

Left Main Trunk Perforation Sealed by 90 Second Perfusion Balloon Inflation
ABSTRACT: Coronary perforation is a rare but serious complication of percutaneous coronary intervention. In our case, kissing balloon technique caused the perforation. We took care of balloon diameter and inflation pressure, but we did not consider that the proximal lumen could take elliptical rather than circular shape. Then perforation occurred at the proximal side of the kissing balloon technique. Fortunately, we could achieve hemostasis successfully by 90 seconds perfusion balloon inflation. You must consider not only balloon diameter and inflation pressure but also balloon form as an important safety factor for the kissing balloon technique on the left main trunk.
J INVASIVE CARDIOL 2012;24(6):E115-E118
Key words: percutaneous coronary intervention, kissing balloon technique
_________________________________________
Coronary perforation is a rare but serious complication of percutaneous coronary intervention (PCI) leading to cardiac tamponade or even death.
Coronary perforation occurs in 0.2% to 0.6% of PCI and is usually due to oversized dilatation, balloon rupture, and guidewire injury.1-6 Although surgery is necessary if bleeding from the artery remains uncontrolled, most perforation is successfully managed with prolonged balloon inflation.7,8 However, balloon inflation often takes more than 5-10 minutes to achieve hemostasis, which cannot be tolerated hemodynamically in the proximal coronary segment such as the left main trunk (LMT). In this case report, the perforation was successfully sealed immediately after 90 seconds of perfusion balloon inflation.
 Case Report. A 77-year-old male was admitted for acute interstitial pneumonitis and gastric cancer. The patient developed chest discomfort during the hospital stay. His coronary artery multi-detector computed tomography examination revealed a significant LMT lesion. His echocardiography showed diffuse hypokinesia with depressed systolic function, and ejection fraction was 40%. Following the test, the chest discomfort worsened further and was accompanied by diffuse ST-depression on electrocardiogram. At the same time, the blood pressure fell down from 120 mm Hg to 100 mm Hg. Coronary artery bypass graft was considered, but deferred because the patient was still on high-dose steroids for interstitial pneumonitis and had significant bilateral carotid artery stenosis and gastric cancer. The decision was made to proceed to PCI with bare metal stents. Coronary angiography confirmed the distal LMT trifurcation lesion with heavy calcification (Figure 1A).
Case Report. A 77-year-old male was admitted for acute interstitial pneumonitis and gastric cancer. The patient developed chest discomfort during the hospital stay. His coronary artery multi-detector computed tomography examination revealed a significant LMT lesion. His echocardiography showed diffuse hypokinesia with depressed systolic function, and ejection fraction was 40%. Following the test, the chest discomfort worsened further and was accompanied by diffuse ST-depression on electrocardiogram. At the same time, the blood pressure fell down from 120 mm Hg to 100 mm Hg. Coronary artery bypass graft was considered, but deferred because the patient was still on high-dose steroids for interstitial pneumonitis and had significant bilateral carotid artery stenosis and gastric cancer. The decision was made to proceed to PCI with bare metal stents. Coronary angiography confirmed the distal LMT trifurcation lesion with heavy calcification (Figure 1A).
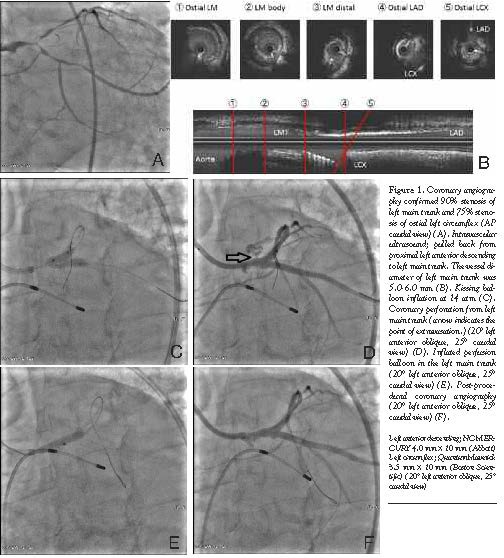
The procedure was performed under intra-aortic balloon pump support. An 8 Fr JL4.0 guiding catheter was engaged, and rotational atherectomy was performed for LMT-left anterior descending (LAD) lesion with a 1.75 mm and a 2.15 mm burr. Then the LMT-left circumflex (LCX) lesion was also treated with a 1.75-mm burr. As he had elective total gastrectomy scheduled for his gastric cancer, we chose bare metal stents and underwent T stenting. From distal to ostial LCX, S-STENT (Biosensors) 3.0 x 18 mm and DRIVER 3.0 x 18 mm (Medtronic Medical) were placed. Intravascular ultrasound (IVUS) showed that the external elastic membrane diameter was 5.0-6.0 mm at the LMT (Figure 1B). Based on the IVUS findings, a S-STENT 3.5 x 14 mm was placed from LMT to LAD at 18 atm. Then, jailed LCX was recrossed and kissing balloon technique (KBT) was utilized with 2 non-compliant balloons [4.0 mm (LAD) and 3.5 mm (LCX)] at 14 atm (Figure 1C). The balloons were inflated for 10 seconds, and blood pressure did not change. After KBT, perforation of LMT was noted (Figure 1D). Sealing of the perforation was attempted immediately with a 4.0 mm balloon, which had been used for KBT. However, blood pressure fell under 80 mm Hg within 30 seconds. Thus, we switched to a perfusion balloon, and due to similar episode of hypotension, the balloon could be inflated for only 90 seconds. Surprisingly, repeat angiogram showed that hemostasis was achieved successfully (Figure 1F). After waiting for a few minutes, no effusion or clinically significant bleeding was noted. The patient was monitored in the coronary care unit for 2 days, and transferred back to pulmonary service uneventfully.
