

Intrapericardial Synthetic Glue Injection — A Last Resort Effort to Salvage Recurrent Cardiac Tamponade Secondary to Coronary Microleak Post PCI
ABSTRACT: We report a case of cardiac tamponade caused by a coronary microleak from an unapparent site that was successfully managed by sealing of the pericardial space with intrapericardial injection of sterile synthetic glue which, to the best of our knowledge, is the first report of its kind for post-PCI coronary leaks.
J INVASIVE CARDIOL 2011;23(12):E293-E295
______________________________________
Post-angioplasty cardiac tamponade is an important cause of in-hospital morbidity and mortality.1 Coronary artery perforations occur secondary to use of debulking devices, or more commonly, due to oversized balloon/stent dilatations and sometimes wire-tip microperforations.2,3 Cardiac tamponade, though itself usually apparent intraprocedure, may sometimes become evident only a few hours after the procedure, with or without an apparent leaking site from the coronary vasculature. Immediate pericardiocentesis is life-saving, but most cases require definitive management with active fixation of the cause and reversal of anticoagulation as well. Some of the active measures used include prolonged balloon inflation, implantation of covered stents, coil embolization, intra-arterial glue injection, or even emergent coronary artery bypass surgery.4-10
We report a case of recurrent cardiac tamponade caused by a coronary microleak from an unapparent site that was successfully managed by sealing of the pericardial space with intrapericardial injection of sterile synthetic glue which, to the best of our knowledge, is the first report of its kind.
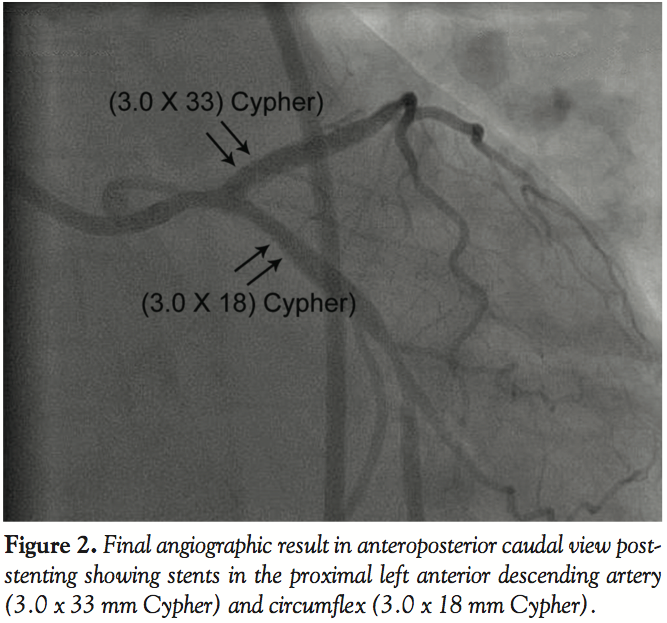
 Case Report. The patient was a 58-year-old postmenopausal hypertensive lady who presented with recent onset unstable angina. Her coronary angiography revealed severe proximal long segment left anterior descending (LAD) artery and severe circumflex (CX) stenosis at ostium with moderate independent stenosis in mid-segment of the CX (50%), while the right coronary artery (RCA) was normal (Figure 1). A successful V-stenting to both the LAD and CX was performed with a 3 x 33 mm Cypher stent in the proximal LAD and a 3 x 18 mm Cypher stent in the proximal left CX beginning from the ostium of both vessels. The moderate mid-CX lesion was electively not addressed. The postprocedure result was reasonable, with the left main segment looking anatomically small but without any evidence of dissection or microleak, which was accepted (Figure 2). High-pressure postdilatation was specifically not attempted, lest matters got complicated, especially at the left main bifurcation.
