

Left Main Stenting and Landmark Analysis — Drawing the Line
The optimal revascularization strategy for emergent left main coronary artery (LMCA) in the setting of acute coronary syndrome (ACS) remains largely an unresolved issue. The most current ACC/AHA 2009 Focused Update Guidelines assign it a IIb recommendation.1 This carefully adjudicated recommendation stems from the fact that not all LMCA lesions are created equal and outcomes depend among many other considerations on lesion and procedural characteristics, door-to-balloon time, and a myriad of underlying patient comorbidities. In addition, patients with LMCA are frequently not included in contemporary prospective randomized trials, thus depriving us from sorely needed hard outcome data.2
Nonetheless, ST-elevation myocardial infarctions (STEMI) due to LMCA lesions continue to occur and in our daily practice we interventionalists are indeed the “first responders.” The tantalizing question, when faced with a patient with LMCA STEMI, is how best to revascularize these severely and acutely ill patients. The article by Martin-Yuste et al published in this issue of the Journal of Invasive Cardiology provides us with much-needed, state-of-the-art, single-center experience.3
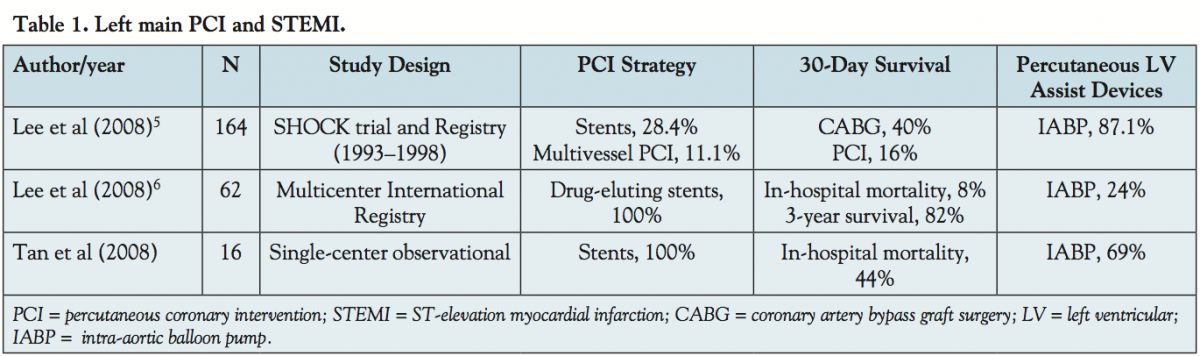 The present dearth of solid evidence makes this report even more relevant. Three representative studies tackling the same topic are summarized in Table 1.4-6 It is immediately obvious that the data we have at present stem from small, highly heterogeneous work. Use of devices, ventricular assist devices, and overall outcome reporting are difficult to compare. Additionally, as frequently seen in interventional cardiology trials, practice patterns change rapidly during times when these studies are performed.
The present dearth of solid evidence makes this report even more relevant. Three representative studies tackling the same topic are summarized in Table 1.4-6 It is immediately obvious that the data we have at present stem from small, highly heterogeneous work. Use of devices, ventricular assist devices, and overall outcome reporting are difficult to compare. Additionally, as frequently seen in interventional cardiology trials, practice patterns change rapidly during times when these studies are performed.
Martin-Yuste et al report on 98 consecutive patients in their institution, of which 41 were treated on an emergent basis. IABP was used in 32% of patients and PCI was successful in 88% of those patients. Drug-eluting stents were used in slightly less than half of the patients. Yet, the most fascinating finding of this study relates to the statistical methods and merits careful review. In-hospital mortality was 24% (n = 10) in the “emergent” compared to 2% (n = 1) for the “elective” LMCA revascularization group (p <0.001). Long-term (mean, 626 days) mortality was 16% (n = 5) in the “emergent” and 11% (n = 6) in the “elective” group (p = 0.52). The authors then performed a landmark analysis using hospital discharge time as “time zero” and found a 17% mortality rate in the “emergent” group (n = 5) and 11% mortality in the “elective” group (n = 6) (p = 0.52) until the end of the observation period.
What does that really mean for clinicians taking care of these patients? It may appear difficult to reconcile those two disparate findings — a marked difference in in-hospital mortality and essentially equal outcomes after discharge.
Landmark analysis has been around for almost 30 years, since its first introduction in 1983 in the Journal of Clinical Oncology.7,8 Simply stated, the landmark analysis “resets the clock” and starts survival analysis at some future time point chosen by the investigators. One of the most recent examples of use of landmark analysis is the TRITON-TIMI 38 trial comparing prasugrel and clopidogrel. Prasugrel reduced events both during the first 3 days and in landmark analysis from 3 days onward to the end of the trial.9
The bias in clinical trials when assessing time-to-event data for various treatment groups exists when, for instance, two groups receive different treatments.