 Discussion. Previous reports have demonstrated that the increase in the risk of perforation is highly associated with the use of oversized balloons,9 stenting against eccentric or tortuous calcified lesions,3,5,9 and the use of atherectomy devices.1,4,6,9,10 In many cases, oversized balloon inflation is the cause of coronary perforation, but in this case, we believe oversized balloon inflation was not the reason of the coronary perforation. Before stent placement on LMT, IVUS presented that external elastic membrane diameter of LMT was 5.0-6.0 mm. Based on the IVUS findings, we chose 3.5 mm and 4.0 mm balloons for KBT. According to the Mitsudo’s formula: R2=D12+D22 (R = theoretical mean hugging balloon diameter in the hugging balloon segment, D1=balloon diameter of main branch, and D2=balloon diameter of side branch) (personal communication, widely used in Japanese clinical practice) (Figure 2),11 the estimated diameter after KBT was 5.3 mm in the LMT. Morino et al stated maximum stent diameter never exceeds the sum of the 2 balloon diameters, but with a more elliptical rather than circular dilation in the proximal segment.11 Although the wall injury by rotablation might have predisposed the perforation, the fact that balloons were inflated elliptically, not circularly, when KBT was performed was thought to be the main cause of the perforation. Extensive tension was probably applied to the uncovered stent area in the LCX ostium, which lead to the complication.
Discussion. Previous reports have demonstrated that the increase in the risk of perforation is highly associated with the use of oversized balloons,9 stenting against eccentric or tortuous calcified lesions,3,5,9 and the use of atherectomy devices.1,4,6,9,10 In many cases, oversized balloon inflation is the cause of coronary perforation, but in this case, we believe oversized balloon inflation was not the reason of the coronary perforation. Before stent placement on LMT, IVUS presented that external elastic membrane diameter of LMT was 5.0-6.0 mm. Based on the IVUS findings, we chose 3.5 mm and 4.0 mm balloons for KBT. According to the Mitsudo’s formula: R2=D12+D22 (R = theoretical mean hugging balloon diameter in the hugging balloon segment, D1=balloon diameter of main branch, and D2=balloon diameter of side branch) (personal communication, widely used in Japanese clinical practice) (Figure 2),11 the estimated diameter after KBT was 5.3 mm in the LMT. Morino et al stated maximum stent diameter never exceeds the sum of the 2 balloon diameters, but with a more elliptical rather than circular dilation in the proximal segment.11 Although the wall injury by rotablation might have predisposed the perforation, the fact that balloons were inflated elliptically, not circularly, when KBT was performed was thought to be the main cause of the perforation. Extensive tension was probably applied to the uncovered stent area in the LCX ostium, which lead to the complication.
