

Intra-Aortic Counterpulsation for Hemodynamic Support in Patients With Acute Ischemic Versus Non-Ischemic Heart Failure
Abstract: Background. Intra-aortic counterpulsation (IABP) is frequently applied to provide hemodynamic support in patients with refractory cardiogenic shock (CS) of ischemic and non-ischemic cause. However, clinical data comparing outcomes are lacking for both indications. The purpose of this analysis was to evaluate outcome and safety of IABP support in patients with ischemic and non-ischemic CS and to identify predictors of early mortality in this severely ill patient population. Methods and Results. For the period between 1998 to 2010, data from 489 consecutive patients (age, 67.2 ± 12.2 years; 65.9% male) who had received IABP support for CS at the University Heart Center Jena were retrospectively analyzed. The primary endpoint was overall mortality at 7 and 30 days. Secondary endpoints included the incidence of vascular and neurologic complications as well as long-term survival. Follow-up data on current health status of the patients were acquired either from health insurance records or based on patient and physician interviews. After data compilation, patients were assigned to one of the following subgroups: ST-elevation myocardial infarction (STEMI; n = 368; 75.3%), non-STEMI (n = 75; 15.3%) and congestive heart failure (CHF; n = 46; 9.4%). Of the 489 patients enrolled, 422 (86.4%) were successfully weaned from IABP support. However, a significantly lower proportion of patients were weaned successfully in the STEMI group (n = 310; 84.1%) compared to the other two groups (non-STEMI: n = 70, 92.4%; CHF: n = 45, 97.8%; P=.041). Overall mortality at 30 days was 36.4% (n = 178) and was not significantly different between the subgroups. Significant predictors of 30-day mortality included age >70 years (odds ratio [OR], 16.81; confidence interval [CI], 1.241-227.54), ejection fraction <40% (OR, 36.33; CI, 2.93-451.05) and mechanical ventilation (OR, 12.42; CI, 1.21-127.17). Long-term follow-up was 803 ± 1061 days (range, 0-1380 days), with a long-term survival rate of 38.3%. Conclusion. IABP represents a safe technology for hemodynamic support and is associated with low complication rates. Parameters relating to early mortality include age >70 years, respiratory failure requiring mechanical ventilation, and left ventricular function <40%, which represent an additional risk of death. However, the etiology of CS had no effect on mortality in this analysis. This observation should encourage physicians to apply IABP for hemodynamic support in patients with non-ischemic left ventricular failure.
J INVASIVE CARDIOL 2012;24(11):583-589
Key words: intra-aortic counterpulsation, cardiogenic shock, mechanical circulatory support
_____________________________________________________
Intra-aortic counterpulsation (IABP) is a widely used concept of circulatory support in patients with cardiogenic shock (CS). Introduced in 1962 to augment native cardiac function by afterload reduction and improvement of coronary perfusion, the method was applied clinically for the first time by Kantrowitz et al in 1968.1,2 Since then, IABP therapy has improved considerably and has evolved into a mature technique with more than 160,000 applications each year worldwide.3 Mechanical support using IABP in CS complicating acute myocardial infarction has a Class I guideline recommendation.4,5 However, it is also applied to provide hemodynamic support in CS for other, potentially irreversible causes of left ventricular (LV) dysfunction, such as refractory congestive heart failure. Despite the frequent use of IABP support for a wide range of serious cardiovascular conditions, in the literature, there are few data comparing the outcome of IABP support in CS between potentially reversible versus irreversible causes. Therefore, the purpose of this registry was to review our institutional experience with IABP-application in patients with CS from ST-elevation myocardial infarction (STEMI), non-STEMI, and refractory chronic heart failure (CHF) in order to assess safety and outcome, as well as to identify predictors of early mortality.
Methods
Study design and data collection. This clinical registry was established in order to analyze procedural characteristics and outcomes of patients receiving hemodynamic support using IABP based upon 13 years of institutional experience with this treatment modality. Data were collected from medical records at the University Heart Center Jena between 1998 and 2010. Eligible patients were identified from the hospital’s electronic information system by searching for the keywords “intra-aortic counterpulsation,” “IABP,” and “cardiogenic shock.” Electronic records and hard-copy files were then reviewed by a cardiologist for retrieval of demographic, procedural, and laboratory data (peak cardiac enzyme levels, creatine kinase, serum creatinine, c-reactive protein). For all patients included, the APACHE II score was calculated as a marker of disease severity. For early and long-term follow-up, multiple sources were exploited: medical records, if available, public records, health insurance data, as well as patient and physician interviews. Finally, this study was approved by the institutional review board. Registry design, anonymous acquisition, and publication of data were performed according to the Declaration of Helsinki.
