

Longitudinal Stent Compression is Not Always a Bad Event: A Case Report
ABSTRACT: Ostial left anterior descending artery stent implantation was performed, while trying to cross another stent through the left main coronary artery into the left circumflex artery the stent was detached from the delivery balloon, subsequently jamming the stent of the ostial left anterior descending artery stent. Removing the detached stent was possible, but longitudinal compression of the ostial left anterior descending artery stent occurred. We finally took advantage of the longitudinal compression to advance the equipment into the left circumflex artery with good final result.
J INVASIVE CARDIOL 2012;24(8):E167-E169
_____________________________________________________
Case Report. A 66-year-old male smoker with long-standing systemic arterial hypertension was seen at our facility, complaining of a 5-month crescendo angina and a syncopal episode during an angina event. The ECG showed a first-degree AV block and a possible septal infarct. At the time of presentation he was asymptomatic, a TL-201 gated myocardial perfusion imaging study showed a nontransmural myocardial infarction of the apex with anteroseptal and lateral wall extension with severe residual ischemia as well as mild inferolateral ischemia and moderate left ventricular dysfunction.
 The patient was sent for coronary artery catheterization that was performed via right radial artery approach (6 Fr Glidesheat and 5 Fr Optitorque radial TIG catheter Terumo interventional systems). The angiographic findings were a mild mid left main coronary artery (LMCA) lesion, a partially recanalized chronic left anterior descending (LAD) coronary artery proximal occlusion with excellent collaterals, severe proximal left circumflex (LCX), mid obtuse marginal (OM) stenosis (Figure 1A), and a severe stenosis of the bifurcation compromising the posterior descending and posterolateral branches of the right coronary artery (not shown in figures).
The patient was sent for coronary artery catheterization that was performed via right radial artery approach (6 Fr Glidesheat and 5 Fr Optitorque radial TIG catheter Terumo interventional systems). The angiographic findings were a mild mid left main coronary artery (LMCA) lesion, a partially recanalized chronic left anterior descending (LAD) coronary artery proximal occlusion with excellent collaterals, severe proximal left circumflex (LCX), mid obtuse marginal (OM) stenosis (Figure 1A), and a severe stenosis of the bifurcation compromising the posterior descending and posterolateral branches of the right coronary artery (not shown in figures).
The patient refused coronary artery bypass graft surgery and we therefore performed a percutaneous coronary intervention (PCI) by the radial artery approach. The LMCA was engaged with an EBU 3.5 6 Fr guiding catheter. The LAD occlusion was crossed using a 0.014” Pilot 50 guidewire (Abbott Vascular), and subsequently pre-dilated with a 2.0 mm x 20 mm Maverick (Boston Scientific) in several occasions at 10 atm of pressure, achieving TIMI 2 coronary artery flow. We then deployed 2 overlapping Endeavor Resolute cobalt-chromium drug-eluting stents (DES) (Medtronic Inc.) at 12 atm from distal to proximal, 2.5 mm x 30 mm and 2.75 mm x 24 mm, respectively. During the delivery of the proximal stent, a type B dissection developed within the ostium of the LAD extension and anterograde flow compromise (Figure 1B), which forced us to deploy another ostial 2.75 mm x 18 mm overlapped Endeavor Resolute DES despite the risk of jailing the origin of the LCX. The stent was deployed at 12 atm with good angiographic result re-establishing TIMI 3 flow.
