

Late Cardiac Perforation Following Percutaneous Atrial Septal Defect Closure Using the Solysafe Device
ABSTRACT: Percutaneous atrial septal defect closure has been demonstrated to be a safe and effective procedure. Many different devices have been utilized during the last decade with a low complication rate. We report a patient who presented with cardiac tamponade 6 months after ASD closure using the Solysafe device. Emergency surgery demonstrated a disarticulated device as well as a broken wire migrated into the pericardial space causing cardiac perforation and tamponade. To the best of our knowledge, this is the first report of late cardiac perforation following ASD closure using the Solysafe device.
J INVASIVE CARDIOL 2011;23:E139–E141
_______________________________________
Percutaneous closure of ostium-secundum type atrial septal defect (ASD) has become a safe and effective alternative to surgical repair during the last decade.1,2 Procedural complications are rare; nevertheless, erosion/cardiac perforation are well recognized and poorly understood.3,4 Several devices are utilized in contemporary clinical practice, and the Solysafe device (Swissimplant AG, Solothurn, Switzerland) is one of the newest.
We report a patient who presented with hemodynamic instability secondary to large hemopericardium and cardiac perforation that occurred 6 months after Solysafe device implantation for ASD closure. During emergency surgery, the device was resected, a broken wire from the device was rescued and the defect was patch-closed. Indications, advantages and a hypothetical explanation regarding the complication encountered with this device are presented.
Case Report. A 54-year-old female weighing 58 kg underwent uneventful ASD closure using a Solysafe device. The defect showed adequate rims (slightly attenuated anterosuperior or aortic rim) measuring 20 mm by transesophageal echocardiography (TEE) and 24 mm after balloon sizing. A type 30 device was utilized, placed through a 14 French (Fr) short introducer. The patient recovered well and remained with an immediate small anterosuperior shunt measuring 2.5 mm in diameter.
The patient was asymptomatic at follow-up. Two Doppler echocardiograms were performed at 1 and 3 months post-device implantation reporting a persistent 2.5 mm small anterosuperior shunt.
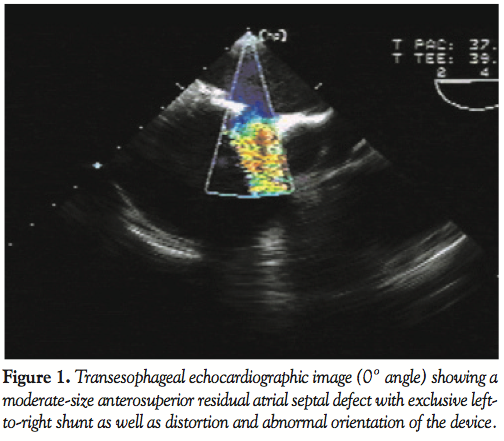 During her 6-month post-implantation visit, the patient complained of shortness of breath and easy fatigue since 20 days earlier. During physical examination, muffled heart sounds and hypotension were detected. A CXR showed large cardiomegaly and an electrocardiogram revealed right atrial enlargement and incomplete right bundle branch block. A Doppler echocardiogram showed a large circumferential pericardial effusion. A TEE was performed and a larger shunt measuring 8 mm in diameter at the anterosuperior rim was discovered with distortion of the device with
During her 6-month post-implantation visit, the patient complained of shortness of breath and easy fatigue since 20 days earlier. During physical examination, muffled heart sounds and hypotension were detected. A CXR showed large cardiomegaly and an electrocardiogram revealed right atrial enlargement and incomplete right bundle branch block. A Doppler echocardiogram showed a large circumferential pericardial effusion. A TEE was performed and a larger shunt measuring 8 mm in diameter at the anterosuperior rim was discovered with distortion of the device with 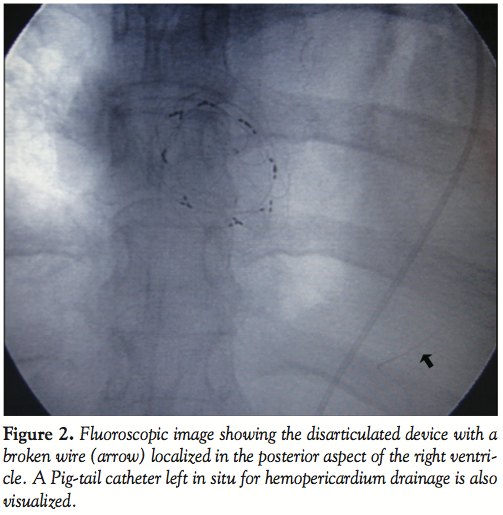 abnormal orientation of some wires (Figure 1). Fluoroscopy was performed in different angles and compared with the initial images obtained the day of implantation. This comparative study showed a disarticulated device with a portion of a wire fractured, separated from the device and migrated inferiorly. It was unclear if this wire was located either in the right ventricle (RV) or in the pericardial space (Figure 2).
