Long-Term Successful Percutaneous Coronary Intervention in Factor VII Deficiency
ABSTRACT: Factor VII deficiency (FVIId) is a congenital coagulation disorder with a wide spectrum of bleeding phenotypes. Percutaneous coronary intervention requires full anticoagulation during stent implantation to avoid acute coronary thrombosis and long-term dual antiplatelet therapy. Feasibility of percutaneous coronary intervention in FVIId is not described in literature. We present a successful case of percutaneous coronary intervention in a 55-year-old male with FVIId, discussing briefly the periprocedural handicaps (anticoagulation regimen and hemostasis at arterial puncture site) as the safety of long-term antiplatelet therapy, and future implications for recombinant FVIId administration in a patient with a previous coronary stent.
J INVASIVE CARDIOL 2012;24(6):E119-E121
________________________________________
Factor VII deficiency (FVIId) is a congenital coagulation disorder presented with an autosomal recessive pattern of inheritance, with an estimated incidence of 1/500,000 people in the general population,1 and a wide spectrum of hemorrhagic phenotypes, ranging from severe life-threatening hemorrhages to miscellaneous minor bleeding or asymptomatic patients.2,3 Its diagnosis is based on an isolated prolongation of the prothrombin time (reduction in prothrombin activity) with a normal activated partial thromboplastin time in a coagulation test, and a FVII coagulant activity (FVIIc) reduction.3
FVIId is associated with an increased perioperative bleeding risk,4 and FVII substitution has proved to be convenient, safe and effective during and after extracorporeal surgery,5-7 but no evidence is described concerning a percutaneous coronary intervention (PCI) and the antithrombotic and antiplatelet regimens required during and after it. Regarding previous literature, we aim to report the first case of a long-term successful PCI in a patient with FVIId.
Case report. A 55-year-old male patient presented with severe obesity (130 kilograms, body mass index: 42), hypertension, hypercholesterolemia, type 2 diabetes mellitus on metformin treatment, and active smoker. Also a heterozygous factor VII deficiency (FVIIc: 40%) had been diagnosed secondary to repeated abnormal coagulation tests, without history of significant bleeding events.
 He was referred for coronarography due to typical effort angina. Prior to the procedure, blood analysis showed normal hemoglobin levels (16.1 gr/dL), platelets recount (291.000/mm3), and normal renal function. Coagulation study revealed a prothrombin activity of 48% (INR: 1.72) with a normal partial thromboplastin time (28 seconds). Coronarography was performed by radial approach to minimize hemorrhagic complications, and 2000 UI of unfractionated heparin were administered as protocolled to avoid radial artery thrombosis. The
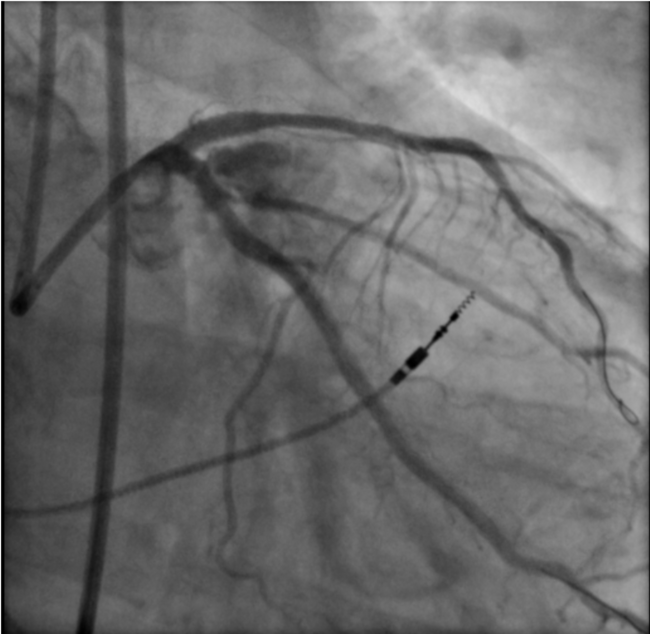
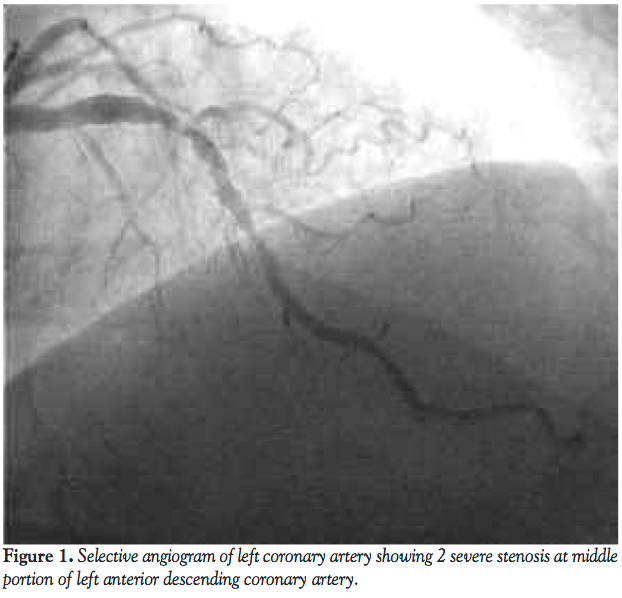
