leading to tamponade physiology.18
Data to support PCI for acute SVG occlusion remain sparse. One small case series in acutely occluded grafts in acute coronary syndrome, using contemporary techniques including DES and embolic protection, demonstrated high procedural success at 81%, but considerable 1- and 3-year mortality at 8% and 42%, respectively, and high repeat coronary revascularization of 38% at 3 years.19 Criticisms of this study include relatively infrequent use of embolic protection (25%) and DES (61%), and frequent use of rheolytic thrombectomy (39%), the latter having shown no benefit when compared with intragraft urokinase in the VeGAS 2 trial20 and harm in studies of acute MI.21 It is not surprising that, when compared to PCI within a native culprit artery in acute MI, the rate of MACE is higher when the intervened vessel is a vein graft, particularly when the periprocedural biomarkers are increased.22
Intervention of a chronically occluded vein graft, as in Cases 3 and 4, carries a separate set of clinical and technical challenges, more akin to native vessel CTO, and the distinction should be made before proceeding. First, attempting recanalization of the SVG CTO should be viewed as a last option, as the very characteristics that constitute a chronic total occlusion are the ones most predictive of 30-day MACE in the vein graft population at large; namely, angiographic degeneration, plaque volume, and lesion length.23 Note that in both CTO examples, medical management had been exhausted, and intervention in the native vasculature was taken as a first strategy. Until techniques for SVG CTO PCI improve, these are necessary steps. When attention was turned to the occluded graft in each case, AL1 guides were used (both were left grafts), in anticipation of the increased back-up that is required to deliver wires and balloons through the harder plaque. In a right graft, a multipurpose is the most coaxial, and is a reasonable choice. Again, as in the native CTO, the likelihood of ultimate success is better if a clear stump with a tapered end, rather than blunt end, can be identified.
CTO wires were also used from the beginning in each case, as lesion crossing can be expected to require more forward push. Choices for this purpose may include either hydrophilic wires, as mentioned earlier, or higher-force wires such as the Asahi Miracle Bros series (nonhydrophilic); Pilot 150 or 200 wires, PT Graphix intermediate or ChoICE PT Extra Support (hydrophilic); rarely requiring stiffer tapered wires such as Confianza (Abbott Vascular). The general strategy of graduating from moderate to increasingly stiff wires only as needed is recommended. If prior films of the patent graft are available, these should be reviewed, and actively compared to the course of the advancing wire. If a subintimal or non-luminal course is suspected, the wire can be left in place, and the parallel wire/see-saw technique24 employed with injection through an OTW balloon to confirm intraluminal passage. Once intraluminal position is assured, we again believe that embolic protection should be utilized if possible in order to achieve better outcomes, particularly as in Case 3, where heavy thrombus burden was visualized. In the CTO setting, placing embolic protection can be met with the challenges of high resistance to device passage, and lack of a clear requisite landing zone before graft touchdown, which is on the order 25-30 mm in the filter devices, and 9 mm in the Guardwire device.
