

Learning Curve in Transradial Cardiac Catheterization: Procedure-Related Parameters Stratified by Operators’ Transradial Volume
Abstract: Objectives. To determine whether radial artery access is associated with a reduction in fluoroscopy time, procedure time, and other procedural variables over a 27-month period during which the radial artery approach was incorporated in a single academic Medical Center. Background. Although previous studies have demonstrated a relationship between increased volume and decreased procedural time, no studies have looked at the integration of radial access over time. Methods. Data were collected from consecutive patients who presented to the Vanderbilt University Medical Center cardiac catheterization laboratory from January 1, 2009 to April 1, 2011. Patients who underwent radial access diagnostic catheterization with and without percutaneous coronary intervention were included in this study. A total of 1112 diagnostic cardiac catheterizations through the radial access site were analyzed. High-volume, intermediate-volume, and low-volume operators were grouped based on the percentage of procedures performed through a radial approach. Results. From 2009 to 2011, there was a significant decrease in fluoroscopy time in all operator groups for diagnostic catheterization (P=.035). The high-volume operator group had 1.88 and 3.66 minute reductions in fluoroscopy time compared to the intermediate- and low-volume operator groups, respectively (both P<.001). Likewise, the intermediate-volume operator group had a 1.77 minute improvement compared to the low-volume operator group, but this did not reach statistical significance (P=.102). The improvement in fluoroscopy time and other procedure-related parameters was seen after approximately 25 cases with further improvement after 75 cases. Conclusions. The incorporation of the radial access approach in the cardiac catheterization laboratory led to a decrease in fluoroscopy time for each operator and operator group over the last 3 years. Our data demonstrated that higher-volume radial operators have better procedure, room, and fluoroscopy times when compared to intermediate- and low-volume operators. However, lower-volume operators have a reduction in procedure-related parameters with increased radial cases. Number of procedures needed to become sufficient was demonstrated in the current study.
J INVASIVE CARDIOL 2012;24(11):599-604
Key words: radial access technique
_________________________________________________________
Although cardiac catheterization through radial access has been extensively used in Europe and Asia for the past two decades, it remains common practice in the United States to utilize a femoral artery approach. In fact, the National Cardiovascular Data Registry (606 US sites; 2004 to 2007) showed that the radial approach was used in only 4.5% of cardiac catheterizations and less than 2% of percutaneous coronary interventions (PCI).1 Studies have shown multiple benefits of utilizing the radial approach in cardiac catheterization. Radial access reduced major bleeding by 73% compared to femoral access.2 Radial access has been shown to be feasible and safe in patients who are fully anticoagulated,3 in non-ST elevation myocardial infarction,4 and in the setting of acute ST-elevation myocardial infarction without cardiogenic shock.5
Prior studies have evaluated the effect of radial access on radiation exposure.6 Mercuri et al have observed that radial access is associated with an increased exposure to radiation compared to femoral access, although they didn’t compare operators based on experience. In a 1996 paper, Spaulding et al evaluated left radial approach variables including procedure duration, procedure failure, and sheath insertion.7 They showed mean procedure duration of 19.1 ± 8.2 minutes, procedure failure rate of 9%, and mean time for sheath insertion of 4.7 ± 4.7 minutes. No studies have looked at how operator experience affects these variables or how these variables improve over time.
The recent RIVAL study8 looked at patients with ACS undergoing PCI through a radial versus femoral approach. In addition to finding no significant difference among the patient groups in mortality rate, number of major bleeding events, or number of coronary events, there was a statistically significant reduction in mortality for high-risk patients with acute coronary syndromes who underwent angiography via the radial approach. In medical centers that perform the most radial procedures, angiography patients had a much lower risk of death, myocardial infarction, or stroke (1.3% in the highest tertile compared to 4.9 and 2.8% in the intermediate and lower tertiles, respectively; interaction P=.013).