abnormal orientation of some wires (Figure 1). Fluoroscopy was performed in different angles and compared with the initial images obtained the day of implantation. This comparative study showed a disarticulated device with a portion of a wire fractured, separated from the device and migrated inferiorly. It was unclear if this wire was located either in the right ventricle (RV) or in the pericardial space (Figure 2).
The patient was admitted to the Intensive Care Unit and a pericardiocentesis 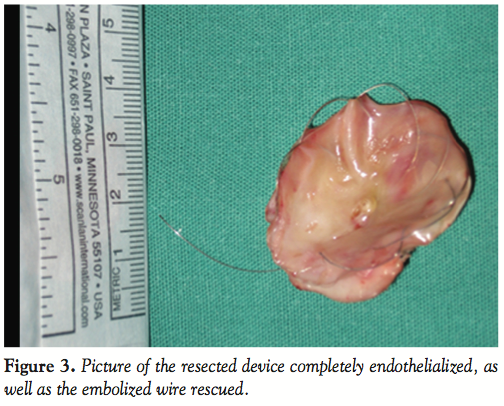 was performed, obtaining 450 cc of fresh blood. A Pig-tail catheter was left in situ. An emergency surgery was carried out with confirmation of the findings: the portion of broken wire was rescued from the posterior aspect of the RV in the pericardial space. The device was resected (Figure 3) and a pericardial patch was sutured, closing the defect. It was not possible to localize the perforation site, although there was a localized atrial wall hematoma involving the dome of the right atrium. The patient recovered successfully and was discharged after 5 days in hospital. At 6- and 12-month follow-up, she was well and has returned to normal activities.
was performed, obtaining 450 cc of fresh blood. A Pig-tail catheter was left in situ. An emergency surgery was carried out with confirmation of the findings: the portion of broken wire was rescued from the posterior aspect of the RV in the pericardial space. The device was resected (Figure 3) and a pericardial patch was sutured, closing the defect. It was not possible to localize the perforation site, although there was a localized atrial wall hematoma involving the dome of the right atrium. The patient recovered successfully and was discharged after 5 days in hospital. At 6- and 12-month follow-up, she was well and has returned to normal activities.
Discussion. Device implantation is the preferred treatment modality for closure of ostium-secundum type ASD with adequate anatomy in children as well as in adults. It has been proven to be safe and effective in terms of closure success rate, morbidity, hospital length of stay and earlier hemodynamic improvement compared to surgical closure.1,2
Many different ASD devices have been utilized during the last decade, with a low rate of early and late complications.5 Erosion/perforation, embolization, arrhythmias and nickel allergy have been described.
The Solysafe septal occluder is a self-centering device with two foldable polyester patches attached to eight metal wires made of phynox (a cobalt-based alloy). Two wire holders keep the wires fixed at the proximal (right atrium) and distal (left atrium) ends of the device. As the wire holders are brought together, the device configures into a very flat, flower-like shape. Devices with patch diameters of 15, 20, 25, 30 and 35 mm are available. It is recommended to use the device in children > 10 kg due to the smallest size of the introducer sheath (10 Fr) required. Due to its self-centering capabilities, it is possible to close ASD up to 30 mm in diameter. In general, the nominal diameter of the device should exceed the defect diameter by at least 3 mm. Oversizing is relatively forgiving and does not result in excessive bulging.
The reported experience with the use of this device for ASD closure is reduced to two small studies with 15 and 32 patients. Closure rate was 100% at 6-month follow-up in both studies,6,7 showing no early or late complications. One advantage reported is its explicit self-centering capabilities, with the possibility of adaptation to different defect sizes, leading to the necessity of stocking fewer occluder sizes to close a broad spectrum of defects. Another unique characteristic is the folding mechanism, which is able to configure either the left or right atrial component while avoiding the prolapse of the left disc in larger defects. Moreover, the device does not require the use of a large sheath for deployment, so the incidence of air embolism is thought to be decreased.