In each of our cases requiring a stent, a DES was placed. In non-occlusive SVG intervention, use of DESs is generally accepted to improve MACE when compared with bare-metal stent (BMS). As might be expected, this is mostly driven by reduction in target lesion revascularization (TLR). The largest and most recent of such trials is the ISAR-CABG trial of 610 patients demonstrating 7.2% versus 13.1% TLR at 1 year favoring DES (P=.02).25 In the smaller RRISC trial (75 patients), DES impressively reduced binary in-stent restenosis in vein grafts from 30.6% to 11.3% at 6 months when compared with BMS, TLR from 21.6% to 5.3%, as well as lessened late lumen loss.26 A similarly impressive reduction in binary restenosis was found in the randomized SOS trial (88 patients), which compared paclitaxel-eluting stent versus BMS, with restenosis rates of 9% versus 51% at a median of 1.5 years, with significant reductions in TLR and graft failure as well.27 The apparent slight increase in stent thrombosis and late mortality with DES in the RRISC trial did not bear out in meta-analyses, which support a reduction in MACE, mortality, TLR, and no increased risk for thrombosis or MI with the use of DESs.28,29
It should be emphasized that the above results emanate from studies in non-total occlusions. In the true chronic SVG occlusion, outcomes for this strategy are not well established. In one series utilizing 95% DESs (mixed types) and 78% embolic protection devices, only 1 infarct occurred in the successfully revascularized patients at 1 year. Though TLR was high at 61%, re-stenting was usually achievable.30 In a real-world matched comparison of post-CABG patients with CTO, the Rotterdam Group demonstrated similar 3-year survival and TVR when comparing intervention within the graft CTO versus the native vessel.31 A small case series evaluated the use of paclitaxel DESs in SVG CTO, and found angiographic restenosis in 40% and TLR in 18% at 1 year.32 Confirmation of stent expansion with IVUS or OCT may be of benefit to reduce restenosis and/or stent thrombosis, as grafts can be large, and underexpansion/malapposition may be an even more powerful predictor for stent thrombosis in SVG than in native vessels.33,34
Finally, in Cases 1 and 4, FFR was utilized to guide intervention within the graft. This technique has been well validated in native arteries.35 While there are few data on the use of FFR in SVG and long-term outcomes, clearly the source of ischemia from SVG disease can be ascertained.36 In Case 4, the FFR value was consistent with ischemia, justifying the PCI. Had the graft in Case 4 been supplying infarcted tissue, the FFR could be expected to be in the normal range,37 and the benefit of PCI would be outweighed by the risk. Because by definition only viable tissue can be ischemic, this technique may prove useful prior to SVG PCI to discern whether the PCI is justifiable. Caution is advised, however, when interpreting what value can be taken as a cut-off to defer PCI, as this has not yet been delineated.
Vein graft intervention is high-risk endeavor, even if the lesion appears relatively straightforward and discrete, as there is a frequent association of bulky thrombus burden with the lesion. This index of caution is to be raised even higher in the diffuse disease of an occluded SVG, whether acute or chronic. Embolic infarctions occur, and are not benign, as periprocedural MI after SVG PCI has been shown to be associated with poorer outcomes, including mortality, even when the procedure itself is successful.38 Randomized data of conservative versus interventional therapy on SVG total occlusions are not available, and may never be, because not only is this a difficult population to study due to the inherent non-uniformity in the disease process and patient presentation, but there are low numbers at any given time. As such, the report of adverse events in case series cannot be taken as justification to refrain from all interventions in the occluded graft, as some have advocated.23 It may be the case that patients with diffusely diseased vein grafts simply represent a population with a greater disease burden and elevated comorbidity. The class III indication must be reconciled with the clinical scenario — the known limited longevity of vein grafts and higher risk/benefit ratio of re-operation, acute infarcts, refractory angina, and unrevascularized viable tissue. We have described four cases in which intervention improved anginal pain and quality of life. When the decision has been made to move forward with intervention, we believe embolic protection devices should be used in each case, if at all possible. DESs appear to carry benefit as compared with BMSs. One should anticipate complications, act quickly, and consider staging the procedure as necessary.
References
- Campeau L, Lesperance J, Hermann J, Corbara F, Grondin CM, Bourassa MG. Loss of improvement of angina between 1 and 7 years after aortocoronary bypass surgery. Circulation. 1979;60(2 Pt 2):1-5.
- Cameron AA, Davis KB, Rogers WJ. Recurrence of angina after coronary artery bypass surgery: predictors and prognosis (CASS Registry). J Am Coll Cardiol. 1995;4(4):895-899.
- Motwani JG, Topol EJ. Aortocoronary saphenous vein graft disease. Pathogenesis, predisposition, and prevention. Circulation. 1998;97(9):916-931.
- Zaman AG, Herath J. Percutaneous coronary intervention in saphenous vein graft disease. In: Essential Interventional Cardiology, 2nd Edition. Norell MS, Perrins EJ, Meier B, Lincoff AM (eds). W.B. Saunders, Philadelphia, Pennsylvania: 2008.
- de Feyter PJ, van Suylen RJ, de Jaegere PP, et al. Balloon angioplasty for the treatment of lesions in saphenous vein bypass grafts. J Am Coll Cardiol. 1993;21(7):1539-1549.
