

Intracardiac Echocardiography (ICE)-Guided Biopsy of a Right Atrial Mass
ABSTRACT: Although performing a biopsy of the right ventricular septum is a routine procedure in many cardiac catheterization laboratories, the ability to direct a bioptome to a mass within the right or left side of the heart is extremely difficult with fluoroscopic or echocardiographic guidance. The first intracardiac echo (ICE) was performed in the early 1970s. Since that time, the use of ICE in the cardiac catheterization laboratory has aided in transseptal puncture, ablation of cardiac arrhythmias, mitral valvuloplasty, and the closure of atrial septal defects and patent foramen ovale. This case report describes the use of ICE to facilitate intracardiac biopsy of a right atrial mass.
J INVASIVE CARDIOL 2011;23:E99–E101
Key words: biopsy, intracardiac echo, intracardiac mass,
superior vena cava compression
_______________________________________
Although biopsy of the right ventricular septum is a routine procedure in many cardiac catheterization laboratories, the ability to direct a bioptome to a mass within the right or left side of the heart is extremely difficult with fluoroscopic or echocardiographic guidance.  The first intracardiac echocardiogram (ICE) was performed in the early 1970s.1 Since that time, the use of ICE in the cardiac catheterization laboratory has aided in transseptal puncture, ablation of cardiac arrhythmias, mitral valvuloplasty, and the closure of atrial septal defects and patent foramen ovale.2–5 This case report describes the use of ICE to facilitate intracardiac biopsy of a right atrial mass.
The first intracardiac echocardiogram (ICE) was performed in the early 1970s.1 Since that time, the use of ICE in the cardiac catheterization laboratory has aided in transseptal puncture, ablation of cardiac arrhythmias, mitral valvuloplasty, and the closure of atrial septal defects and patent foramen ovale.2–5 This case report describes the use of ICE to facilitate intracardiac biopsy of a right atrial mass.
Case Report. A 70-year-old male with a complex past medical history, including  transient ischemic attacks, sick sinus syndrome with pacemaker placement, bilateral renal transplants secondary to glomerulonephritis and bovine aortic valve replacement, initially presented with acute onset of facial swelling. Imaging from an outside facility demonstrated superior vena cava compression from the left subclavian vein, which was thought to be related to occlusive thrombus on his pacemaker wires. He was placed on anticoagulation, instructed to sleep at a
transient ischemic attacks, sick sinus syndrome with pacemaker placement, bilateral renal transplants secondary to glomerulonephritis and bovine aortic valve replacement, initially presented with acute onset of facial swelling. Imaging from an outside facility demonstrated superior vena cava compression from the left subclavian vein, which was thought to be related to occlusive thrombus on his pacemaker wires. He was placed on anticoagulation, instructed to sleep at a  45° angle and brought to the catheterization lab, where balloon angioplasty of the left subclavian and innominate veins was performed, despite not finding a significant stenosis in this area. It was thought that the anticoagulation had resulted in resolution of clot burden prior to the procedure. The patient was seen in follow-up two weeks later with return of his facial swelling while sleeping flat. This usually resolved during the course of the day with normal activities. He was continued on anticoagulation and followed clinically. He presented one month later with sweats, abdominal pain and flu-like symptoms. Further imaging revealed a large right atrial mass with hypermetabolic activity on positron emission tomography scan (Figures 1A, 1B and 2). The patient was referred to cardiac catheterization for a tissue diagnosis.
45° angle and brought to the catheterization lab, where balloon angioplasty of the left subclavian and innominate veins was performed, despite not finding a significant stenosis in this area. It was thought that the anticoagulation had resulted in resolution of clot burden prior to the procedure. The patient was seen in follow-up two weeks later with return of his facial swelling while sleeping flat. This usually resolved during the course of the day with normal activities. He was continued on anticoagulation and followed clinically. He presented one month later with sweats, abdominal pain and flu-like symptoms. Further imaging revealed a large right atrial mass with hypermetabolic activity on positron emission tomography scan (Figures 1A, 1B and 2). The patient was referred to cardiac catheterization for a tissue diagnosis.
Two 8 French (Fr) sheaths (Cordis Corporation, Warren, New Jersey) were  placed in the right femoral vein. A right atrial angiogram was performed with a 6 Fr pigtail catheter (Cordis Corporation) (Figure 3). An 8 Fr Acuson AcuNav intracardiac echo probe (Siemens Medical USA, Malvern, Pennsylvania) was inserted into the right atrium. This was used to visualize the mass (Figure 4). A Mullins sheath (Medtronic, Inc., Minneapolis, Minnesota) was used to guide biopsy forceps (Argon Medical, Athens, Texas) to obtain specimens from the right atrial mass (Figure 5).
placed in the right femoral vein. A right atrial angiogram was performed with a 6 Fr pigtail catheter (Cordis Corporation) (Figure 3). An 8 Fr Acuson AcuNav intracardiac echo probe (Siemens Medical USA, Malvern, Pennsylvania) was inserted into the right atrium. This was used to visualize the mass (Figure 4). A Mullins sheath (Medtronic, Inc., Minneapolis, Minnesota) was used to guide biopsy forceps (Argon Medical, Athens, Texas) to obtain specimens from the right atrial mass (Figure 5).
