

Management of Drug-Eluting Stent Restenosis
Abstract: In-stent restenosis has been a longstanding problem after percutaneous coronary intervention. The introduction of the drug-eluting stent (DES) successfully reduced the rate of restenosis; however, it is not completely diminished. Although restenosis occurs less frequently compared to the bare-metal stent (BMS), DES restenosis remains a familiar problem due to the increasing total number of implanted DESs as well as the targeting of more complex lesions. In addition, worse outcomes after repeat revascularization compared to BMS restenosis are reported in DES restenosis. Management of DES restenosis is an emerging issue, which requires careful evaluation of the restenosed lesion, together with cautious determination of therapeutic strategy. In this review, available repeat revascularization procedures for DES restenosis as well as possible impacting factors on the outcomes are discussed.
J INVASIVE CARDIOL 2012;24(4):178-182
Key words: coronary interventions, CABG versus PCI, in-stent restenosis, stenting
___________________________________________
The introduction of the drug-eluting stent (DES) has significantly changed the world of clinical percutaneous coronary intervention (PCI). A dramatic reduction of in-stent restenosis (ISR) when compared to a bare-metal stent (BMS) prompted an explosive number of DES implantations. Initially, DES restenosis was considered no different from BMS restenosis, and stent thrombosis emerged as a major focus of DES complications due to the suspected mechanism related to the delayed endothelialization that is unique to DES. However, multiple studies revealed worse outcomes after PCI for DES restenosis compared to BMS restenosis.1-3 This may be associated with a weak response to the DES, such as drug resistance,4 in a portion of patients. Although the rate of restenosis after DES implantation is significantly lower than we had in the BMS era,5,6 the total number of restenoses is increasing as the number of implanted DESs is increasing.7 Therefore, it is important to recognize the consequences of repeat PCI for DES restenosis and select the optimal treatment for each case. This review focuses on the available approaches for DES failure and the potential factors that may affect the outcomes.
Overview
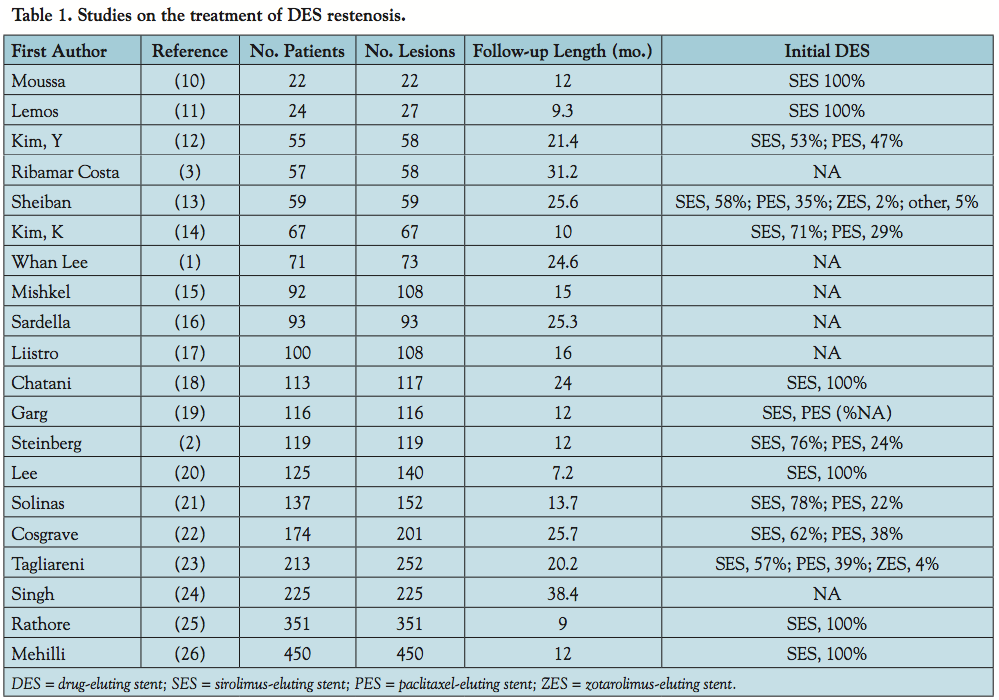 A number of studies have reported the clinical and angiographic outcomes after revascularization procedures for DES restenosis.1-3,8-24 Most were targeted at the restenosis of first-generation DESs, which are sirolimus-eluting (SES) and paclitaxel-eluting stents (PES), and there are very few cases of restenosis in the new generation of DES. In these studies, revascularization was mainly performed with PCI and the comparison was made between the PCI procedures. The available results of studies that investigated repeat revascularization for