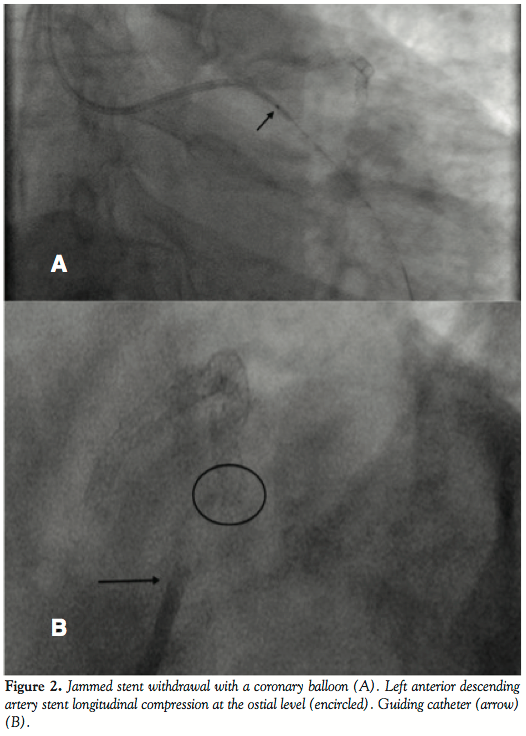 A 0.014” BMW guidewire (Abbott Vascular) was then used to cross into the LCX to perform PCI to the OM immediately distal to a posterolateral branch. While trying to cross with a stent (2.5 mm x 15 mm Promus platinum-chromium DES [Boston Scientific]) through the LMCA into the LCX, the stent was detached from the delivery balloon, subsequently jamming the ostial LAD stent (Figure 1C). This precluded the possibility to further advance the stent to the distal segment of the OM and prevented deployment at the actual detached position due to the compromise of the LMCA, LAD ostial stent, and LCX, which were not the intended segments to treat. Fortunately we were able to maintain wire position across the non-expanded stent. A new 1.5 mm x 12 mm Sprinter coronary balloon (Medtronic) was positioned distal to the detached stent (Figure 2A), and applying low atmospheres for its inflation, we pulled the system (balloon-stent-guidewire-guiding catheter) back into the distal radial artery and removed it, including the glide sheath, without damaging the radial artery.
A 0.014” BMW guidewire (Abbott Vascular) was then used to cross into the LCX to perform PCI to the OM immediately distal to a posterolateral branch. While trying to cross with a stent (2.5 mm x 15 mm Promus platinum-chromium DES [Boston Scientific]) through the LMCA into the LCX, the stent was detached from the delivery balloon, subsequently jamming the ostial LAD stent (Figure 1C). This precluded the possibility to further advance the stent to the distal segment of the OM and prevented deployment at the actual detached position due to the compromise of the LMCA, LAD ostial stent, and LCX, which were not the intended segments to treat. Fortunately we were able to maintain wire position across the non-expanded stent. A new 1.5 mm x 12 mm Sprinter coronary balloon (Medtronic) was positioned distal to the detached stent (Figure 2A), and applying low atmospheres for its inflation, we pulled the system (balloon-stent-guidewire-guiding catheter) back into the distal radial artery and removed it, including the glide sheath, without damaging the radial artery.
