

Irrigated Radiofrequency Ablation Catheter and Electro-Anatomical Mapping With Computerized Tomography Integration for Renal Artery Sympathetic Denervation
ABSTRACT: Despite over 6 decades of progress in the development of pharmacological therapy for hypertension, severe drug-resistant hypertension remains a major problem. Endovascular radiofrequency ablation of the proximal renal arteries has been reported to decrease renal artery sympathetic activity and improve long-term hypertensive control. Existing “approved” catheters for this procedure are solid tip, non-irrigated, and often difficult to steer. The existing technique uses angiography and lends itself to increased risk of renal scarring and possible stenosis. We describe a patient with multi-drug resistant hypertension who underwent catheter ablation of the bilateral renal arteries, using for the first time, an open irrigated cardiac ablation catheter with both electro-anatomical guidance and computerized tomography anatomical integration. We used “off-label” irrigated catheters, which are less prone to overheating and char formation at the catheter-surface interface, thereby decreasing the possibility of distal embolization to the renal parenchyma. The integration of electro-anatomical mapping into this procedure allowed us to avoid inadvertent circumferential ablation of the artery using electro-anatomical mapping may lower the risk of subsequent renal artery stenosis.
J INVASIVE CARDIOL 2012;24(12):E308-E310
Key words: endovascular radiofrequency ablation
_____________________________________________
Hypertension is a global healthcare problem affecting over 1 billion people. Despite over 6 decades of progress in the development of pharmacological therapy for hypertension, severe drug-resistant hypertension remains a major and growing problem.1 Endovascular radiofrequency ablation of the proximal renal arteries has been reported to decrease renal artery sympathetic activity, decrease renal vein catecholamine levels, and improve long-term hypertensive control.2,3 To date, this procedure has been primarily performed with specially designed solid-tip fixed curved catheters using angiographic guidance. Solid-tip catheters have significant disadvantages compared to existing irrigated-tip catheters widely utilized for catheter ablation of cardiac arrhythmias. In this case report, we describe a patient with multi-drug resistant hypertension who underwent catheter ablation of the bilateral renal arteries using an open irrigated cardiac ablation catheter incorporating both electro-anatomical guidance and computerized tomography (CT) anatomical integration.
 Case Report. A 74-year-old male with a 30-year history of refractory hypertension was referred to our clinic for assessment. Causes for secondary hypertension had previously been excluded and at time of assessment the patient was being treated with eight anti-hypertensive medications at optimal doses. Despite these therapies, resting systolic blood pressures in this patient typically exceeded 180 mm Hg. The patient had a normal creatinine clearance and renal artery spiral CT angiogram was performed in anticipation of electro-anatomical CT integration. An 8 Fr hemostatic sheath was inserted into the right femoral artery. The previously obtained renal CTA scan images were segmented on the CARTO 3 cardiac catheter ablation system (Biosense Webster, Inc). The patient was heparinized to achieve an activated clotting time of >300 seconds. An SL-2 guiding sheath (St. Jude Medical, Inc) was