Inclusion criteria and treatment. The records of all patients meeting the above criteria were reviewed and patients who had received acute IABP support for CS were included in the analysis. In these patients, diagnosis of CS was based on the definition from the SHOCK trial, which included: (1) the presence of systolic blood pressure equal to or below 90 mm Hg for at least 30 minutes; (2) administration of vasopressors required to maintain blood pressure >90 mm Hg; (3) evidence of end-organ hypoperfusion (eg, urine output <30 mL or cold, diaphoretic extremities, or altered mental status); and (4) evidence of elevated filling pressures (eg, pulmonary congestion on examination or chest radiograph).6 In each patient, drug therapy and interventional treatment were tailored to the rapidly changing hemodynamic status and included mechanical ventilation and pharmacologic treatment (inotropes, vasopressors). The decision to institute IABP support was made at the discretion of the treating cardiologist, usually at the time of primary coronary angiography. The diagnosis of STEMI or acute coronary syndrome was based on coronary angiography examination, laboratory results (elevation troponin I >1.5 ng/mL) and electrocardiographic studies (ST-segment elevation in two or more contiguous leads). Chronic heart failure as cause of CS was diagnosed in patients with systolic LV dysfunction from causes other than acute myocardial ischemia, such as dilated cardiomyopathy and hypertensive or valvular heart disease.
Institution of intra-aortic counterpulsation. The implanted balloon size was chosen according to the manufacturers (IABP System 97; Datascope and Arrow International, Inc) recommendations based on patient height. If the patient was taller than 165 cm, a 40 mL balloon was implanted. For those between 155-165 cm and <155 cm in height, balloons of 35 mL and 30 mL were chosen, respectively. Implantation was performed via a 8 Fr femoral sheath under fluoroscopic or echocardiographic guidance either in the catheter laboratory or the intensive care unit. For hemodynamic support, the device was set on 1:1 augmentation and inflation and deflation were timed to achieve maximum diastolic pressure augmentation. After hemodynamic improvement, the augmentation rate was reduced and the patient was eventually weaned from support.
Study endpoints. The primary endpoint of the study was all-cause mortality at 7 and 30 days in each subgroup of CS. The secondary endpoints evaluated the incidence of neurologic complications, vascular complications in association with IABP implantation, as well as long-term survival.
Cerebrovascular complications occurring during hospital treatment were either classified as transient ischemic attack (TIA) or stroke. The diagnosis of TIA was defined as complete resolution of neurological symptoms within 24 hours and a normal neuroimaging study. In contrast, diagnosis of stroke was based upon persisting neurological symptoms >24 hours, or appropriate new computed tomography (CT) or magnetic resonance imaging (MRI) findings. Acute kidney injury was staged according to the modified RIFLE (risk, injury, failure, loss, and end-stage kidney disease) classification (Table 2), which has been validated in the intensive care and cardiac surgical settings.7-11 Major vascular complications were defined as loss of pulse or sensation, pallor, or bleeding requiring surgical intervention. Minor vascular complications were defined as diminished pulse resolving with balloon removal and minor hematomas not requiring blood transfusion or surgical intervention. Kaplan-Meier curves were plotted for each etiology of CS.
Statistics. Continuous data are presented as mean ± standard deviation (SD) and categorical variables as percentages and numbers. All variables were tested for normal distribution using the Shapiro-Wilk test. Univariate logistic regression was performed among established predictors of 30-day mortality. Age was dichotomized to above and below the median of 70 years. Ejection fraction and durations of mechanical ventilation and IABP support were dichotomized to above and below 40% and 72 hours, respectively. APACHE II score at hospital admission was dichotomized to above and below the median of 17 mmol/L. All covariates with a P-value of <.1 were included in the multivariate regression model. Backward stepwise logistic regression analysis was subsequently performed to identify independent predictors for 30-day mortality. A covariate was removed from the model if the P-value was >.10. All P-values <.05 were considered statistically significant. Kaplan-Meier curves were constructed for the following survival functions: etiology of CS substratified for STEMI, non-STEMI and CHF, age above and below 70 years, ejection fraction above and below 40%, and the requirement of mechanical ventilation. Survival differences were tested using the log-rank statistic. All statistical analyses were performed with the Statistical Package for the Social Sciences (version 18.0; SPSS Inc).