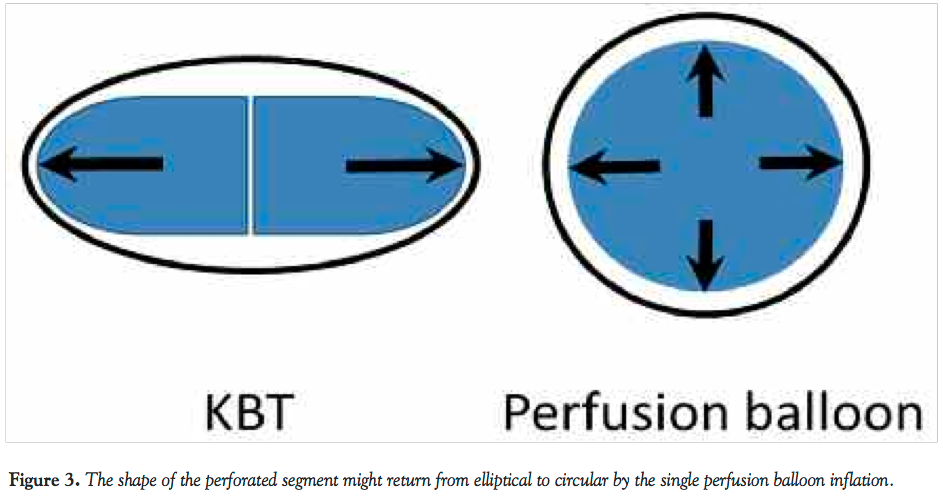 Prolonged (5-15 min) balloon inflation is often needed to seal coronary perforation. In this case, however, hemostasis was achieved in as short as 90 seconds. We thought that there were 2 reasons. First, the high concentrations of elastic fibers in the LMT have been proposed as the possible mechanism of elastic recoil, which might help hemostasis.12 Second, the shape of the perforated segment might return from elliptical to circular by the single perfusion balloon inflation, which was likely to release the tension applied to the area of perforation (Figure 3). Stent graft would have been another effective bailout, but we reserved the choice considering the risk of jailing LCX. At all events, we think that the bailout was a lucky one.
Prolonged (5-15 min) balloon inflation is often needed to seal coronary perforation. In this case, however, hemostasis was achieved in as short as 90 seconds. We thought that there were 2 reasons. First, the high concentrations of elastic fibers in the LMT have been proposed as the possible mechanism of elastic recoil, which might help hemostasis.12 Second, the shape of the perforated segment might return from elliptical to circular by the single perfusion balloon inflation, which was likely to release the tension applied to the area of perforation (Figure 3). Stent graft would have been another effective bailout, but we reserved the choice considering the risk of jailing LCX. At all events, we think that the bailout was a lucky one.
Conclusion
We experienced a case of coronary perforation sealed with a brief 90-second balloon inflation. While applying KBT onto LMT lesion, the size of balloons, application of ideal pressure, and the fact that the proximal lumen can take elliptical, not circular, shape need to be carefully considered.
References
- Ellis SG, Ajluni S, Arnold AZ, et al. Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. Circulation. 1994;90(6):2725-2730.
- Fasseas P, Orford JL, Panetta CJ, et al. Incidence, correlates, management, and clinical outcome of coronary perforation: analysis of 16,298 procedures. Am Heart J. 2004;147(1):140-145.
- Gunning MG, Williams IL, Jewitt DE, Shah AM, Wainwright RJ, Thomas MR. Coronary artery perforation during percutaneous intervention: incidence and outcome. Heart. 2002;88(5):495-498.
- Stankovic G, Orlic D, Corvaja N, et al. Incidence, predictors, in-hospital, and late outcomes of coronary artery perforations. Am J Cardiol. 2004;93(2):213-216.
- Ramana RK, Arab D, Joyal D, et al. Coronary artery perforation during percutaneous coronary intervention: incidence and outcomes in the new interventional era. J Invasive Cardiol. 2005;17(11):603-605.
- Fukutomi T, Suzuki T, Popma JJ, et al. Early and late clinical outcomes following coronary perforation in patients undergoing percutaneous coronary intervention. Circ J. 2002;66(4):349-356.
- Dorros G, Jain A, Kumar K. Management of coronary artery rupture: covered stent or microcoil embolization. Cathet Cardiovasc Diagn. 1995;36(2):148-154.
- Satler LF. Successful nonsurgical treatment of left main stem perforation by sacrifice of the LAD. Catheter Cardiovasc Interv. 2007;69(6):850-851.
- Gruberg L, Pinnow E, Flood R, et al. Incidence, management, and outcome of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2000;86(6):680-682, A8.
- Von Sohsten R, Kopistansky C, Cohen M, Kussmaul WG 3rd. Cardiac tamponade in the "new device" era: evaluation of 6999 consecutive percutaneous coronary interventions. Am Heart J. 2000;140(2):279-283.
- Morino Y, Yamamoto H, Mitsudo K, et al. Functional formula to determine adequate balloon diameter of simultaneous kissing balloon technique for treatment of bifurcated coronary lesions: clinical validation by volumetric intravascular ultrasound analysis. Circ J. 2008;72(6):886-892.
- Villa M, de la Llera LD, Morán JE, Pérez-Cortacero JA, Fournier JA. Coronary perforation during unprotected left main angioplasty. Management with conservative approach: a case report. Int J Cardiol. 2004;97(1):145-146.
_________________________________________
From the Department of Cardiology, Keio University School of Medicine, Tokyo, Japan.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 21, 2011, provisional acceptance given November 22, 2011, final version accepted January 18, 2012.
Address for correspondence: Akio Kawamura, MD, Department of Cardiology, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo 1608582, Japan. Email: kawamura@cpnet.med.keio.ac.jp