A number of studies have reported the clinical and angiographic outcomes after revascularization procedures for DES restenosis.1-3,8-24 Most were targeted at the restenosis of first-generation DESs, which are sirolimus-eluting (SES) and paclitaxel-eluting stents (PES), and there are very few cases of restenosis in the new generation of DES. In these studies, revascularization was mainly performed with PCI and the comparison was made between the PCI procedures. The available results of studies that investigated repeat revascularization for 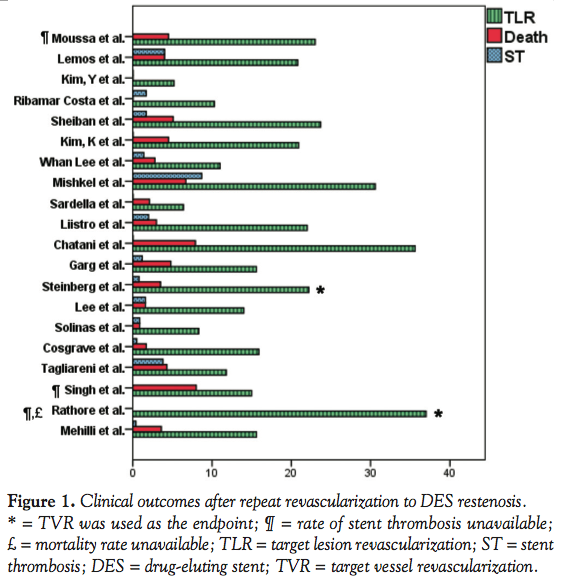 DES restenosis are shown in Table 1 and Figure 1. Target lesion revascularization (TLR) ranged from 5%-35%, stent thrombosis from 0%-9%, and mortality rate from 0%-8%. Because device used, set endpoint, and length of study were all different, it is difficult to recapitulate a conclusion from these studies. However, some factors did show trends toward the same direction. The available procedures for revascularization will be discussed, as well as lesion characteristics that may affect the results of intervention.
DES restenosis are shown in Table 1 and Figure 1. Target lesion revascularization (TLR) ranged from 5%-35%, stent thrombosis from 0%-9%, and mortality rate from 0%-8%. Because device used, set endpoint, and length of study were all different, it is difficult to recapitulate a conclusion from these studies. However, some factors did show trends toward the same direction. The available procedures for revascularization will be discussed, as well as lesion characteristics that may affect the results of intervention.
Revascularization Approaches
 Stenting. Efficacious results of DES over balloon angioplasty,25 BMS,26 and brachytherapy27 for BMS-ISR made clinicians hope for a similar outcome in DES implantations for DES-ISR. Readily available devices also facilitated DES use for DES-ISR in daily practice. Although this approach seems safe and feasible, Ribamar Costa et al showed less efficacy of DES for DES-ISR compared to DES for BMS-ISR.3 This result suggests the influence of drug resistance or hypersensitivity to the polymer. Several studies examined the theory that implanting a different type of DES may be effective in a DES failure due to using different drugs as well as a different polymer (Figure 2). Contrary to the expectations, only one study showed a significant difference between the same and different DES strategies.16 However, a large randomized study by Mehili et al showed no significant difference when using either same or different DES for DES-ISR.24 Because this study targeted only SES-ISR, there may be a chance of improving the outcome by using different DESs for PES-ISR. In addition, the new generation of DES also possesses the potential to improve the results since everolimus-eluting stents have been shown to have better outcomes compared to PES.28 If the restenosis is due to hypersensitivity, BMS may also be effective; however, there are almost no data on outcomes after BMS implantation for DES-ISR.