- Srivatsa SS, Edwards WD, Boos CM et al. Histologic correlates of angiographic chronic total coronary occlusions: influence of occlusion duration on neovascular channel patterns and intimal plaque composition. J Am Coll Cardiol. 1997;29(5):955-963.
- Levine GN, Bates ER, Blankenship JC, et al. ACC/AHA/SCAI guidelines for the performance of percutaneous intervention. J Am Coll Cardiol. 2011;58(24):E44-E122.
- Ergelen M, Uyarel H, Gul M, et al. Efficacy and outcome of primary percutaneous coronary intervention in patients with myocardial infarction due to saphenous vein graft occlusion. Kardiyol Dern Ar. 2010;38(8):531-536.
- Arzamendi D, Ly HQ, Tanguay JF, et al. Differential 1-year clinical outcomes for ST-segment elevation myocardial infarction related to stent thrombosis or saphenous vein graft thrombosis. Catheter Cardiovasc Interv. 2011 July 29. doi: 10.1002/ccd.23300. (Epub ahead of print).
- Cameron A, Kemp HG Jr, Green GE. Reoperation for coronary artery disease: 10 years of clinical follow-up. Circulation. 1998;78(3 Pt 2):1158-1162.
- Roffi M, Mukherjee D, Chew DP, et al. Lack of benefit from intravenous platelet glycoprotein IIb/IIIa receptor inhibition as adjunctive treatment for percutaneous interventions of aortocoronary bypass grafts: a pooled analysis of five randomized clinical trials. Circulation. 2002;106(24):3063-3067.
- Baim D, Wahr D, George B et al. Randomized trial of a distal embolic protection device during percutaneous intervention of saphenous vein aortocoronary bypass grafts. Circulation. 2002;105(11):1285-1290.
- Halkin A, Masud Z, Rogers C, et al. Six-month outcomes after percutaneous intervention for lesion in aortocoronary saphenous grafts using distal protection devices: results from the FIRE trial. Am Heart J. 2006;151(4):915.E1-E7.
- Michaels AD, Appleby M, Otten MH, et al. Pretreatment with intragraft verapamil prior to percutaneous coronary intervention of saphenous vein graft lesions: results of the randomized, controlled vasodilator prevention on no-reflow (VAPOR) trial. J Invasive Cardiol. 2002;14(6):299-302.
- Werner GS, Lang K, Kuehnert H, Figulla HR. Intracoronary verapamil for reversal of no-reflow during coronary angioplasty for acute myocardial infarction. Catheter Cardiovasc Interv. 2002;57(4):444-451.
- Fischell T, Haller S, Ashraf K. Intragraft nicardipine prophylaxis to prevent no-reflow in triple-vessel saphenous vein graft intervention. J Invasive Cardiol. 2005;17(6):334-337.
- Baruah DK. Covered stent to treat saphenous venous graft perforation — a case report. Catheter Cardiovasc Interv. 2010;76(6):844-846.
- Lowe R, Hammond C, Perry RA. Prior CABG does not prevent pericardial tamponade following saphenous vein graft perforation associated with angioplasty. Heart. 2005;91(8):1052.
- Abdel-karim, Banerjee S, Brilakis ES. Percutaneous intervention of acutely occluded saphenous vein grafts: contemporary techniques and outcomes. J Invasive Cardiol. 2010;22(6):253-257.
- Kuntz RE, Baim DS, Cohen DJ, et al. A trial comparing rheolytic thrombectomy prior to percutaneous intervention in diseases saphenous vein grafts, and thrombus-containing coronary arteries. J Am Coll Cardiol. 2003;42(11):2007-2013.
- Ali A, Cox D, Dib N, et al. Rheolytic thrombectomy with percutaneous coronary intervention for infarct size reduction in acute myocardial infarction: 30-day results from a multicenter randomized study. J Am Coll Cardiol. 2006;48(2):244-252.
- Galia MA Jr, Torguson R, Xue Z, et al. Outcomes of patients with acute myocardial infarction from a saphenous vein culprit undergoing percutaneous coronary intervention. Cathet Cardiovasc Interv. 2011;78(1):23-29.