He was referred for coronarography due to typical effort angina. Prior to the procedure, blood analysis showed normal hemoglobin levels (16.1 gr/dL), platelets recount (291.000/mm3), and normal renal function. Coagulation study revealed a prothrombin activity of 48% (INR: 1.72) with a normal partial thromboplastin time (28 seconds). Coronarography was performed by radial approach to minimize hemorrhagic complications, and 2000 UI of unfractionated heparin were administered as protocolled to avoid radial artery thrombosis. The  left anterior descending coronary artery presented 2 severe stenosis at middle portion (Figure 1). The obtuse marginal artery presented a long chronic total occlusion at middle portion (Figure 2) and the right coronary artery showed absence of other significant lesions. Left ventricular systolic function was preserved. According to the hematologist recommendation to diminish the risk of severe bleeding, 1 mg of recombinant activated VII factor (NovoSeven®, Eptacog alfa 50,000 UI) was administered before arterial sheath removal, achieving successful hemostasis after 4 H of radial compressive bandage.
left anterior descending coronary artery presented 2 severe stenosis at middle portion (Figure 1). The obtuse marginal artery presented a long chronic total occlusion at middle portion (Figure 2) and the right coronary artery showed absence of other significant lesions. Left ventricular systolic function was preserved. According to the hematologist recommendation to diminish the risk of severe bleeding, 1 mg of recombinant activated VII factor (NovoSeven®, Eptacog alfa 50,000 UI) was administered before arterial sheath removal, achieving successful hemostasis after 4 H of radial compressive bandage.
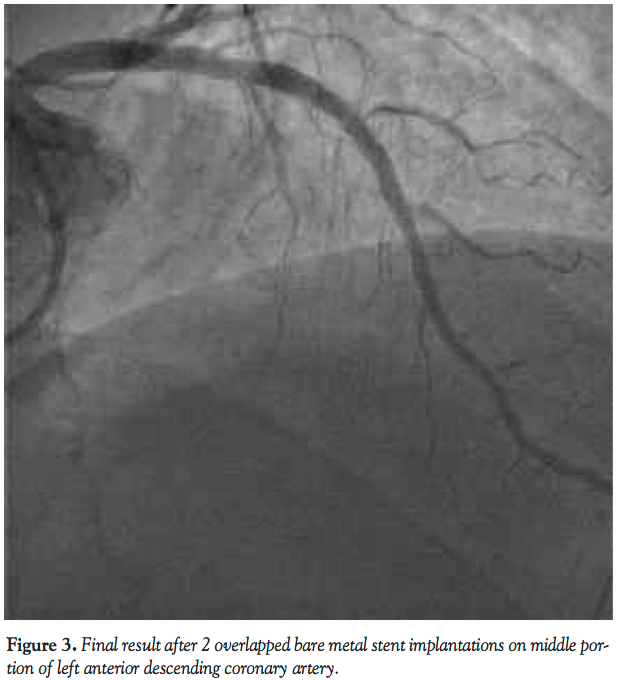 Due to FVIId, revascularization options were discussed between clinical cardiologist, interventional cardiologist, and hematologist. Initially, a provisional PCI on left anterior descending artery was decided, using bare metal stents due to an excellent diabetes mellitus control (glicated hemoglobin of 5.3%) and a shorter dual antiplatelet therapy recommended. A further PCI on obtuse marginal using drug-eluting stents (chronic total occlusion) would be considered depending on symptoms and bleeding events. PCI was also performed by radial approach. The patient was on treatment with aspirin 100 mg/24 H and clopidogrel 75 mg/24 H over 10 days, and both drugs, as 5000 UI of unfractionated heparin, were administered during the procedure (activated clotting time of 218 seconds). Two consecutive bare metal stents (3 mm x 23 mm and 4 mm x 23 mm, Apolo Bionert, IHT Cordynamic) were successfully implanted at middle segment of left anterior descending coronary artery without complications (Figure 3). Recombinant VII factor was not administered to avoid an acute stent thrombosis, but after radial sheath removal complete hemostasis was also achieved with a 4 H bandage.