Stenting. Efficacious results of DES over balloon angioplasty,25 BMS,26 and brachytherapy27 for BMS-ISR made clinicians hope for a similar outcome in DES implantations for DES-ISR. Readily available devices also facilitated DES use for DES-ISR in daily practice. Although this approach seems safe and feasible, Ribamar Costa et al showed less efficacy of DES for DES-ISR compared to DES for BMS-ISR.3 This result suggests the influence of drug resistance or hypersensitivity to the polymer. Several studies examined the theory that implanting a different type of DES may be effective in a DES failure due to using different drugs as well as a different polymer (Figure 2). Contrary to the expectations, only one study showed a significant difference between the same and different DES strategies.16 However, a large randomized study by Mehili et al showed no significant difference when using either same or different DES for DES-ISR.24 Because this study targeted only SES-ISR, there may be a chance of improving the outcome by using different DESs for PES-ISR. In addition, the new generation of DES also possesses the potential to improve the results since everolimus-eluting stents have been shown to have better outcomes compared to PES.28 If the restenosis is due to hypersensitivity, BMS may also be effective; however, there are almost no data on outcomes after BMS implantation for DES-ISR.
Balloon. Balloon therapy is the other method frequently used to treat DES-ISR other than stent implantation. Several balloon types are widely available and used depending on the restenosis pattern. Plain old balloon angioplasty (POBA) is used in underexpanded lesions, whereas cutting balloons and similar devices are used in proliferative lesions aiming to decrease neointimal thickening by reducing the vessel trauma. Currently, intravascular ultrasound (IVUS) is the best way to distinguish the possible causes of DES restenosis. Underexpansion was frequently observed in cases of SES restenosis,29 whereas diameter stenosis after a second PCI was associated with recurrent restenosis.8,18 Therefore, using an IVUS for detecting underexpansion as well as checking the vessel size to obtain the maximum expansion could be useful in these cases. Although recurrent restenosis seems more prevalent after balloon intervention than DES,9,16 no significant differences have been reported on TLR or major adverse cardiac events (MACE). A larger sample size may show the superiority of DES over ballooning in these hard endpoints. However, current data, when considered along with the benefits of not implanting another stent as well as the economical point of view, suggest balloon therapy to be the most effective therapy for DES-ISR treatment.
Drug-eluting balloons. Recent advancements of balloon devices brought in a drug-eluting balloon as a new therapeutic device for treating ISR. Drug-eluting balloons share the common features of balloon therapy while maintaining the antiproliferative properties of DES. BMS-ISR treated by paclitaxel-coated balloons showed significantly lower restenosis and TLR compared to non-drug coated balloons for up to 2 years.30 Delivery of an anti-restenotic agent without adding a second layer of metal is the most attractive feature of this device and therefore has great potential for being the best strategy for DES-ISR. However, recent results of paclitaxel-coated balloon in 126 patients with ISR showed higher rates of 12-month MACE and TLR in DES-ISR than BMS-ISR, although there was no significant difference.31 At this point, the data available are too few and further study is needed to determine the utility of this device for DES-ISR.
Coronary artery bypass graft (CABG) surgery. To date, there are few studies that compared the outcomes of PCI and CABG to DES-ISR. Due to the different nature of the intervention procedures, it is difficult to compare the angiographic outcomes such as restenosis and late loss between PCI and surgery. However, considering the relatively low target vascular failure after CABG,32 surgery might be the best revascularization procedure for DES-ISR in a subset of patients. Sheiban et al followed 70 patients in different treatment groups with DES-ISR with unprotected left main coronary artery, and showed the lowest MACE rate in the CABG group compared to medication only and PCI.11 In our data on 176 lesions with SES restenosis, MACE rate was significantly lower after CABG compared to the PCI strategies (unpublished data). Although CABG is highly invasive, some patients who may gain more benefit, such as patients with existing valve disease or past history of major bleeding, should always be considered for this revascularization procedure.
Vascular brachytherapy. Although early results of vascular brachytherapy for ISR seemed promising,33 concerns about late stent thrombosis as well as a high rate of late restenosis due to late catch-up34 have been reported. In addition to these safety and efficacy concerns,35 a complex apparatus with a well-refined technique to deliver the adequate dose of radiation limits the application of this treatment in daily practice. The superior outcome of DES over brachytherapy for BMS-ISR also discourages selecting this therapy as a first choice.