Case Report. The patient was a 58-year-old postmenopausal hypertensive lady who presented with recent onset unstable angina. Her coronary angiography revealed severe proximal long segment left anterior descending (LAD) artery and severe circumflex (CX) stenosis at ostium with moderate independent stenosis in mid-segment of the CX (50%), while the right coronary artery (RCA) was normal (Figure 1). A successful V-stenting to both the LAD and CX was performed with a 3 x 33 mm Cypher stent in the proximal LAD and a 3 x 18 mm Cypher stent in the proximal left CX beginning from the ostium of both vessels. The moderate mid-CX lesion was electively not addressed. The postprocedure result was reasonable, with the left main segment looking anatomically small but without any evidence of dissection or microleak, which was accepted (Figure 2). High-pressure postdilatation was specifically not attempted, lest matters got complicated, especially at the left main bifurcation.
 Six hours later, the patient developed severe hypotension and a bedside echocardiogram revealed a moderate pericardial effusion with cardiac tamponade. Immediate pericardiocentesis was done and 150 mL of blood aspirated through the subxiphoid approach; a pigtail catheter was left in situ. The residual heparin effect was reversed by protamine. The patient was monitored in the ward with serial echocardiography. She remained stable for the next 8 hours or so, when she again developed hypotension, and the echocardiogram again showed cardiac tamponade. About 100 mL of blood was again aspirated from the in situ pigtail and auto transfused. Two hours later, there was again clinical tamponade with re-accumulation of pericardial fluid, which was re-aspirated; at this point, the patient was moved to the cath lab so we could attempt to locate the leaking site and attempt to actively fix the problem.
Six hours later, the patient developed severe hypotension and a bedside echocardiogram revealed a moderate pericardial effusion with cardiac tamponade. Immediate pericardiocentesis was done and 150 mL of blood aspirated through the subxiphoid approach; a pigtail catheter was left in situ. The residual heparin effect was reversed by protamine. The patient was monitored in the ward with serial echocardiography. She remained stable for the next 8 hours or so, when she again developed hypotension, and the echocardiogram again showed cardiac tamponade. About 100 mL of blood was again aspirated from the in situ pigtail and auto transfused. Two hours later, there was again clinical tamponade with re-accumulation of pericardial fluid, which was re-aspirated; at this point, the patient was moved to the cath lab so we could attempt to locate the leaking site and attempt to actively fix the problem.
 The check angiography, however, did not reveal any obvious leaking site (Figure 3). The stented site, if it was the source of the leak, could not be fixed by a specific intervention like a covered stent or coil embolization because the site involved the left main bifurcation and the ostia of two major vessels, i.e., the LAD and CX. However, since the patient was certainly having recurrent tamponade which definitely needed management, as a last resort, it was decided to inject intrapericardial sterile glue and try to seal the pericardial space itself.
The check angiography, however, did not reveal any obvious leaking site (Figure 3). The stented site, if it was the source of the leak, could not be fixed by a specific intervention like a covered stent or coil embolization because the site involved the left main bifurcation and the ostia of two major vessels, i.e., the LAD and CX. However, since the patient was certainly having recurrent tamponade which definitely needed management, as a last resort, it was decided to inject intrapericardial sterile glue and try to seal the pericardial space itself.