Due to FVIId, revascularization options were discussed between clinical cardiologist, interventional cardiologist, and hematologist. Initially, a provisional PCI on left anterior descending artery was decided, using bare metal stents due to an excellent diabetes mellitus control (glicated hemoglobin of 5.3%) and a shorter dual antiplatelet therapy recommended. A further PCI on obtuse marginal using drug-eluting stents (chronic total occlusion) would be considered depending on symptoms and bleeding events. PCI was also performed by radial approach. The patient was on treatment with aspirin 100 mg/24 H and clopidogrel 75 mg/24 H over 10 days, and both drugs, as 5000 UI of unfractionated heparin, were administered during the procedure (activated clotting time of 218 seconds). Two consecutive bare metal stents (3 mm x 23 mm and 4 mm x 23 mm, Apolo Bionert, IHT Cordynamic) were successfully implanted at middle segment of left anterior descending coronary artery without complications (Figure 3). Recombinant VII factor was not administered to avoid an acute stent thrombosis, but after radial sheath removal complete hemostasis was also achieved with a 4 H bandage.
After 1 year, the patient is asymptomatic without angina or stent restenosis suspicion. The patient has not presented hemorrhagic events, neither during the first 3 months on dual antiplatelet therapy (aspirin 100 mg plus clopidogrel 75 mg), nor in the last months on aspirin treatment.
Discussion. We report a safe and successful long-term PCI in a patient with FVIId. PCI determines some handicaps in this clinical scenery: first, the optimal periprocedural antithrombotic regimen for stent deployment and later puncture site hemostasis; and second, the need for chronic dual antiplatelet therapy with clopidogrel (at least during 3 months) and lifelong aspirin.8
The presence of diabetes mellitus, left anterior descending artery lesions, and the long chronic occlusion of marginal branch could have supported the surgical revascularization. Even in more severe FVIId, successful surgical revascularization had been described under perioperative FVII substitution.6,7 However, we did not find in the literature any PCI reference9 as absence of evidence concerning the safety of long-term clopidogrel plus aspirin administration in these patients, which is why the final strategy was discussed and surgical revascularization was offered to the patient, but the patient refused it due to his obesity and related risks.
After PCI was decided, the excellent glycemic control allowed a reasonable bare metal stent approach, which seemed to have a lower hemorrhagic profile due to a shorter clopidogrel regimen. Spontaneous bleeding is unlikely to occur if FVIIc is over 20%,4 as occurred in our patient, but in a concomitant antiplatelet therapy this fact is unknown. As FVIId does not protect against thrombosis, antiplatelet therapy was mandatory.3 In PCI cases in which prothrombin activity is reduced by chronic warfarin therapy and dual antiplatelet is mandatory, bleeding episodes usually occur during the first months.10 Our hypothesis was that if there were not significant spontaneous bleeding episodes during the first 3 months (dual antiplatelet therapy), their likelihood would be inferior with aspirin alone, and if no symptoms after 1 year, the procedure could be considered safe and effective.
The standard practice of PCI requires full periprocedural anticoagulation and dual antiplatelet therapy to avoid thrombotic complications.8 A preload of 100 mg of aspirin and 75 mg of clopidogrel a few days before, and only 5000 UI of periprocedural unfractioned heparin (supported by a reduced prothrombin activity) were enough to avoid acute coronary or stent thrombosis. In another congenital coagulation disorder (factor VIII), bivalirudin, has been safely used as well.11,12
Recombinant activated FVII is considered the optimal replacement therapy for FVIId.13 In our case, the simple and successful radial puncture site hemostasis was remarkable, despite the omitted FVII replacement therapy (recommended and used at the first coronarography), even with dual antiplatelet preload and greater heparin dose given, suggesting no need for recombinant FVII administration before a radial arterial sheath removal.
Previous stent placement is considered a formal contraindication for recombinant activated FVII administration due to its thrombin generation enhance and coronary thrombosis predisposition,14 and was one of the key points discussing the PCI approach considering a future major surgery possibility. This contraindication does not consider a chronological assumption, and it is reasonable to think that complete intimal stent struts coverage after some months could equalize the coronary thrombosis risk with a native coronary if a future activated FVII administration was necessary.