Results
Patient characteristics at hospital admission. In the period from 1998 to 2010, intra-aortic counterpulsation was instituted in a total of 533 patients. Of this population, 489 patients received circulatory support for severe CS and were included in this registry. Another frequent indication for institution of IABP was elective left-main PCI (LMS-PCI; n = 44); however, these patients were excluded from the present analysis. Patients included in the registry were stratified to 3 different subgroups depending on etiology of CS: STEMI (n = 368; 75.3%), non-STEMI (n = 75; 15.3%), and CHF (n = 46; 9.4%).
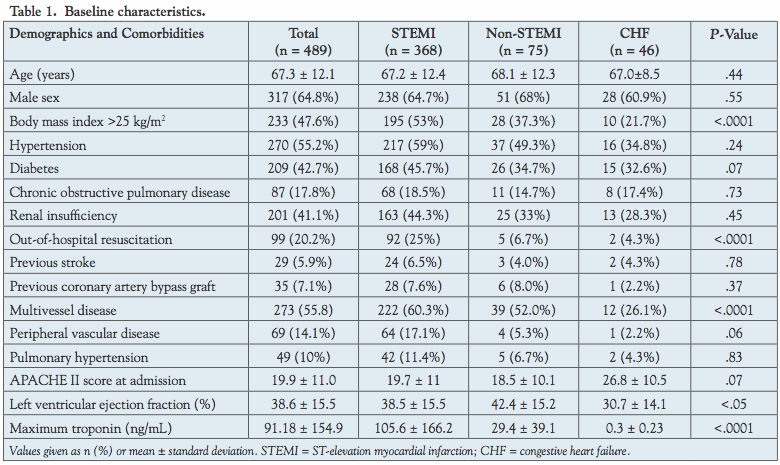 Baseline characteristics are further detailed in Table 1. In the overall study population, the mean age was 67.6 ± 12.2 years and 351 patients (65.9%) were male. Concomitant diseases included type 2 diabetes mellitus in 230 (43.2%), renal insufficiency in 218 (40.9%), arterial hypertension in 302 (56.7%), and COPD in 96 (18.0%) patients. Furthermore, 39 patients (7.3%) had previously undergone open heart surgery. Left ventricular ejection fraction (LVEF; defined by either echocardiography or ventriculography) was moderately reduced (0.39 ± 0.16%). In addition, 99 of the patients (20.2%) had received out-of-hospital resuscitation (OH-CPR) prior to hospital admission. The proportion of patients requiring OH-CPR was significantly higher in the STEMI subgroup (n = 92; 25%) versus patients with non-STEMI (n = 5; 6.7%) and CHF (n = 2; 4.3%; P<.0001). LVEF was significantly lower in the CHF group (30.7 ± 14.1%) compared to patients with STEMI (38.5 ± 15.5%) and non-STEMI (42.4 ± 15.2; P<.05). All other demographic variables were not significantly different between the subgroups.
Baseline characteristics are further detailed in Table 1. In the overall study population, the mean age was 67.6 ± 12.2 years and 351 patients (65.9%) were male. Concomitant diseases included type 2 diabetes mellitus in 230 (43.2%), renal insufficiency in 218 (40.9%), arterial hypertension in 302 (56.7%), and COPD in 96 (18.0%) patients. Furthermore, 39 patients (7.3%) had previously undergone open heart surgery. Left ventricular ejection fraction (LVEF; defined by either echocardiography or ventriculography) was moderately reduced (0.39 ± 0.16%). In addition, 99 of the patients (20.2%) had received out-of-hospital resuscitation (OH-CPR) prior to hospital admission. The proportion of patients requiring OH-CPR was significantly higher in the STEMI subgroup (n = 92; 25%) versus patients with non-STEMI (n = 5; 6.7%) and CHF (n = 2; 4.3%; P<.0001). LVEF was significantly lower in the CHF group (30.7 ± 14.1%) compared to patients with STEMI (38.5 ± 15.5%) and non-STEMI (42.4 ± 15.2; P<.05). All other demographic variables were not significantly different between the subgroups.