- Lee MS, Park SJ, Kandzari DE et al. Saphenous vein graft intervention. JACC Cardiovasc Interv. 2011;4(8):831-843.
- Ochiai M, Ashida K, Araki H, Ogata N, Okabayashi H, Obara C. The latest wire technique for chronic total occlusion. Italian Heart J. 2005;6(6):489-493.
- Mehilli J, Pache J, Abdel-Wahab M, et al. Drug-eluting versus bare-metal stents in saphenous vein graft lesions (ISAR-CABG): a randomized controlled superiority trial. Lancet. 2011;378(9796):1071-1078.
- Vermeersch P, Agostini P, Verheye S, et al. Randomized double-blind comparison of sirolimus-eluting stent versus bare-metal stent implantation in diseased saphenous vein grafts: six months angiographic, intravascular ultrasound, and clinical follow-up of the RRISC Trial. J Am Coll Cardiol. 2006;48(12):2423-2431.
- Brilakis ES, Lichtenwalter C, de Lemos JA, et al. A randomized controlled trial of a paclitaxel-eluting stent versus a similar bare-metal stent in saphenous vein graft lesions the SOS (stenting of saphenous vein grafts) trial. J Am Coll Cardiol. 2009;53(11):919-928.
- Brilakis ES, Saeed B, Banerjee S. Drug-eluting stents in saphenous vein graft interventions: a systematic review. EuroIntervention. 2010;5(6):722-730.
- Wiisanen M, Abdel-Latif A, Mukherjee D, Ziada KM. Drug-eluting stents versus bare-metal stents in saphenous vein graft interventions: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;3(12):1262-1273.
- Al-Lamee R, Alfonso I, Latib A, et al. Clinical and angiographic outcomes after percutaneous recanalization of chronic total saphenous vein graft occlusion using modern techniques. Am J Cardiol. 2010;106(12):1721-1727.
- Meliga E, Garcia-Garcia HM, Kukreja N, et al. Chronic total occlusion treatment in post-CABG patients: saphenous graft versus native vessel recanalization — long-term follow-up in the drug-eluting stent era. Catheter Cardiovasc Interv. 2007;70(1):21-25.
- Jim MH, Ho HH, Ryan LY, et al. Paclitaxel-eluting stents for chronically occluded saphenous vein grafts (EOS) study. J Intervent Cardiol. 2010;23(1):40-44.
- Alfonso F, Suárez A, Pérez-Vizcayno MJ, et al. Intravascular ultrasound findings during episodes of drug-eluting stent thrombosis. J Am Coll Cardiol. 2007;50(21):2095-2097.
- Fusso RJ, Attubato MS, Davidson CJ, et al. Angiography versus intravascular ultrasound-directed stent placement: final results from AVID (Abstr). Circulation. 1999;100:I-234.
- Tonino PA, De Bruyne B, Pijls N, et al. Fraction flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360(3):213-224.
- Aqel R, Zoghbi GJ, Hage F, et al. Hemodynamic evaluation of coronary artery bypass graft lesions using fractional flow reserve. Catheter Cardiovasc Interv. 2008;72(4):479-485.
- Pijls N. Fractional flow reserve after previous myocardial infarction. Eur Heart J. 2007;28(19):2301-2302.
- Hong M, Mehran R, Dangas G, et al. Creatine kinase-MB elevation following successful saphenous vein graft intervention is associated with late mortality. Circulation. 1999;100(24):2400-2405.
_______________________________________________________
From the Department of Medicine, Division of Cardiology, Central Arkansas Veterans Healthcare System and University of Arkansas for Medical Sciences, Little Rock, Arkansas.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Sachdeva discloses that he serves on speaker bureaus for Volcano Corporation and St Jude Medical. Drs Cook and Uretsky have nothing to disclose.
Manuscript submitted March 22, 2012, provisional acceptance given April 10, 2012, final version accepted May 22, 2012.
Address for correspondence: Rajesh Sachdeva, MD, 4300 W. 7th Street, Little Rock, AR 72205. Email: rrsachdeva@gmail.com