Restenosis Pattern
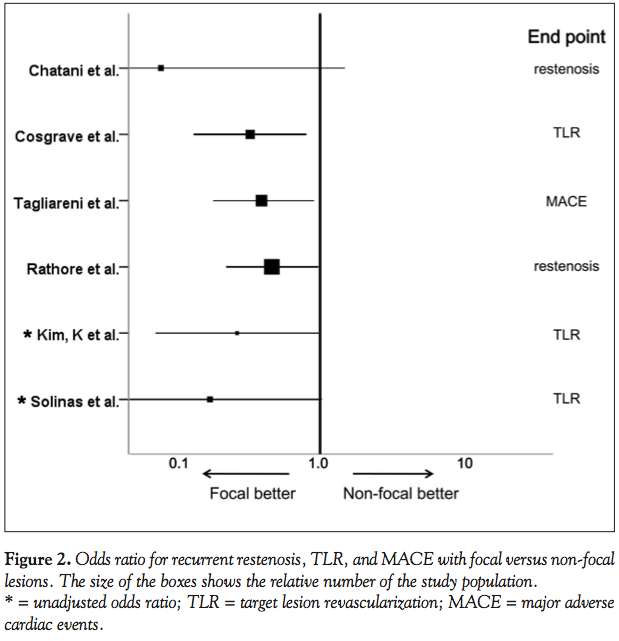
 Focal or non-focal. The outcome after treatment of BMS-ISR was significantly better in a focal pattern of restenosis.36,37 Mehran et al classified the angiographic pattern of BMS-ISR into four groups, and showed the increasing rates of repeat revascularization in more diffuse patterns of restenosis.37 There are some studies that investigated the influence of restenosis pattern on the outcome of repeat revascularization for DES-ISR. Most of these studies used the simplified classification based on that of Mehran et al, and compared the outcomes of focal ISR (lesions <10 mm) and non-focal ISR (lesions >10 mm, occlusive lesions). In line with the results of BMS-ISR, focal pattern of restenosis seems to have better outcomes compared to the non-focal pattern (Figure 3). PES restenosis has been shown to have a higher rate restenosis pattern, whereas SES restenosis was associated with a more focal pattern.29,38 Therefore, SES restenosis may have a favorable outcome after repeat PCI; however, no study has confirmed the different outcomes of repeat PCI between SES and PES-ISR. The higher incidence of non-focal restenosis in the “real-world” compared to the initial stage of DES studies39 may lead to increased revascularization failure in the clinical setting.
Focal or non-focal. The outcome after treatment of BMS-ISR was significantly better in a focal pattern of restenosis.36,37 Mehran et al classified the angiographic pattern of BMS-ISR into four groups, and showed the increasing rates of repeat revascularization in more diffuse patterns of restenosis.37 There are some studies that investigated the influence of restenosis pattern on the outcome of repeat revascularization for DES-ISR. Most of these studies used the simplified classification based on that of Mehran et al, and compared the outcomes of focal ISR (lesions <10 mm) and non-focal ISR (lesions >10 mm, occlusive lesions). In line with the results of BMS-ISR, focal pattern of restenosis seems to have better outcomes compared to the non-focal pattern (Figure 3). PES restenosis has been shown to have a higher rate restenosis pattern, whereas SES restenosis was associated with a more focal pattern.29,38 Therefore, SES restenosis may have a favorable outcome after repeat PCI; however, no study has confirmed the different outcomes of repeat PCI between SES and PES-ISR. The higher incidence of non-focal restenosis in the “real-world” compared to the initial stage of DES studies39 may lead to increased revascularization failure in the clinical setting.
Stent fracture, gap. Stent fracture is recognized as one of the contributors to DES-ISR40 and the rates of DES fracture have been reported to range from 1%-16%.40,41 Multiple factors are known to be associated with increased risk of stent fracture, such as right coronary artery lesions, overlapping stents, SES, etc.40 Stent gap is a similar condition to stent fracture in terms of deficient local drug delivery and scaffolding support. Especially when there is a geographic miss at the initial DES implantation, the chances of developing restenosis at the gap will be higher. Given the potential cause of the restenosis, adding another DES at the restenosis site seems reasonable if only the fracture site or the gap site presented restenosis. In the case of stent fracture, a flexible stent should be chosen to avoid recurrent fracture.
Target
Small arteries. The dramatic reduction of restenosis led to the expanded “off-label” use of DES in the “real-world.” As a result, the rate of restenosis became higher compared to the initial DES studies,5,6 which targeted “on-label” use of DES. The most widely employed “off-label” use is the DES application to small arteries. Because the original lumen diameter is small, the incidence of restenosis gets higher even with a little late loss. The initial size of the artery is an important factor that impacts the outcome of repeat PCI. In fact, the size of the initial stent was significantly smaller in lesions with recurrent restenosis after SES restenosis.16 When restenosis develops in the small artery, DES treatment is undesirable because it limits the size of the inner lumen. In these cases, underexpansion needs to be carefully examined and must be avoided. Thus, IVUS use is recommended to identify the underexpansion, as well as size of the vessel to expand the stent as much as possible.