Device fracture has been described for several occluders, including the CardioSEAL/STARFlex family of devices, Helex and Cardia.8–11 To date, no device fracture has been reported with the use of the Solysafe occluder. We speculate that in this patient, one of the wires completely disarticulated and broke from the central connecting part of the device and perforated the dome of the right atrium (the site where the surgeon found a hematoma), migrating into the pericardial space and landing in the posterior aspect of the RV. This complication led to a complete rearrangement of the remaining device, with the appearance of a larger residual shunt. Viewing a chest x-ray initially performed in the patient, it was difficult to completely visualize the device, and we failed to detect the broken wire. Fluoroscopy was very useful in detecting the problem. Whether the cause of this complication was a manufacturer defect or fatigue fracture must be elucidated. Due to the subacute clinical presentation in this case, we believe it is necessary to emphasize the importance of teaching the patients receiving new cardiac devices about signs and symptoms of potential complications related to the implanted device, such as the cardiac tamponade in this case. They should be warned to seek medical advice immediately if any sign or symptom arises.
Our case demonstrated that fracture/disarticulation remains a potential complication and can occur with the new Solysafe device. The importance of close follow-up of new implanted devices and the role of late fluoroscopy to re-check the position/configuration of this type of occluders are highlighted.
Conclusion. This report shows a severe late complication following an ostium-secundum type ASD closure using a Solysafe device. Occluder fracture and fragmentation are shown. Surgical resolution is presented. Close follow-up of newly developed devices is recommended.
References
- Du ZD, Hijazi ZM, Kleinman CS, et al. Comparison between transcatheter and surgical closure of secundum atrial defect in children and adults: Results of a multicenter nonrandomized trial. J Am Coll Cardiol 2002;39:1833–1846.
- Butera G, Carminati M, Chessa M, et al. Percutaneous versus surgical closure of secundum atrial defect: Comparison of early results and complications. Am Heart J 2006;151:228–234.
- Amin Z, Hijazi ZM, Bass JL, et al. Erosion of Amplatzer septal occluder device after closure of secundumatrial defects: Review of registry of complications and recommendations to minimize future risk. Catheter Cardiovasc Interv 2004;63:496–502.
- Divecar A, Gaamangwe T, Shaikh N, et al. Cardiac perforation after device closure of atrial septal defects with the Amplatzer septal occluder. J Am Coll Cardiol 2005;45:1213–1218.
- Chessa M, Carminati M, Butera G, et al. Early and late complications associated with transcatheter occlusion of secundum atrial defect. J Am Coll Cardiol 2002;39:1061–1065.
- Ewert P, Söderberg B, Dähnert I, et al. ASD and PFO closure with the Solysafe septal occluder — Results of a prospective multicenter pilot study. Catheter Cardiovasc Interv 2008;71:398–402.
- Kretschmar O, Sglimbea A, Daehnert I, et al. Interventional closure of atrial septal defects with the Solysafe Septal Occluder — Preliminary results in children. Int J Cardiol 2009;13:13.
- Fagan T, Dreher D, Cutright W, et al. GORE HELEX Septal Occluder Working Group. Fracture of the GORE HELEX septal occluder: Associated factors and clinical outcomes. Catheter Cardiovasc Interv 2009;73:941–948.
- Scott PA, Wilson N, Veldtman GR. Fracture of a GORE HELEX septal occluder following PFO closure in a diver. Catheter Cardiovasc Interv 2009;73:828–831.
- Marinakis A, Lampropoulos K, Iliopoulos T. Fractura del oclusor implantado en una comunicación interauricular como causa de taponamiento cardiaco. Rev Esp Cardiol 2010;63:346.
- Narayan V, Puri P, Mehra AO. Late presentation of CardioSEAL PFO closure device fracture and thrombus formation three years after device implantation. J Invasive Cardiol 2008;20:247–249.
_________________________________________
From 1the Adult Congenital Heart Disease Program, Division of Cardiology, San Roque Hospital, 2the Division of Cardiology, and 3the Section of Pediatric Cardiology, Private Hospital of Córdoba, Córdoba, Argentina.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 3, 2010, provisional acceptance given October 12, 2010, final version accepted October 27, 2010.
Address for correspondence: Alejandro Peirone, MD, FSCAI, Belgrano 2771 (5016) Córdoba, Argentina. Email: alepeirone@yahoo.com