Vanderbilt Heart and Vascular Institute is a tertiary care referral center. The cardiac catheterization laboratory is a high-volume center with 14 interventional cardiologists. All operators perform at least 250 diagnostic cases per year and have experience in both the radial and femoral approaches. Radial access was rarely performed at our institution prior to 2007 (less than 1%, institutional data). In the period from 2007 to 2008, the radial artery was introduced as a routine point of access, and was more widely adopted as a method of access starting in 2009. Due to this change, we evaluated the effects on procedure-related parameters: fluoroscopy time, procedure time, room time, volume of contrast used, and number of catheters used per case. Furthermore, we sought to study the change in these parameters based on operator volume of the radial access site (high, intermediate, and low).
Methods
 All patients who presented to our cardiac catheterization laboratory from January 1, 2009 to April 1, 2011 were included in this study. Patients were included if they underwent a diagnostic cardiac catheterization with the primary purpose of investigation for coronary artery disease. Patients were excluded if they were: (1) referred for an emergency PCI (eg, primary or rescue PCI for ST-segment elevation myocardial infarction); (2) simultaneous right heart catheterization and/or biopsies; (3) elective PCI with or without diagnostic catheterization; (4) underwent peripheral angiography and/or intervention); (5) underwent additional diagnostics with an intravascular ultrasound and/or pressure wire during the diagnostic catheterization procedure; (6) had a procedure that required crossover to femoral or brachial artery access; (7) renal dysfunction (defined as having a creatinine >1.80 mg/dL) and/or were on dialysis at the time of referral to the catheterization laboratory. Each patient had baseline characteristics collected: age, gender, height and weight, BMI, and history of prior coronary artery bypass grafting. Procedural variables were collected including procedure time (defined as time when the operator begins to obtain access to when access sheath is removed), room time (defined as the time the patient entered the room to the time he/she exited the room), fluoroscopy time (time in minutes that fluoroscopy was utilized), amount of contrast (in milliliters), and the number of catheters used.
All patients who presented to our cardiac catheterization laboratory from January 1, 2009 to April 1, 2011 were included in this study. Patients were included if they underwent a diagnostic cardiac catheterization with the primary purpose of investigation for coronary artery disease. Patients were excluded if they were: (1) referred for an emergency PCI (eg, primary or rescue PCI for ST-segment elevation myocardial infarction); (2) simultaneous right heart catheterization and/or biopsies; (3) elective PCI with or without diagnostic catheterization; (4) underwent peripheral angiography and/or intervention); (5) underwent additional diagnostics with an intravascular ultrasound and/or pressure wire during the diagnostic catheterization procedure; (6) had a procedure that required crossover to femoral or brachial artery access; (7) renal dysfunction (defined as having a creatinine >1.80 mg/dL) and/or were on dialysis at the time of referral to the catheterization laboratory. Each patient had baseline characteristics collected: age, gender, height and weight, BMI, and history of prior coronary artery bypass grafting. Procedural variables were collected including procedure time (defined as time when the operator begins to obtain access to when access sheath is removed), room time (defined as the time the patient entered the room to the time he/she exited the room), fluoroscopy time (time in minutes that fluoroscopy was utilized), amount of contrast (in milliliters), and the number of catheters used.
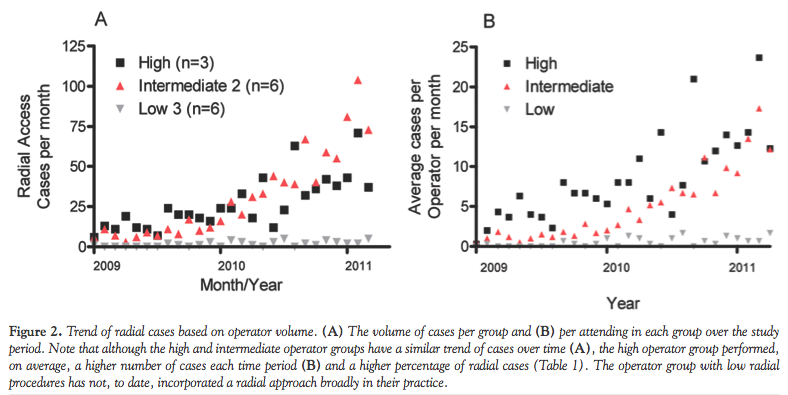 The operators were then subgrouped into tertiles based on the percentage of radial access for each operator. Group 1 was those operators performing more than 30% of their cases through a radial approach (over the last year) and Group 2 was those operators performing between 10%-30%, and Group 3 was those performing less than 10%. This is detailed in Figure 2 and Table 1.