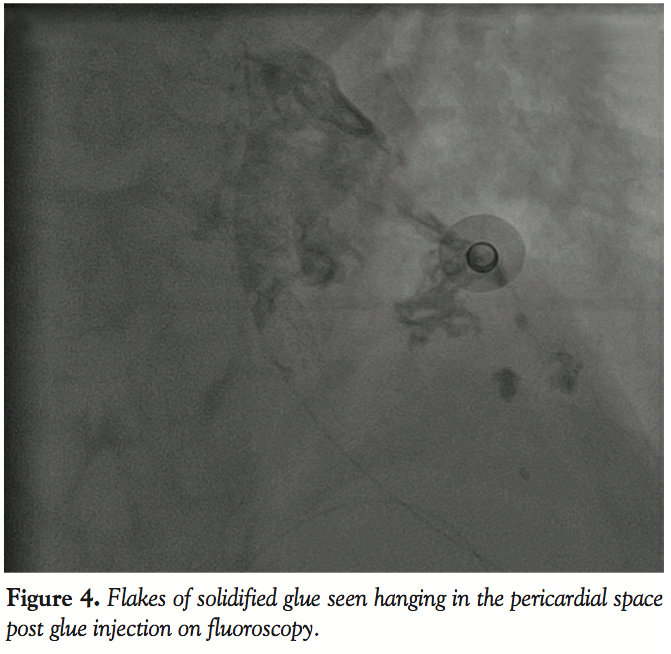 We first ensured that maximum possible blood had been drained out of the pericardial space (through the in situ catheter) so that the two layers of the pericardium were as close together as possible. The pigtail catheter was then exchanged for an infant feeding tube passed in through the 7 Fr vascular sheath in place. Injection of sterile glue was then made through the infant feeding tube into the pericardial space. Each injection contained 0.3 mL of sterile synthetic glue (Histoacryl, Braun Inc.) diluted with 0.3 mL Lipiodol solution with a prior dextrose flush of the system so as to prevent setting of the glue anywhere in transit (Figure 4). A total of 5 such injections were performed. Following this, the patient stabilized and hemodynamics improved rapidly. Over the next 24 hours, serial echocardiography revealed no re-accumulation of pericardial fluid. The intrapericardial sheath was removed 24 hours later and the patient was closely monitored for the next 48 hours and subsequently discharged in a stable condition.
We first ensured that maximum possible blood had been drained out of the pericardial space (through the in situ catheter) so that the two layers of the pericardium were as close together as possible. The pigtail catheter was then exchanged for an infant feeding tube passed in through the 7 Fr vascular sheath in place. Injection of sterile glue was then made through the infant feeding tube into the pericardial space. Each injection contained 0.3 mL of sterile synthetic glue (Histoacryl, Braun Inc.) diluted with 0.3 mL Lipiodol solution with a prior dextrose flush of the system so as to prevent setting of the glue anywhere in transit (Figure 4). A total of 5 such injections were performed. Following this, the patient stabilized and hemodynamics improved rapidly. Over the next 24 hours, serial echocardiography revealed no re-accumulation of pericardial fluid. The intrapericardial sheath was removed 24 hours later and the patient was closely monitored for the next 48 hours and subsequently discharged in a stable condition.
At 9-month follow-up exam, the patient was asymptomatic and echocardiographic examination revealed normal biventricular function without any evidence of constriction.
Discussion. Iatrogenic pericardial effusion has been reported with almost all cardiac percutaneous diagnostic or interventional procedures.1 Most instances of pericardial effusion and cardiac tamponade after percutaneous coronary interventions are due to coronary arterial perforations secondary to a wire-tip microperforation or oversized balloon/stent dilatations, and sometimes use of different kinds of atherectomy devices in heavily calcific or tortuous vessels. The management of such patients is usually tailored to the severity of the clinical situation and though pericardiocentesis can be life-saving in such instances, often patients require definitive interventions to seal off the leak, including prolonged balloon inflations, implantation of covered stents, coil embolization, or even emergent coronary artery bypass surgery.2,3 However, recurrent pericardial tamponade, especially in the absence of an apparent leaking site, poses a difficult therapeutic challenge to the interventional cardiologist.
Sterile glue is available for medical use either as pure synthetic glue (Histoacryl), or as dual component fibrin glue (fibrin plus thrombin) and has long been used as an embolic agent. Though it has been used mainly for neurointerventional indications,4 anecdotal use for closure of esophageal varices,5 femoral pseudoaneurysms,6 septal ablation in HOCM,7 distal coronary artery microperforations,8,9 and intrapericardial injection in a few cases of acute myocardial infarction with cardiac rupture10 have been reported.