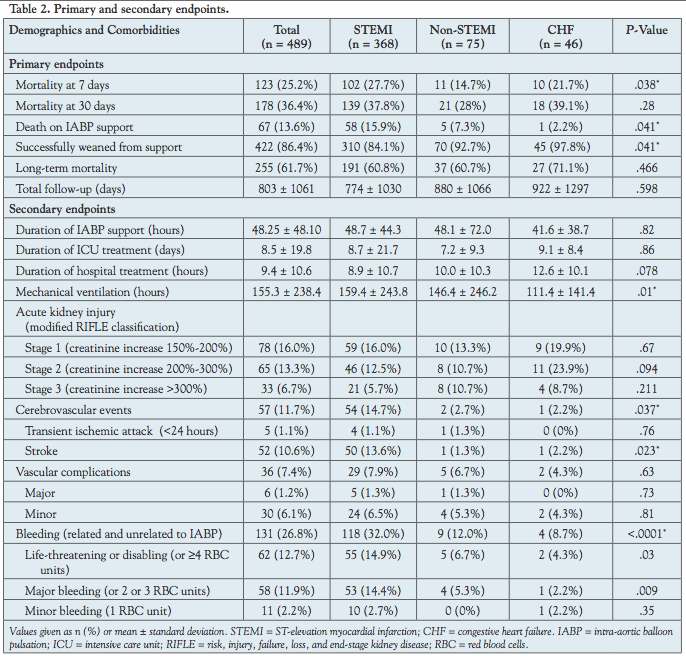 Primary endpoint and predictors of early mortality. Overall mortality in the study cohort was 25.3% (n = 123) and 36.4% (n = 178) at 7 days and 30 days, respectively (Table 2). In patients suffering from non-STEMI, mortality at 7 days (n = 11; 14.7%) was significantly lower compared to patients with STEMI (n = 102; 27.7%) and CHF (n = 10; 21.7%; P=.038). However, at 30 days, no difference in mortality was observed between the groups (STEMI 37.8% vs non-STEMI 28% vs CHF 39.1%; P=.28).
Primary endpoint and predictors of early mortality. Overall mortality in the study cohort was 25.3% (n = 123) and 36.4% (n = 178) at 7 days and 30 days, respectively (Table 2). In patients suffering from non-STEMI, mortality at 7 days (n = 11; 14.7%) was significantly lower compared to patients with STEMI (n = 102; 27.7%) and CHF (n = 10; 21.7%; P=.038). However, at 30 days, no difference in mortality was observed between the groups (STEMI 37.8% vs non-STEMI 28% vs CHF 39.1%; P=.28).