The operators were then subgrouped into tertiles based on the percentage of radial access for each operator. Group 1 was those operators performing more than 30% of their cases through a radial approach (over the last year) and Group 2 was those operators performing between 10%-30%, and Group 3 was those performing less than 10%. This is detailed in Figure 2 and Table 1.
Statistical analysis. All data are expressed as median and inter-quartile range (25%-75%) in the tables and median ± 95% confidence interval (CI) in the figures for continuous variables, frequency (%) for categorical variable and median ± 95% 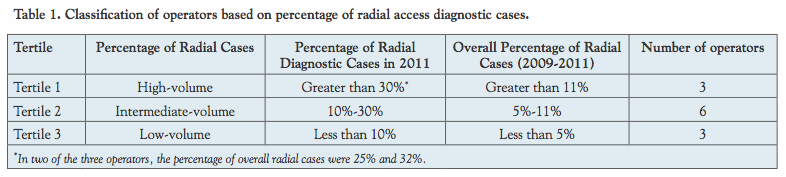 confidence interval in the figures, unless otherwise stated. Analysis among groups was done using the global test for overall comparison of group means in ANOVA and the non-parametric Kruskal-Wallis one-way ANOVA. All subgroups were defined a priori. Statistical significance was defined as a two sided P<.05. Statistical analysis was done using SPSS version 18 (Release 18.0.2, April 2010).
confidence interval in the figures, unless otherwise stated. Analysis among groups was done using the global test for overall comparison of group means in ANOVA and the non-parametric Kruskal-Wallis one-way ANOVA. All subgroups were defined a priori. Statistical significance was defined as a two sided P<.05. Statistical analysis was done using SPSS version 18 (Release 18.0.2, April 2010).
Results
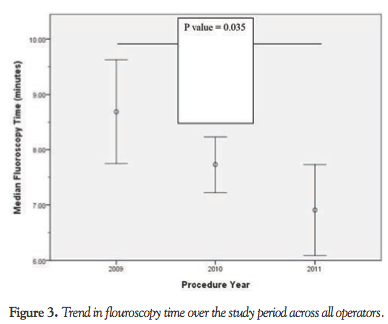
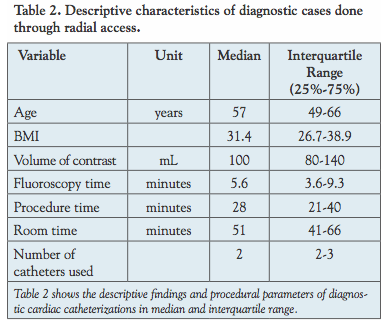 From 1/1/2009 to 4/1/2011, a total of 1112 patients underwent diagnostic cardiac catheterization using a radial approach. Table 2 shows baseline characteristics of these patients. Initially, we analyzed the overall fluoroscopy time in all operators over the study period (Figure 3). This figure shows an improvement starting in 2009 and continuing into 2011. There is a trend toward improvement between 2009 to 2011, and the difference between 2009 and 2011 is statistically signifcant (P=.035). The procedure time and room time did not change significantly.
From 1/1/2009 to 4/1/2011, a total of 1112 patients underwent diagnostic cardiac catheterization using a radial approach. Table 2 shows baseline characteristics of these patients. Initially, we analyzed the overall fluoroscopy time in all operators over the study period (Figure 3). This figure shows an improvement starting in 2009 and continuing into 2011. There is a trend toward improvement between 2009 to 2011, and the difference between 2009 and 2011 is statistically signifcant (P=.035). The procedure time and room time did not change significantly.