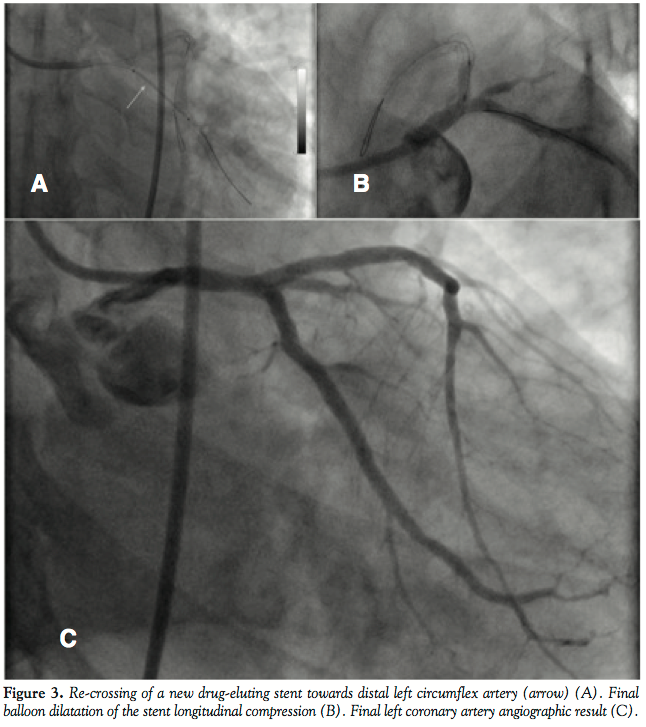 We decided to gain right femoral artery access in order to use a 7 Fr system to improve guiding catheter support, alignment, and to protect the LAD during performance of a certainly difficult procedure. The first angiogram showed the presence of a longitudinal compression of the ostial LAD stent (Figure 2B) probably due to the previous forceful withdrawal of the detached and jammed stent with secondary and involuntary deep guiding catheter intubation. We decided to wire the LCX and the LAD with BMW guidewires and, taking advantage of the longitudinal compression of the LAD stent, we were able to easily advance balloons and stents into the distal segments of the OM (Figure 3A). Then 2 non-overlapped Endeavor Resolute DES (2.5 mm x 18 mm an 2.75 mm x 24 mm) were delivered to the LCX without difficulties, resulting in a good final angiographic result with no further compromise of the ostial LAD stent.
We decided to gain right femoral artery access in order to use a 7 Fr system to improve guiding catheter support, alignment, and to protect the LAD during performance of a certainly difficult procedure. The first angiogram showed the presence of a longitudinal compression of the ostial LAD stent (Figure 2B) probably due to the previous forceful withdrawal of the detached and jammed stent with secondary and involuntary deep guiding catheter intubation. We decided to wire the LCX and the LAD with BMW guidewires and, taking advantage of the longitudinal compression of the LAD stent, we were able to easily advance balloons and stents into the distal segments of the OM (Figure 3A). Then 2 non-overlapped Endeavor Resolute DES (2.5 mm x 18 mm an 2.75 mm x 24 mm) were delivered to the LCX without difficulties, resulting in a good final angiographic result with no further compromise of the ostial LAD stent.
Finally balloon re-expansion of the DES longitudinal compression was performed with a Voyager (Abbott Vascular) 3.0 mm x 12 mm at 12 atm (Figure 3B), with complete resolution of the stent compression and a good final angiographic result (figure 3C).
Angioplasty with stenting to RCA was performed a few days later also with good results. The patient continues to be free of angina almost a year after PCI.
Discussion. When treating ostial lesions in the LAD or LCX, stent protrusion into the LMCA may interfere with your ability to cross into the other vessel. Therefore, it is advisable first to treat the other vessel lesions, before deploying ostial stents that could prevent the other vessel treatment. However, if you are forced into treating any ostium of the LMCA bifurcation, it is essential to position a second wire into the other artery to ensure patency. In our case, we suffered the stent detachment due to the interference with the ostial LAD stent to cross to the LCX. It is always advisable when this kind of complications occurs to try to minimize deep guiding catheter intubation during forceful pullback of the system in order to avoid harm to the LMCA or a nearby previously delivered stent, preventing the longitudinal compression incident. Nevertheless we finally took advantage of the longitudinal compression to advance the equipment into the LCX. Staging the post-dilatation of the deformed stent allowed us to treat the LCX and we were able to avoid a potentially catastrophic situation.
_____________________________________________________
From the Cardiovascular and Interventional Cardiology Unit, Hospital Regional 1º de Octubre ISSSTE, Mexico City.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted January 24, 2012, provisional acceptance given February 22, 2012, final version accepted April 10, 2012.
Address for correspondence: Dr Alejandro Alcocer, Interventional Cardiologist
Alcocer Cardiologos Asociados SC, Tuxpan 16, 8VO PISO, Cuauhtemoc, Mexico City, DF 06760 Mexico. Email: alcocerchauvet@gmail.com