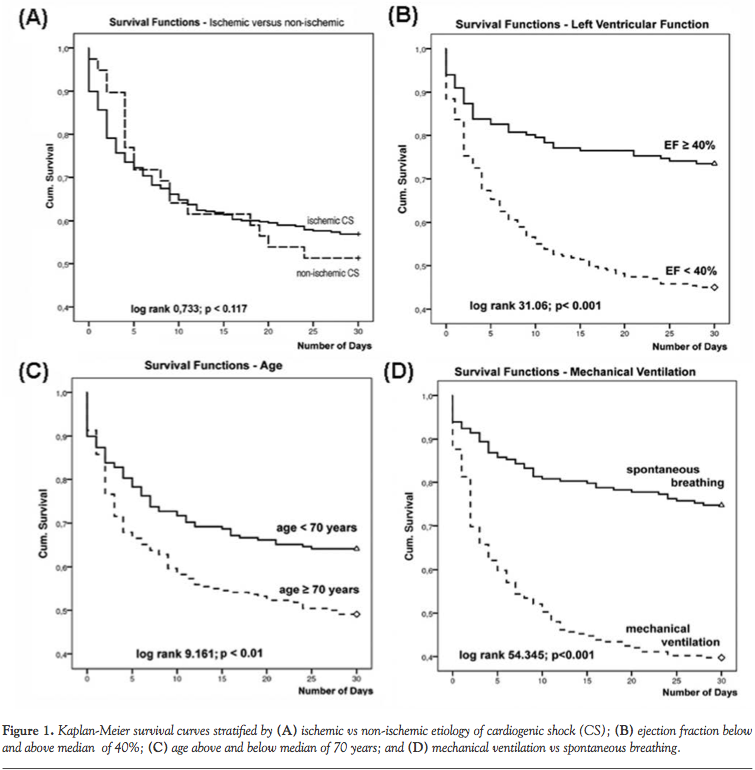
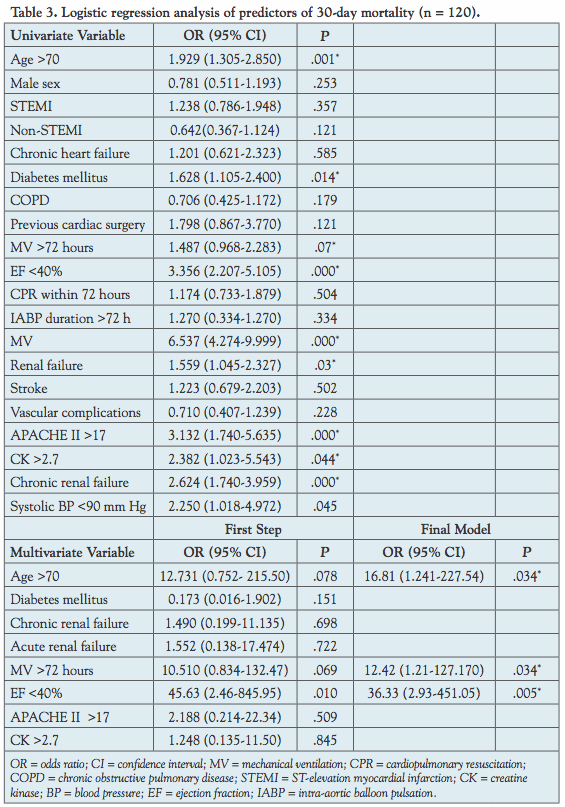 Multivariate logistic regression analysis was performed for identification of mortality predictors (Table 3). Following stepwise backward analysis, the parameters age >70 years (odds ratio [OR], 16.81; confidence interval [CI], 1.241-227.54; P=.034), mechanical ventilation (OR, 12.42; CI, 1.21-127.17; P=.034), and ejection fraction <40% (OR, 36.33; CI, 2.93-451.05; P=.005) remained in the model and were determined as independent predictors for 30-day mortality. Kaplan-Meier curves of 30-day survival are provided in Figure 1 and sub-stratified for different etiologies of CS (Figure 1A), as well as the predictors of 30-day mortality age (Figure 1B), left ventricular function <40% (Figure 1C), and mechanical ventilation (Figure 1D). Long-term follow-up was successfully obtained in 84.5% of all patients after a follow-up time of 803 ± 1061 days. Long-term mortality was 61.7% (n = 255) in the overall study population; however, no differences between the different etiologies of CS were seen (Table 2).
Multivariate logistic regression analysis was performed for identification of mortality predictors (Table 3). Following stepwise backward analysis, the parameters age >70 years (odds ratio [OR], 16.81; confidence interval [CI], 1.241-227.54; P=.034), mechanical ventilation (OR, 12.42; CI, 1.21-127.17; P=.034), and ejection fraction <40% (OR, 36.33; CI, 2.93-451.05; P=.005) remained in the model and were determined as independent predictors for 30-day mortality. Kaplan-Meier curves of 30-day survival are provided in Figure 1 and sub-stratified for different etiologies of CS (Figure 1A), as well as the predictors of 30-day mortality age (Figure 1B), left ventricular function <40% (Figure 1C), and mechanical ventilation (Figure 1D). Long-term follow-up was successfully obtained in 84.5% of all patients after a follow-up time of 803 ± 1061 days. Long-term mortality was 61.7% (n = 255) in the overall study population; however, no differences between the different etiologies of CS were seen (Table 2).