 First and foremost, the patients need to survive from the time of diagnosis to time of treatment. In this study, this applies to patients undergoing emergent PCI for LMCA STEMI — this was not needed for control (elective) patients (Figure 1). Thereafter, treatments available are frequently so different, such as coronary artery bypass grafting (CABG), for which there is inherent delay in performing the procedure due to technical considerations and PCI, which can, by its very nature, be performed more expeditiously. This situation introduces a particular bias, also referred to as “time-to-treatment” bias.
First and foremost, the patients need to survive from the time of diagnosis to time of treatment. In this study, this applies to patients undergoing emergent PCI for LMCA STEMI — this was not needed for control (elective) patients (Figure 1). Thereafter, treatments available are frequently so different, such as coronary artery bypass grafting (CABG), for which there is inherent delay in performing the procedure due to technical considerations and PCI, which can, by its very nature, be performed more expeditiously. This situation introduces a particular bias, also referred to as “time-to-treatment” bias.
The next step where bias occurs is quite difficult to unscramble. The very variables to be included in the emergent LMCA PCI “group” continue to change over time. Namely, the longer a patient survives in the “emergent” group may lead us to conclude that there is a more “favorable” response to treatment in that group, while biasing the “control/elective PCI” group to more “unfavorable” response.8 Numerous unmeasured confounders are present and even the most careful adjustment for baseline characteristics may not be completely helpful.
Does this then mean that the reported landmark analysis is incorrect? It is correct as performed and reported, but needs to be cautiously interpreted. The landmark analysis, by definition, cannot correct for lack of randomization.
This study accurately illustrates limitations of this type of statistical analysis — the arbitrary selection of landmark time and intended omission of events prior to landmark time. The consequence is that landmark analysis may effectively favor generating “data-driven” findings; for instance, no difference is found in survival between the two groups after the arbitrary set landmark time at hospital discharge. Patients who survive to hospital discharge are indeed a sub-selected group with likely overall favorable long-term outcomes.
Since landmark time is arbitrary, one may select an earlier landmark and in so doing include more early events, but then risk misclassifying patients at a longer follow-up. Conversely, if a landmark is set at a later time, a large proportion of early events will be missed with resulting loss of power.
The study by Martin-Juste et al is an observational trial and there was no randomization; it is, however, important to emphasize once again that landmark analyses lack randomization when creating new groups at the landmark time. Therein lies the complexity in drawing conclusions from observational trials with landmark analyses — sorting out the confounding impact of the fundamental factors that lead to “treatment allocation” to “emergent” and “elective” groups may be quite elusive.
And the take-home message? Read the statistics’ fine print — landmark analyses are important tools in our data interpretation toolbox, but they are easily misinterpreted if their limitations are disregarded. This well-conducted study by Martin-Yuste et al further adds to our understanding of how to treat these very ill patients.
References
- Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54(23):2205-2241.
- Patel MR, Smalling RW, Thiele H, et al. Intra-aortic balloon counterpulsation and infarct size in patients with acute anterior myocardial infarction without shock: the CRISP AMI randomized trial. JAMA. 2011 Aug 29 (Epub ahead of print).
- Martin-Yuste V, Alvarez-Contreras L, Brugaletta S. Emergent versus elective percutaneous stent implantation in the unprotected left main: long-term outcomes from a single-center registry. J Invasive Cardiol. 2011;23(10):392-397.
- Tan CH, Hong MK, Lee CW, et al. Percutaneous coronary intervention with stenting of left main coronary artery with drug-eluting stent in the setting of acute ST elevation myocardial infarction. Int J Cardiol. 2008;126(2):224-228.
- Lee MS, Tseng CH, Barker CM, et al. Outcome after surgery and percutaneous intervention for cardiogenic shock and left main disease. Ann Thorac Surg. 2008;86(1):29-34.
- Lee MS, Sillano D, Latib A, et al. Multicenter international registry of unprotected left main coronary artery percutaneous coronary intervention with drug-eluting stents in patients with myocardial infarction. Catheter Cardiovasc Interv. 2009;73(1):15-21.
- Anderson JR, Cain KC, Gelber RD. Analysis of survival by tumor response. J Clin Oncol. 1983;1(11):710-719.
- Dafni U. Landmark analysis at the 25-year landmark point. Circ Cardiovasc Qual Outcomes. 2011;4(3):363-431.
- Antman EM, Wiviott SD, Murphy SA, et al. Early and late benefits of prasugrel in patients with acute coronary syndromes undergoing percutaneous coronary intervention: a TRITON-TIMI 38 (TRial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet InhibitioN with Prasugrel-Thrombolysis In Myocardial Infarction) analysis. J Am Coll Cardiol. 2008;51(21):2028-2033.
____________________________________
From the Division of Cardiology, University of Illinois at Chicago and Jesse Brown VA Medical Center, Chicago, Illinois.
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The author reports no conflicts of interest regarding the content herein.
Address for correspondence: Mladen I. Vidovich, MD, FACC, FSCAI, 840 South Wood Street, MC 715, Chicago, IL 60612. Email: miv@uic.edu