 Fluoroscopy time, procedure time, and room time were analyzed by subgroup based on utilization of the radial access site. This is shown in Figure 4. Here, there is a reduction in fluoroscopy time in all three groups of operators over the study period. This improvement in these procedure-related parameters happens after 25 cases and then plateaus until 75 cases. There is further improvement after 75 cases are done (Figure 5).
Fluoroscopy time, procedure time, and room time were analyzed by subgroup based on utilization of the radial access site. This is shown in Figure 4. Here, there is a reduction in fluoroscopy time in all three groups of operators over the study period. This improvement in these procedure-related parameters happens after 25 cases and then plateaus until 75 cases. There is further improvement after 75 cases are done (Figure 5).
 By the global test for means ANOVA between high, intermediate, and low groups, there was a statistically significant difference between the groups in terms of fluoroscopy time. The high operator group had a 1.88 and 3.66 minute reduction in fluoroscopy time compared to the intermediate and low operator groups, respectively (both P<.001). Likewise, the intermediate-volume operator group had a 1.77 minute improvement compared to the low-volume operator group, but this did not reach statistical significance (P=.102). Procedure time and room time showed a similar trend with fluoroscopy time (Table 4).
By the global test for means ANOVA between high, intermediate, and low groups, there was a statistically significant difference between the groups in terms of fluoroscopy time. The high operator group had a 1.88 and 3.66 minute reduction in fluoroscopy time compared to the intermediate and low operator groups, respectively (both P<.001). Likewise, the intermediate-volume operator group had a 1.77 minute improvement compared to the low-volume operator group, but this did not reach statistical significance (P=.102). Procedure time and room time showed a similar trend with fluoroscopy time (Table 4).
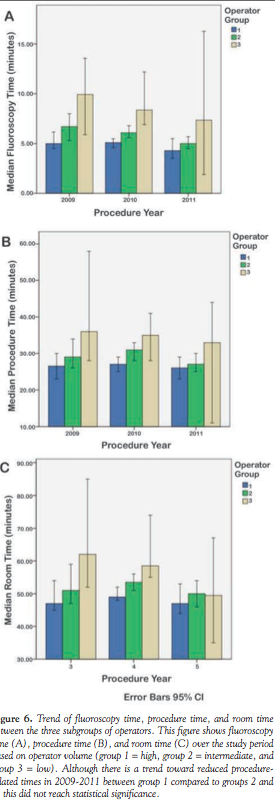
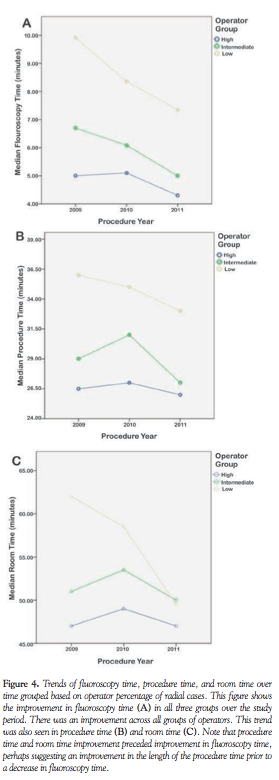 Figure 6 further details this trend by year and operator group. Although there was a trend toward lower fluoroscopy, procedure, and room times between each subgroup (high, intermediate and low operator subgroups), this was not statistically significant.
Figure 6 further details this trend by year and operator group. Although there was a trend toward lower fluoroscopy, procedure, and room times between each subgroup (high, intermediate and low operator subgroups), this was not statistically significant.
In addition, the high operator group used 0.448 catheters less than the low operator group (P=.034). Also, contrast volume per case was not different between the different subgroups (data not shown).
Discussion
 During the more than 2-year period during which radial access was used more commonly in our catheterization laboratory, flouroscopy, procedure, and room times were all reduced. There was a non-significant reduction in fluoroscopy times from 2009 to 2010, and the difference between 2009 and 2011 was statistically signifcant (P=.035). This is notable because a reduction in fluoroscopy time can decrease radiation exposure to the operator and staff (which can be substantial over a career spanning decades) as well as to patients, many of whom receive multiple procedures. This reduction in fluoroscopy time was also seen in procedure time and room time. This is also of potential clinical importance, since over the course of a career, this can reduce the cumulative dose of radiation exposure to operators.