 Secondary endpoint and clinical course. Mean duration of IABP support in the overall population was 48.25 ± 48.10 hours and was not significantly different between the groups. In the overall population, 422 patients (86.4%) were successfully weaned from IABP support. The proportion of patients weaned successfully in the STEMI subgroup (n = 310; 84.1%) was significantly lower compared to patients with non-STEMI (n = 70; 92.4%) and CHF (n = 45; 97.8%; P=.041).
Secondary endpoint and clinical course. Mean duration of IABP support in the overall population was 48.25 ± 48.10 hours and was not significantly different between the groups. In the overall population, 422 patients (86.4%) were successfully weaned from IABP support. The proportion of patients weaned successfully in the STEMI subgroup (n = 310; 84.1%) was significantly lower compared to patients with non-STEMI (n = 70; 92.4%) and CHF (n = 45; 97.8%; P=.041).
In patients receiving IABP support for STEMI, a significantly higher rate of neurologic complications including TIA and stroke was observed (STEMI 11.7% vs non-STEMI 14.7% vs CHF 2.7%; P=.037). Strokes occurred more frequently in the STEMI subgroup (13.6%) than in patients with non-STEMI (1.3%) and CHF (2.2%; P=.023).
The rate of vascular complications associated with IABP insertion was generally low and did not show statistically significant differences between the groups. Major vascular complications (eg, bleeding, limb ischemia) at the site of IABP insertion occurred in 6 patients (1.2%), minor complications (eg, hematoma) were observed in 30 patients (6.1%). In the overall population, 212 patients (61.8%) required mechanical ventilation because of respiratory failure or post-cardiopulmonary resuscitation. The mean duration of respirator support was 155.3 ± 238.4 hours with a significantly longer duration of mechanical ventilation in patients with STEMI (159.4 ± 243.8 hours) vs non-STEMI (146.4 ± 246.2 hours) and CHF (111.4 ± 141.4 hours; P=.01). Newly developed renal dysfunction was observed in a total of 176 patients (36%), with the majority of patients experiencing stage 1 acute kidney injury. Stage 3 renal failure (creatinine increase >300%) occurred in a total of 33 patients (6.7%), without a significant difference between subgroups (Table 2).
Discussion
Since the pioneering work of Kantrowitz et al, intra-aortic counterpulsation has become a standard technique for circulatory support in patients with cardiogenic shock.1 The hemodynamic effects of IABP support are well documented and involve augmentation of coronary and systemic perfusion and reduction of left ventricular afterload.12
Due to its easy application, IABP is frequently applied to provide urgent hemodynamic support for CS for both ischemic and non-ischemic causes.13,14 IABP application is recommended by current guidelines in patients with acute myocardial infarction (AMI). However, evidence from randomized clinical trials supporting IABP use in acute ischemic or non-ischemic heart failure is still lacking.13 Early mortality in patients with CS from AMI has improved significantly with emergency revascularization. In contrast, non-ischemic heart failure still has a particularly poor prognosis due to the lack of causative treatment options. Also, evidence for IABP use in this condition is scant.6 In patients with refractory non-ischemic heart failure, IABP may be applied as a temporary bridge for recovery of cardiac function or before upgrading to other devices. The purpose of the present report was to analyze early and long-term outcomes of IABP support in CS from ischemic versus non-ischemic causes based upon data of a single-center registry. To date, this is the first analysis to compare intra-aortic counterpulsation in unselected “all-comers” with ischemic and non-ischemic heart failure.
Early and long-term mortality in patients with ischemic versus non-ischemic CS. Among the different etiologies of CS included in this study, patients with STEMI had the highest mortality at 7 days (STEMI: n = 102 [27.7%]; non-STEMI: n = 11 [14.7%]; and CHF: n = 10 [21.7%]). This difference in very early mortality can be explained by the high-risk profile in this group, which is also reflected by the significantly higher proportion of patients requiring out-of-hospital CPR. However, at 30 days and during long-term follow-up, no significant mortality difference was observed between the groups (STEMI 37.8% vs non-STEMI 28% vs CHF 39.1% and STEMI 60.8% vs non-STEMI 60.7% vs CHF 71.1%, respectively; P=.47).