Case Report. A 74-year-old male with a 30-year history of refractory hypertension was referred to our clinic for assessment. Causes for secondary hypertension had previously been excluded and at time of assessment the patient was being treated with eight anti-hypertensive medications at optimal doses. Despite these therapies, resting systolic blood pressures in this patient typically exceeded 180 mm Hg. The patient had a normal creatinine clearance and renal artery spiral CT angiogram was performed in anticipation of electro-anatomical CT integration. An 8 Fr hemostatic sheath was inserted into the right femoral artery. The previously obtained renal CTA scan images were segmented on the CARTO 3 cardiac catheter ablation system (Biosense Webster, Inc). The patient was heparinized to achieve an activated clotting time of >300 seconds. An SL-2 guiding sheath (St. Jude Medical, Inc) was 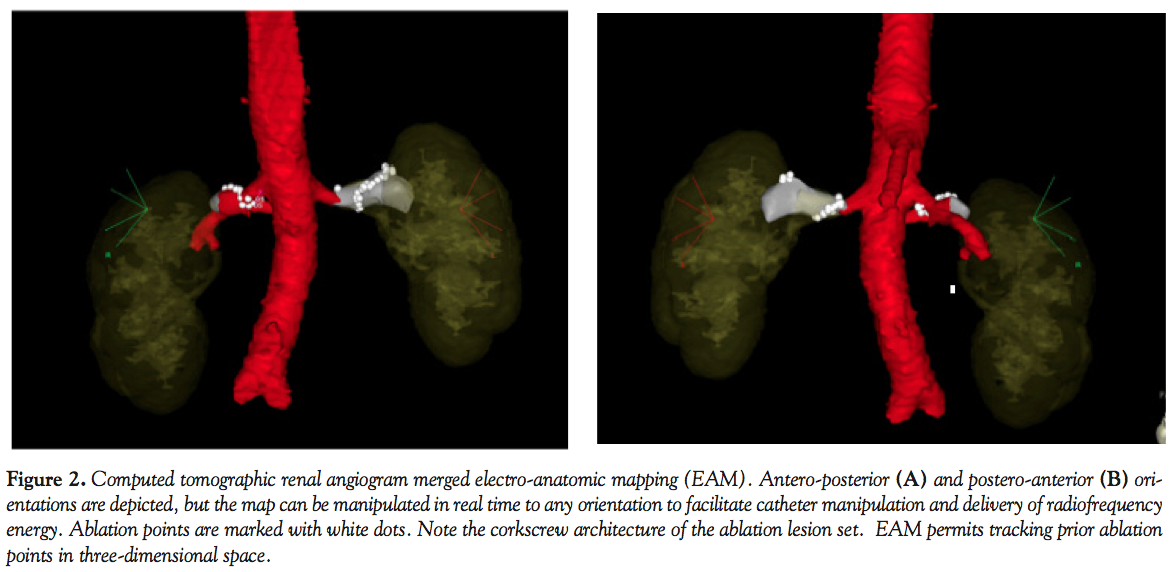 inserted into the descending aorta and pre-ablation bilateral renal artery angiograms were performed (Figure 1). This sheath was continuously irrigated during the procedure with heparinized saline solution. A 3.5 mm tip Navistar thermocool B-curve ablation catheter (Biosense Webster, Inc) was inserted via the guiding sheath and positioned at both renal artery ostia. The proximal renal artery take-off point from the aorta was electro-anatomically tagged for both renal arteries at its inferior portion. These tags were used for image registration and the previously obtained renal artery CTA was registered with the CARTO 3 mapping system. High-output burst pacing of 20 mA at rates up to 9 msec was then applied to various portions of the renal artery under electro-anatomical guidance. No significant change in central arterial pressures or the heart rate was seen during these pacing maneuvers.
inserted into the descending aorta and pre-ablation bilateral renal artery angiograms were performed (Figure 1). This sheath was continuously irrigated during the procedure with heparinized saline solution. A 3.5 mm tip Navistar thermocool B-curve ablation catheter (Biosense Webster, Inc) was inserted via the guiding sheath and positioned at both renal artery ostia. The proximal renal artery take-off point from the aorta was electro-anatomically tagged for both renal arteries at its inferior portion. These tags were used for image registration and the previously obtained renal artery CTA was registered with the CARTO 3 mapping system. High-output burst pacing of 20 mA at rates up to 9 msec was then applied to various portions of the renal artery under electro-anatomical guidance. No significant change in central arterial pressures or the heart rate was seen during these pacing maneuvers.
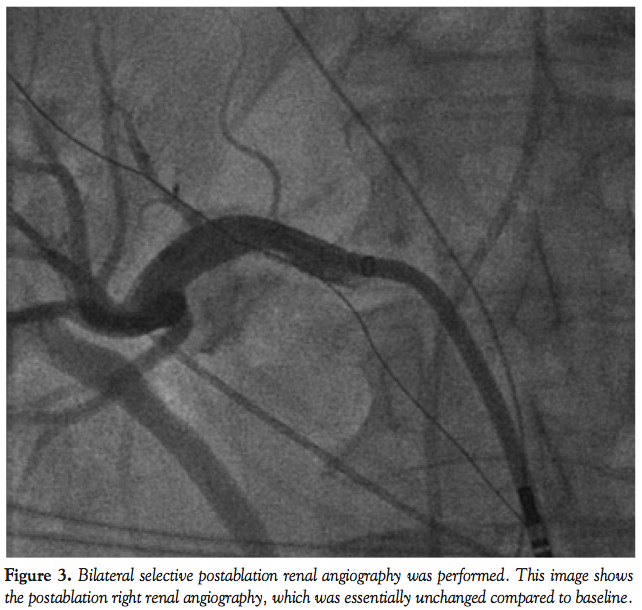 The open irrigation system was set to continuously irrigate the ablation catheter at 2 cc/min during catheter manipulation and at 17 cc/min during radiofrequency delivery. The ablation catheter was inserted into the distal right renal artery just proximal to the primary arterial branch point. Ablation was started at this point. Care was utilized during ablation to avoid the adrenal branch of the renal artery. Radiofrequency energy (10 watts) was delivered for 10 seconds at each ablation point. Ablation lesions were tagged with the electro-anatomical mapping system. The ablation lesion set was delivered in a corkscrew type manner as previously described,2-4 starting distally and ending proximally in the artery. The corkscrew architecture versus a circumferential architecture was utilized in an attempt to avoid potential renal artery stenosis from occurring as a result of the ablation procedure. During ablation delivery, no changes to either the centrally monitored blood pressure or heart rate were seen. The same procedure was then performed on the left renal artery. The catheter was navigated during this procedure utilizing electro-anatomic and fluoroscopic guidance. All ablations were recorded on the integrated merged CTA map (Figure 2). Postablation renal angiograms were essentially unchanged from the preablation angiogram (Figure 3). There were no procedural complications.