Although PCI has been communicated in presence of some other congenital coagulation disorders (factor VIII and XI deficiencies),15 no cases in FVIId have been described before. The case reported suggests the feasibility of performing PCI in patients in FVIId, as well as the safety of long-term dual antiplatelet therapy, and the appropriateness of deferring recombinant activated FVII therapy to achieve a correct hemostasis at radial arterial puncture site.
References
- Cooper DN, Millar DS, Wacey A, Banner DW, Tuddenham EG. Inherited factor VII deficiency: molecular genetics and pathophysiology. Thromb Haemost. 1997;78(1):151-160.
- Giansily-Blaizot M, Schved JF. Potential predictors of bleeding risk in inherited factorVII deficiency. Clinical, biological and molecular criteria. Thromb Haemost. 2005;94(5):901-906.
- Lapecorella M, Mariani G; for the International Registry on Congenital Factor VII Deficiency. Factor VII deficiency: defining the clinical picture and optimizing therapeutic options. Haemophilia. 2008;14(6):1170-1175.
- Giansily-Blaizot M, Biron-Andreani C, Aguilar-Martinez P, et al. Inherited factor VII deficiency and surgery: clinical data are the best criteria to predict the risk of bleeding. Br J Haematol. 2002;117(1):172-175.
- Schulman S, Tjønnfjord GE, Wallensten R, Martinowitz U, Kenet G. Continuous infusion of recombinant factor VIIa for surgery in patients with deficiency of factor VII. Thromb Haemost. 2005;94(6):1177-1180.
- Elsner J, Kalweit G, Frehen D, Gams E. Substitution therapy of congenital factor VII deficiency at an extended operation with extracorporeal circulation. Eur J Cardiothorac Surg. 1999;16(3):387-388.
- Rosenthal C, Volk T, Spies C, Ziemer S, Holinski S, von Heymann C. Successful coronary artery bypass graft surgery in severe congenital factor VII deficiency: perioperative treatment with factor VII concentrate. Thromb Haemost. 2007;98(4):900-902.
- Wijns W, Kolh P, Danchin N, et al; for the Task Force on Myocardial Revascularization of the European Society of Cardiology and the European Association for Cardio-Thoracic Surgery and European Association for Percutaneous Cardiovascular Interventions. Guidelines on myocardial revascularization. Eur Heart J. 2010;31(20):2501-2555.
- Mariani G, Dolce A, Batorova A, et al; for the STER and the International Factor VII Deficiency Study Groups. Recombinant, activated factor VII for surgery in factor VII deficiency: a prospective evaluation - the surgical STER. Br J Haematol. 2011;152(3):340-346.
- Karjalainen PP, Porela P, Ylitalo A, et al. Safety and efficacy of combined antiplatelet-warfarin therapy after coronary stenting. Eur Heart J. 2007;28(6):726-732.
- Arora UK, Dhir M, Cintron G, Strom JA. Successful multi-vessel percutaneous coronary intervention with bivalirudin in a patient with severe hemophilia A: a case report and review of literature. J Invasive Cardiol. 2004;16(6):330-332.
- Krolick MA. Successful percutaneous coronary intervention in a patient with severe hemophilia A using bivalirudin as the sole procedural anticoagulant. Haemophilia. 2005;11(4):415-417.
- Mariani G, Konkle BA, Ingerslev J. Congenital factor VII deficiency: therapy with recombinant activated factor VII--a critical appraisal. Haemophilia. 2006;12(1):19-27.
- Franchini M, Zaffanello M, Veneri D. Recombinant factor VII: an update on its clinical use. Thromb Haemost. 2005;93(6):1027-1035.
- Shimony A, Levi E, Zahger D. Percutaneous coronary intervention in a patient with factor XI deficiency. J Invasive Cardiol. 2009;21(9):E178-179.
________________________________________
From the 1Interventional Cardiology Unit, Cardiology Department, Clinic Universitary Hospital “Lozano Blesa”, Zaragoza, Spain; and the 2Haematology Department, Clinic Universitary Hospital “Lozano Blesa”, Zaragoza, Spain.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 26, 2011, provisional acceptance given December 20, 2011, final version accepted January 20, 2012.
Address for correspondence: Dr. Jose A. Linares Vicente, MD, Interventional Cardiology Unit, Cardiology Department, Clinic Universitary Hospital “Lozano Blesa”, Av. San Juan Bosco, 15, 50009, Zaragoza, Spain. Email: joselinares1979@hotmail.com