The 30-day mortality in the STEMI group compares favorably to the results of other studies in patients with cardiogenic shock.15,16 In a recently published report by Cheng et al reviewing outcomes of IABP treatment in patients with CS and STEMI, the authors reported a 30-day mortality rate of 42%.17 The superior outcome observed in our study might be influenced by the more recent patient series in which a higher proportion of patients received early revascularization with primary PCI. However, it is important to note that despite revascularization, there was no survival benefit in patients with STEMI compared to patients with non-ischemic heart failure.
In the present study, three characteristic variables, namely, (1) age ≥70 years; (2) mechanical ventilation; and (3) LVEF <40%, were identified as independent predictors for early death. Patient age has been demonstrated in the SHOCK trial6 to be an established predictor of mortality in patients with CS. In this trial, patients ≥70 years (P=.034) had a significantly higher mortality even under IABP support than younger patients. Another independent predictor for mortality in our study was a LVEF <40%, which contributes to the shock cascade by the reduced cardiac output.23,24 Further, the predictive value of mechanical ventilation for early mortality is in agreement with other studies reporting mechanical ventilation as an independent prognostic factor. In patients with CS, Koreny et al observed mortality rates ranging from 54% in patients without respiratory failure to 84% with mechanical ventilation.18
Interestingly, the etiology of CS had no effect on early and long-term survival. Furthermore, the established predictors of early mortality in cardiovascular disease, such as diabetes mellitus, arterial hypertension, renal failure, or COPD, had no impact on survival in the present analysis.19,20 The lack of predictive value of these established parameters suggests a particularly high-risk profile of patients with CS included in this study with a greater imminent risk of death.
IABP-associated complication rate. In the present study, we observed a very low rate of IABP-associated vascular complications (1.2%), which compares favorably to data previously reported.14 The rate of vascular complications in the overall group was low and not significantly different between the subgroups. Major vascular complications (eg, bleeding, limb ischemia) occurred in 6 patients (1.2%) and minor complications (eg, hematoma) were observed in 30 patients (6.1%), respectively. Historically, IABP application has been associated with a rate of vascular complication as high as 27.5%.21 More recently, the incidence of major vascular complications reported in the literature has decreased to 2.8%.14 Another registry demonstrated a higher rate of vascular complications when arterial sheaths were used for balloon insertion.28 Furthermore, Manord et al demonstrated a higher rate of IABP-related vascular complications along with a prolonged duration of IABP support.22 In the latter study, the mean time of IABP support was 23.2 days, in contrast to 48.25 ± 48.10 hours in the present investigation.
Furthermore, we observed a significantly higher rate of cerebrovascular events in the STEMI subgroup. However, this observation can most likely be explained by the significantly higher number of patients requiring out-of-hospital CPR in this subgroup. This aspect should not be valued as an IABP-related complication, but rather marks the high-risk profile of this subgroup.
Conclusion
In current practice, IABP can be considered a safe technique for circulatory support and is rarely associated with complications. However, although outcomes of patients with CS have improved over the past two decades due to early revascularization strategies, early mortality remains high in patients with CS. This can most likely be attributed to the critically ill status of patients receiving IABP support in this real-world registry. In these patients, age >70 years, respiratory failure requiring mechanical ventilation, and LVEF <40% represent an additional risk of death. In contrast, etiology of CS had no effect on mortality in the current experience. Although verification by further clinical data is required, this observation should encourage physicians not to refrain from IABP implantation in patients with non-ischemic LV failure.
Study limitations. Several limitations of this analysis should be acknowledged. First of all, the lack of a control group (typical for a registry) hampers definite conclusions on efficacy of IABP support. Furthermore, due to the retrospective nature of data collection, detailed hemodynamic data after IABP implantation are not available. The accessibility of data was limited to standard parameters recorded during clinical routine. Finally, patients were included retrospectively over a period of 13 years, which also covers the learning curve and technology advances in use of the IABP during the observational period.
References
- Kantrowitz A, Tjonneland S, Freed PS, Phillips SJ, Butner AN, Sherman JL, Jr. Initial clinical experience with intra-aortic balloon pumping in cardiogenic shock. JAMA. 1968;203(2):113-118.