The open irrigation system was set to continuously irrigate the ablation catheter at 2 cc/min during catheter manipulation and at 17 cc/min during radiofrequency delivery. The ablation catheter was inserted into the distal right renal artery just proximal to the primary arterial branch point. Ablation was started at this point. Care was utilized during ablation to avoid the adrenal branch of the renal artery. Radiofrequency energy (10 watts) was delivered for 10 seconds at each ablation point. Ablation lesions were tagged with the electro-anatomical mapping system. The ablation lesion set was delivered in a corkscrew type manner as previously described,2-4 starting distally and ending proximally in the artery. The corkscrew architecture versus a circumferential architecture was utilized in an attempt to avoid potential renal artery stenosis from occurring as a result of the ablation procedure. During ablation delivery, no changes to either the centrally monitored blood pressure or heart rate were seen. The same procedure was then performed on the left renal artery. The catheter was navigated during this procedure utilizing electro-anatomic and fluoroscopic guidance. All ablations were recorded on the integrated merged CTA map (Figure 2). Postablation renal angiograms were essentially unchanged from the preablation angiogram (Figure 3). There were no procedural complications.
During the 24 hours of postablation observation, the patient was seen to have a marked improvement in blood pressure control with normalization of systolic blood pressure on postablation day 1 and no deterioration in renal function. When seen at follow-up 1 and 4 months postablation, the patient’s blood pressure remained optimally controlled, with systolic blood pressures averaging less than 130 mm Hg, and he was on only 7 oral medications with significantly reduced doses.
Discussion. The Symplicity Catheter System (Medtronic-Ardian) is the only investigational radiofrequency ablation system currently available for use in the renal arteries and uses a solid-tip catheter.2 In this case report, we report using existing catheter ablation equipment to perform a renal sympathetic denervation procedure. Although our procedure entails an “off-label” use of a combination of existing approved products, there are a number of reasons why this approach might prove superior to existing current-generation investigational renal sympathetic denervation radiofrequency ablation tools. Compared to solid-tip ablation catheters, irrigated catheters are less prone to overheating and char formation at the catheter-surface interface, thereby decreasing the possibility of distal embolization to the renal parenchyma. In addition, open irrigated catheters allow greater energy delivery to subendothelial structures.
The integration of electro-anatomical mapping into this procedure is a unique application of existing technologies. With this technique, the operator can track where ablation lesions have been delivered in a three-dimensional manner to prevent repeat ablations at the same location and also to prevent circumferential ablation in the artery. The ability to avoid inadvertent circumferential ablation of the artery using electro-anatomical mapping may lower the risk for subsequent renal artery stenosis. Moreover, electro-anatomic mapping may ultimately decrease the amount of contrast medium used during the procedure. Unlike existing proprietary renal artery sympathetic ablation catheters, the catheters used in this case report are steerable. The catheters and equipment used for this case report are currently widely available and many of these technologies can be utilized for renal artery sympathetic denervation procedures.
References
- Daugherty SL, Powers JD, Magid DJ, et al. Incidence and prognosis of resistant hypertension in hypertensive patients. Circulation. 2012;125(13):1635-1642.
- Symplicity HTN-1 Investigators. Catheter-based renal sympathetic denervation for resistant hypertension: durability of blood pressure reduction out to 24 months. Hypertension. 2011;57(5):911-917.
- Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, Böhm M; Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hypertension (the symplicity HTN-2 trial): A randomised controlled trial. Lancet. 2010;376(9756):1903-1909.
- Ahmed H, Neuzil P, Skoda J, et al. Renal sympathetic denervation using an irrigated radiofrequency ablation catheter for the management of drug-resistant hypertension. JACC Cardiovasc Interv. 2012;5(7):758-765.
_____________________________________
From the 1Department of Internal Medicine, University of Miami Miller School of Medicine Regional Campus, JFK Medical Center, Atlantis, Florida and 2Florida Electrophysiology Associates, Atlantis, Florida.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Fishel is a consultant for Biosense Webster. The other authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 18, 2012, provisional acceptance given November 6, 2012, final version accepted November 8, 2012.
Address for correspondence: Sachil Shah, MD, University of Miami Miller School of Medicine Regional Campus, JFK Medical Center, Department of Internal Medicine, 5301 S. Congress Ave, Atlantis, FL 33462. Email: sshah7@med.miami.edu