Left main. The excellent results of DES prompted the use of DES in one of the most important locations of the coronary artery, ie, the left main. The aforementioned study by Sheiban et al is the only study that reported the outcomes of PCI, CABG, and medical treatment for unprotected left main DES restenosis.11 After 27.2 ± 15.4 months of follow-up, MACE occurred in 50% of the patients treated medically, 25.4% treated with PCI, and 14.3% after CABG. Due to the small number of studied patients, there were no statistically significant differences found among the treatment strategies. However, if a stent thrombosis took place at the left main coronary artery, it will be inevitably fatal. Therefore, a cautious stance should be taken for repeat DES placement at this location.
Bifurcation. The condition of the restenosis at the bifurcation site varies based on the strategy taken at the initial DES implantation. The main branch usually has at least one stent, and some strategies apply another stent implantation for the side branch. In any case, repeat revascularization for the restenosis should be attempted without adding stents to the greatest extent possible, because the double layer of stent strut at the ostium of the side branch raises the risk of obstructing the side-branch flow. In fact, patients who received multiple PES have been shown to have a significant increase in non-Q wave myocardial infarction due to increased rates of side-branch compromise.42
Risk Factors for Recurrent Restenosis
Identifying the predictive factors for DES re-restenosis is challenging due to the various impacting factors from initial DES placement and the second procedure. Lemos et al reported increased incidence of recurrent restenosis in patients with hypercholesterolemia (lipid-lowering therapy or total cholesterol >200 mg/dL) in 27 lesions of SES restenosis.9 However, this is the only study that reported hypercholesterolemia as a predictive recurrent restenosis factor. Interestingly, none of the studies have shown the increased risk of recurrent restenosis or TLR in diabetic patients in contrast to BMS-ISR.37 Other predictive factors related to patient characteristic are previous PCI9 and multiple episodes of restenosis in the past.20 Early recurrence of restenosis (<6 months) has also been reported as a predictor of recurrent restenosis,9 TLR,8 and MACE21 after the treatment of DES restenosis. These results suggest that the patients with more progressive neointimal growth are at risk of recurrent restenosis. The length of stent,8,18 reference diameter before second PCI,16,23 and size of initial DES16 are other reported predictors of recurrent restenosis. Longer lesion and smaller size seem to be common risk factors of restenosis after other PCI procedures.
Antiplatelet Therapy
The current guideline recommends at least 12 months of dual antiplatelet therapy after DES implantation to de novo lesions.43 However, no guidelines or consensus are available for antiplatelet therapy after PCI for DES restenosis. As seen in Figure 1, the rate of stent thrombosis after repeat PCI for DES restenosis is relatively high, especially when considering the length of follow-up in these studies. Tagliareni et al compared the clinical outcomes of patients after repeat DES implantation and after balloon angioplasty alone for DES-ISR, and showed a higher rate of myocardial infarction occurrence as well as stent thrombosis in the repeat DES group.21 A double layer of DES renders a higher drug dose, which leads to delayed endothelialization, heterogeneous distribution of drug release, and suboptimal stent geometry inside the lesion. Therefore, a longer duration of dual antiplatelet therapy should be considered after repeat DES implantation. Triple antiplatelet therapy with cilostazol can also be effective, since it has been shown to decrease late loss as well as decrease restenosis after stent implantation.44 Because the major reason for stent thrombosis is considered to be incomplete endothelialization over the stent, antiplatelet therapy after balloon angioplasty could be shortened as the stent is already covered with proliferated neointima. However, the restenosis may derive from heterogeneous distribution of the drug, thus uneven distribution of neointima formation can be observed. Careful assessment with IVUS may be helpful to determine the neointima coverage inside the DES.
Conclusion
Although a numbers of studies reported the outcome after repeat revascularization to DES restenosis, the results vary because of different endpoints and the study duration after PCI. In addition, the time of recurrent restenosis after PCI and the antiplatelet therapy used differs depending on the procedure performed. These factors preclude direct comparison of available procedures for DES restenosis. However, a relatively high rate of recurrent restenosis as well as high TLR compared to the favorable results of DES to BMS-ISR has been reported. Thus, indication of repeat PCI needs to be deliberately decided with careful evaluation of ischemia. When there is a demand for repeat revascularization, the aforementioned risk factors should be taken into consideration. Furthermore, the SYNTAX study showed that the complexity of the coronary artery disease affects the outcome after PCI, while CABG was independent of the complexity score.32 Together with the higher risk of repeat TLR after PCI to DES restenosis, CABG should be recommended in a portion of patients. In addition, IVUS is highly useful in DES restenosis for both determining the cause of restenosis and developing the revascularization strategy. Conclusive results from ongoing randomized studies as well as further development of revascularization procedures for DES restenosis are awaited to improve the prognosis of DES restenosis.