During the more than 2-year period during which radial access was used more commonly in our catheterization laboratory, flouroscopy, procedure, and room times were all reduced. There was a non-significant reduction in fluoroscopy times from 2009 to 2010, and the difference between 2009 and 2011 was statistically signifcant (P=.035). This is notable because a reduction in fluoroscopy time can decrease radiation exposure to the operator and staff (which can be substantial over a career spanning decades) as well as to patients, many of whom receive multiple procedures. This reduction in fluoroscopy time was also seen in procedure time and room time. This is also of potential clinical importance, since over the course of a career, this can reduce the cumulative dose of radiation exposure to operators.
 Increased fluoroscopy time is associated with increased radiation exposure. We have been able to decrease fluoroscopy time in each operator (and therefore institute-wide) over the last 3 years. Although radial access has recently been shown to be associated with increased patient9 and operator exposure10 to radiation, our study shows that with increased experience with this approach, radiation exposure can be reduced in all operators. Our findings support the notion that more consistent utilization of transradial access results in the greater improvements in fluoroscopy time and other procedure-related variables. Similar to our findings, the RIVAL study also showed that radial access had better outcomes than femoral access at institutions that performed a high volume of radial procedures, with no such benefit in middle or low tertiles (interaction P=.021).
Increased fluoroscopy time is associated with increased radiation exposure. We have been able to decrease fluoroscopy time in each operator (and therefore institute-wide) over the last 3 years. Although radial access has recently been shown to be associated with increased patient9 and operator exposure10 to radiation, our study shows that with increased experience with this approach, radiation exposure can be reduced in all operators. Our findings support the notion that more consistent utilization of transradial access results in the greater improvements in fluoroscopy time and other procedure-related variables. Similar to our findings, the RIVAL study also showed that radial access had better outcomes than femoral access at institutions that performed a high volume of radial procedures, with no such benefit in middle or low tertiles (interaction P=.021).
 Our data show an improvement in procedure-related parameters that begins after 25 cases, leveling off after that, then again improving after 75 cases. This is in keeping with the learning curve for radial access suggested by others.1,7 To our knowledge, this is the first study to demonstrate potential competency parameters. These results may help to form training and credentialing criteria in cardiac catheterization laboratories.
Our data show an improvement in procedure-related parameters that begins after 25 cases, leveling off after that, then again improving after 75 cases. This is in keeping with the learning curve for radial access suggested by others.1,7 To our knowledge, this is the first study to demonstrate potential competency parameters. These results may help to form training and credentialing criteria in cardiac catheterization laboratories.
With the overall adjustments in procedural reimbursements, the need to continue to cut costs with comparable delivery of quality health care is needed. Radial approach PCI with same-day discharge after a 6-hour observation period has been shown to be safe in nearly 2200 patients studied by Small et al11 and 800 patients studied by Heyde et al.12 This trend persisted even in high-risk lesions (ACC type B2 and C).
Overall, our objective in expanding the use of radial approach in our institution has been successful. This was encouraged by studies that showed a better morbidity and patient satisfaction in this patient population. In addition, other factors, such as promotion by the high-volume operators, cardiac catheterization lab director, and nationwide increase in utilization of radial access are factors that would further advance broader use of radial access cardiac catheterization.
Study limitations. There are several limitations to our data and conclusions. Operators, regardless of their experience, are different in how much fluoroscopy they utilize. This is the case regardless of access site preference. Operators that use high amounts of fluoroscopy might do so regardless of whether they are well versed in a particular procedure (or utilizing a new access site) or not, and vice versa. This is also the case for procedure time and room time. In addition, there are many other variables that would affect procedure time and room time.