Pathology results were consistent with post-transplant lymphoproliferative 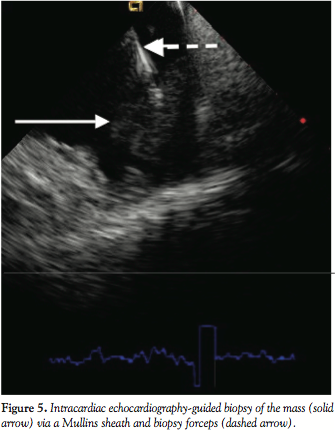 disease. With initiation of chemotherapy, the patient developed tumor lysis syndrome associated with disseminated intravascular coagulopathy, renal failure and profound acidosis with hyperkalemia despite the use of hemodialysis. He quickly succumbed to this disease.
disease. With initiation of chemotherapy, the patient developed tumor lysis syndrome associated with disseminated intravascular coagulopathy, renal failure and profound acidosis with hyperkalemia despite the use of hemodialysis. He quickly succumbed to this disease.
Discussion. There are previous reports in the literature of using ICE to guide intracardiac biopsy procedures. One report utilized the right femoral vein for the ICE catheter and the right subclavian vein for specimen harvesting.6 Another report used a fixed needle system via the right internal jugular and right femoral veins.7 The approach chosen in our case was the most familiar and least complex via the right femoral vein. The Mullins sheath provided directional control and delivery of the biopsy forceps from this access point. The ICE catheter ensured the proper location of the sheath/forceps system in relation to the mass. In previous cases, there has been difficulty using fluoroscopy or even transesophageal echo guidance to direct a bioptome inside the cardiac chambers to retrieve catheter pieces or to obtain a biopsy specimen. With the use of ICE, the probe can be placed next to the tissue and visualize the tip of the bioptome as it touches the echogenic structure to be biopsied. To accomplish this, it is necessary to initially image the mass with the ICE catheter close to the mass. Then using fluoroscopy, bring the bioptome up to the ICE catheter tip. The bioptome tip can then be seen on the ICE image as it touches and moves the mass.
There are many benefits to ICE guidance in the cardiac catheterization laboratory. In addition to the proceduralist being able to control the imaging field, ICE results in greater patient comfort versus transesophageal echocardiography. ICE is routinely used for transseptal punctures, ablation of cardiac arrhythmias and structural heart disease cases. This case report describes an additional use of ICE to facilitate a successful biopsy of a right atrial mass via the femoral vein approach.
References
- Bom N, Lancee CT, Van Egmond FC. An ultrasonic intracardiac scanner. Ultrasonics 1972;10:72–76.
- Mitchel JF, Gillam LD, Sanzobrino BW, et al. Intracardiac ultrasound imaging during transseptal catheterization. Chest 1995;108:104–108.
- Mangrum JM, Mounsey JP, Kok LC, et al. Intracardiac echocardiography-guided, anatomically based radiofrequency ablation of focal atrial fibrillation originating from pulmonary veins. J Am Coll Cardiol 2002;39:1964–1972.
- Hung JS, Fu M, Yeh KH, et al. Usefulness of intracardiac echocardiography in complex transseptal catheterization during percutaneous transvenous mitral commissurotomy. Mayo Clin Proc 1996;71:134–140.
- Hijazi Z, Wang Z, Cao Q, et al. Transcatheter closure of atrial septal defects and patent foramen ovale under intracardiac echocardiographic guidance: Feasibility and comparison with transesophageal echocardiography. Catheter Cardiovasc Interv 2001;52:194–199.
- Mitchell AR, Timperley J, Hudsmith L, et al. Eur J Echocardiogr 2007;8:505–506.
- Sze DY, Lee DP, Hofmann LV, Petersen B. Biopsy of cardiac masses using a stabilized intracardiac echocardiography-guided system. J Vasc Interv Radiol 2008;19:1662–1667.
____________________________
From *Advanced Cardiovascular Consultants, Inc., Rock Island, Illinois and §the University of California, David Geffen School of Medicine, Department of Medicine, Division of Cardiology, Los Angeles, California.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted July 28, 2010 and accepted September 15, 2010.
Address for correspondence: Paul Poommipanit, MD, Advanced Cardiovascular Consultants, Inc., 2525 24th Street, Rock Island, IL 61201. Email: ppoommipanitmd@gmail.com