- Moulopoulos SD, Topaz S, Kolff WJ. Diastolic balloon pumping (with carbon dioxide) in the aorta — a mechanical assistance to the failing circulation. Am Heart J. 1962;63:669-675.
- Koenig SC, Litwak KN, Giridharan GA, et al. Acute hemodynamic efficacy of a 32-mL subcutaneous counterpulsation device in a calf model of diminished cardiac function. ASAIO J. 2008;54(6):578-584.
- Van de Werf F, Bax J, Betriu A, et al. Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2008;29(23):2909-2945.
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). Circulation. 2004;110(9):E282-E292.
- Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341(9):625-634.
- Lameire N, Van Biesen W, Vanholder R. The changing epidemiology of acute renal failure. Nat Clin Pract Nephrol. 2006;2(7):364-377.
- Uchino S, Bellomo R, Goldsmith D, Bates S, Ronco C. An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit Care Med. 2006;34(7):1913-1917.
- Bell M, Liljestam E, Granath F, Fryckstedt J, Ekbom A, Martling CR. Optimal follow-up time after continuous renal replacement therapy in actual renal failure patients stratified with the RIFLE criteria. Nephrol Dial Transplant. 2005;20(2):354-360.
- Abosaif NY, Tolba YA, Heap M, Russell J, El Nahas AM. The outcome of acute renal failure in the intensive care unit according to RIFLE: model application, sensitivity, and predictability. Am J Kidney Dis. 2005;46(6):1038-1048.
- Kuitunen A, Vento A, Suojaranta-Ylinen R, Pettila V. Acute renal failure after cardiac surgery: evaluation of the RIFLE classification. Ann Thorac Surg. 2006;81(2):542-546.
- Scheidt S, Wilner G, Mueller H, et al. Intra-aortic balloon counterpulsation in cardiogenic shock. Report of a co-operative clinical trial. N Engl J Med. 1973;288(19):979-984.
- Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Catheter Cardiovasc Interv. 2009;74(7):E25-E68.
- Ferguson JJ 3rd, Cohen M, Freedman RJ Jr, et al. The current practice of intra-aortic balloon counterpulsation: results from the Benchmark Registry. J Am Coll Cardiol. 2001;38(5):1456-1462.
- Cheng JM, Valk SD, den Uil CA, et al. Usefulness of intra-aortic balloon pump counterpulsation in patients with cardiogenic shock from acute myocardial infarction. Am J Cardiol. 2009;104(3):327-332.
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119(9):1211-1219.
- Cheng JM, den Uil CA, Hoeks SE, et al. Percutaneous left ventricular assist devices vs. intra-aortic balloon pump counterpulsation for treatment of cardiogenic shock: a meta-analysis of controlled trials. Eur Heart J. 2009;30(17):2102-2108.
- Koreny M, Karth GD, Geppert A, et al. Prognosis of patients who develop acute renal failure during the first 24 hours of cardiogenic shock after myocardial infarction. Am J Med. 2002;112(2):115-119.
- Gol MK, Bayazit M, Emir M, Tasdemir O, Bayazit K. Vascular complications related to percutaneous insertion of intra-aortic balloon pumps. Ann Thorac Surg. 1994;58(5):1476-1480.
- Barnett MG, Swartz MT, Peterson GJ, et al. Vascular complications from intra-aortic balloons: risk analysis. J Vasc Surg. 1994;19(1):81-87; discussion 87-89.
- Busch T, Sirbu H, Zenker D, Dalichau H. Vascular complications related to intraaortic balloon counterpulsation: an analysis of ten years experience. Thorac Cardiovasc Surg. 1997;45(2):55-59.
- Manord JD, Garrard CL, Mehra MR, et al. Implications for the vascular surgeon with prolonged (3 to 89 days) intraaortic balloon pump counterpulsation. J Vasc Surg. 1997;26(3):511-515; discussion 515-516.
_________________________________________________
From 1University Heart Center Jena, Department of Cardiology, Jena, Germany and 2Institute for Clinical Chemistry and Laboratory Medicine, Jena University Hospital, Jena, Germany.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 5, 2012 and accepted May 22, 2012.
Address for correspondence: Philipp Lauten, Jena University Hospital, Erlanger Allee 101, 07749 Jena, Germany. Email: philipp.lauten@me.com