Another limitation is that prior experience with radial access in our operators was not accounted for, and assumed no prior experience. Nonetheless, this was very limited (see Figure 1). Furthermore, trainee (general cardiology or interventional cardiology fellows) involvement in the procedure was not accounted for, and we assumed that their distribution among operators was equal. Our sample size was medium. The nature of the study did not allow for randomization. Also, we could not compare right radial to left radial approach because of the very small number of diagnostic catheterizations performed from a left radial approach. The recent PREVAIL study was a prospective, multicenter, observational survey of 1052 consecutive patients and concluded that the left radial route was associated with shorter procedure times and lower radiologic exposure than the right radial approach, independently of an operator’s proficiency.13 This is logical because the left radial route is more similar to a femoral route when transitioning from a femoral to radial approach, but might be a limitation in obese patients with larger abdominal girth.
Conclusions
Incorporation of radial access to our cardiac catheterization laboratory led to a decrease in fluoroscopy time in each operator, operator group, and institute-wide over the last 3 years. This improvement was seen after approximately 25 cases and further improved after 75 cases.
References
- Rao SV, Ou FS, Wang TY, et al. Trends in the prevalence and outcomes of radial and femoral approaches to percutaneous coronary intervention: a report from the National Cardiovascular Data Registry. JACC Cardiovasc Interv. 2008;1(4):379-386.
- Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(11):1409-1420.
- Ziakas AG, Koskinas KC, Gavrilidis S, et al. Radial versus femoral access for orally anticoagulated patients. Catheter Cardiovasc Interv. 2010;76(4):493-499.
- Cayla G, Silvain J, Barthelemy O, et al. Trans-radial approach for catheterisation in non-ST segment elevation acute coronary syndrome: an analysis of major bleeding complications in the ABOARD Study. Heart. 2011;97(11):887-891.
- Hetherington SL, Adam Z, Morley R, et al. Primary percutaneous coronary intervention for acute ST-segment elevation myocardial infarction: changing patterns of vascular access, radial versus femoral artery. Heart. 2009;95(19):1612-1618.
- Mercuri M, Mehta S, Xie C, Valettas N, Velianou JL, Natarajan MK. Radial artery access as a predictor of increased radiation exposure during a diagnostic cardiac catheterization procedure. JACC Cardiovasc Interv. 2011;4(3):347-352.
- Spaulding C, Lefevre T, Funck F, et al. Left radial approach for coronary angiography: results of a prospective study. Cathet Cardiovasc Diagn. 1996;39(4):365-370.
- Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(9775):1409-420.
- Mercuri M, Mehta S, Xie C, Valettas N, Velianou JL, Natarajan MK. Radial artery access as a predictor of increased radiation exposure during a diagnostic cardiac catheterization procedure. JACC Cardiovasc Interv. 2011;4(3):347-352.
- Lange HW, von Boetticher H. Randomized comparison of operator radiation exposure during coronary angiography and intervention by radial or femoral approach. Catheter Cardiovasc Interv. 2006;67(1):12-16.
- Small A, Klinke P, Della Siega A, et al. Day procedure intervention is safe and complication free in higher risk patients undergoing transradial angioplasty and stenting. The discharge study. Catheter Cardiovasc Interv. 2007;70(7):907-912.
- Heyde GS, Koch KT, de Winter RJ, et al. Randomized trial comparing same-day discharge with overnight hospital stay after percutaneous coronary intervention: results of the Elective PCI in Outpatient Study (EPOS). Circulation. 2007;115(17):2299-2306.
- Pelliccia F, Trani C, Biondi-Zoccai GG, et al. Comparison of the feasibility and effectiveness of transradial coronary angiography via right versus left radial artery approaches (from the PREVAIL study). Am J Cardiol. 2012;110(6):771-775.
__________________________________________________________
From the Vanderbilt University Medical Center, Department of Internal Medicine, Division of Cardiovascular Medicine, Nashville, Tennessee.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 26, 2012, provisional acceptance given May 30, 2012, final version accepted June 12, 2012.
Address for correspondence: Ehab Kasasbeh, MD, 383 PRB Division of Cardiovascular Medicine, 2200 Pierce Avenue, Nashville, TN 37232. Email: ehab.kasasbeh@vanderbilt.edu