In our patient, because the stented site included the ostia of both the LAD and left CX, and there was no obvious angiographic leak, the use of covered stents or coil embolization was precluded. We then resorted to intrapericardial glue injection as a last resort with a view to seal the two layers of the pericardium, which would possibly contain any fresh leak by obliterating the space between the two pericardial layers as a result of glue adhesions within the space. Since the synthetic glue Histoacryl sets as soon as it comes in contact with sodium ions in tissue fluid, it was essential to pre-flush the entire system with dextrose solution while injecting into the pericardial space. Glue should be injected rapidly so that it does not come in contact with blood anywhere in transit, else it would set on the way itself. Mixing with Lipiodol helps keep track of the glue passage into the target site, since the glue particles themselves are otherwise radiolucent.
To minimize the length of the delivery system and for optimum instillation of the glue within the pericardium, we used 12-inch long infant feeding tubes through which the injections were made and the tubes were replaced after every injection. Earlier reports of intrapericardial glue injection after myocardial infarction cardiac tamponade have used fibrin glue that does not require a sodium-free environment in the injection catheter. We used the synthetic glue Histoacryl, as that was the only one available on the shelf at the time, but possibly either could have been used, and work as well.
As coronary interventions become progressively more complex and aggressive, interventional cardiologists need to be aware of such novel therapeutic options. It needs to be stressed that such a strategy may only be used as a last resort in cases of recurrent iatrogenic tamponade in a situation with no other options. It could perhaps also be considered for selected patients with recurrent malignant pericardial effusions who are high surgical risk for creation of a pericardial window.
Although our patient is doing well at 9 months without any clinical or echocardiographic evidence of constriction, longer follow-up and more reports are needed to claim this as a routine therapeutic strategy.
We do understand a limitation in our documentation because of the nonavailability of the echocardiographic pictures pre- and post-glue injection showing the glue adhesions within the pericardial space. This was primarily because of the urgency of the clinical situation and our prime attention then being toward patient salvage so that attempts to record the image were overlooked.
References
- Holmes DR Jr, Nishimura R, Fountain R, Turi ZG. Iatrogenic pericardial effusion and tamponade in the percutaneous intracardiac intervention era. JACC Cardiovasc Interv. 2009;2(8):705-717.
- Javaid A, Buch AN, Satler LF, et al. Management and outcomes of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2006;98(7):911-914.
- Shirakabe A, Takano H, Nakamura S, et al. Coronary perforation during percutaneous coronary intervention. Int Heart J. 2007;48(1):1-9.
- Pollak JS, White RI Jr. The use of cyanoacrylate adhesives in peripheral embolisation. J Vasc Interv Radiol. 2001;12(8):907-913.
- Konate A, Oberti F, Aube C, et al. Stomal varices treated by glue embolization. Gastroenterol Clin Biol. 2007;31(3):300-302.
- Goel PK, Modi N, Baijal SS, Kathuria M, Agrawal SK. Sonographically guided thrombin injection for the treatment of femoral artery pseudoaneurysm. Indian Heart J. 2003;55(4):365-367.
- Oto A, Aytemir K, Deniz A. New approach to septal ablation: glue (cyanoacrylate) septal ablation. Catheter Cardivasc Interv. 2007;69(7):1021-1025.
- Stroger H, Ruef J. Closure of guidewire-induced coronary artery perforation with two component fibrin glue. Catheter Cardiovasc Interv. 2007;70(2):237-240.
- Goel PK. Delayed and repeated cardiac tamponade following microleak in RCA successfully treated with intra-arterial sterile glue injection. Catheter Cardiovasc Interv. 2009;73(6):797-800.
- Terashima M, Fujiwara S, Yaginuma GY, Takizawa K, Kaneko U, Meguro T. Outcome of percutaneous intrapericardial fibrin-glue injection therapy for left ventricular free wall rupture secondary to acute myocardial infarction. Am J Cardiol. 2008;101(4):419-421.
______________________________________
From the Department of Cardiology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 12, 2011, provisional acceptance given May 19, 2011, final version accepted August 10, 2011.
Address for correspondence: Pravin K. Goel, MD, DM, FACC, Professor & Head of Cardiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, 226014, India. Email: pkgoel@sgpgi.ac.in