Acknowledgments. The authors would like to thank Lauren Leonardson for editorial assistance.
References
- Whan Lee C, Kim SH, Suh J, et al. Long-term clinical outcomes after sirolimus-eluting stent implantation for treatment of restenosis within bare-metal versus drug-eluting stents. Catheter Cardiovasc Interv. 2008;71(5):594-598.
- Steinberg DH, Gaglia MA Jr, Pinto Slottow TL, et al. Outcome differences with the use of drug-eluting stents for the treatment of in-stent restenosis of bare-metal stents versus drug-eluting stents. Am J Cardiol. 2009;103(4):491-495.
- Ribamar Costa J, Sousa AG, Moreira A, et al. Comparison of the very long term (>1 year) outcomes of drug-eluting stents for the treatment of bare-metal and drug-eluting stent restenosis. EuroIntervention. 2009;5(4):448-453.
- Costa MA. Treatment of drug-eluting stent restenosis. Am Heart J. 2007;153(4):447-449.
- Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346(23):1773-1780.
- Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349(14):1315-1323.
- Epstein AJ, Polsky D, Yang F, et al. Coronary revascularization trends in the United States, 2001-2008. JAMA. 2011;305(17):1769-1776.
- Moussa ID, Moses JW, Kuntz RE, et al. The fate of patients with clinical recurrence after sirolimus-eluting stent implantation (a two-year follow-up analysis from the sirius trial). Am J Cardiol. 2006;97:(11)1582-1584.
- Lemos PA, van Mieghem CA, Arampatzis CA, et al. Post-sirolimus-eluting stent restenosis treated with repeat percutaneous intervention: Late angiographic and clinical outcomes. Circulation. 2004;109(21):2500-2502.
- Kim YH, Lee BK, Park DW, et al. Comparison with conventional therapies of repeated sirolimus-eluting stent implantation for the treatment of drug-eluting coronary stent restenosis. Am J Cardiol. 2006;98(11):1451-1454.
- Sheiban I, Sillano D, Biondi-Zoccai G, et al. Incidence and management of restenosis after treatment of unprotected left main disease with drug-eluting stents 70 restenotic cases from a cohort of 718 patients: fails (failure in left main study). J Am Coll Cardiol. 2009;54(13):1131-1136.
- Kim KH, Kim DI, Kim IH, et al. Therapeutic strategy for in-stent restenosis based on the restenosis pattern after drug-eluting stent implantation. Korean Circ J. 2009;39(10):408-413.
- Mishkel GJ, Moore AL, Markwell S, et al. Long-term outcomes after management of restenosis or thrombosis of drug-eluting stents. J Am Coll Cardiol. 2007;49(2):181-184.
- Sardella G, Colantonio R, De Luca L, et al. Comparison between balloon angioplasty and additional coronary stent implantation for the treatment of drug-eluting stent restenosis: 18-month clinical outcomes. J Cardiovasc Med (Hagerstown). 2009;10(6):469-473.
- Liistro F, Fineschi M, Grotti S, et al. Long-term clinical outcome of alternative treatment strategies for drug-eluting stents restenosis. EuroIntervention. 2009;5(4):454-459.
- Chatani K, Muramatsu T, Tsukahara R, et al. Predictive factors of re-restenosis after repeated sirolimus-eluting stent implantation for SES restenosis and clinical outcomes after percutaneous coronary intervention for SES restenosis. J Interv Cardiol. 2009;22(4):354-361.
- Garg S, Smith K, Torguson R, et al. Treatment of drug-eluting stent restenosis with the same versus different drug-eluting stent. Catheter Cardiovasc Interv. 2007;70(1):9-14.
- Lee SS, Price MJ, Wong GB, et al. Early- and medium-term outcomes after paclitaxel-eluting stent implantation for sirolimus-eluting stent failure. Am J Cardiol. 2006;98(10):1345-1348.
- Solinas E, Dangas G, Kirtane AJ, et al. Angiographic patterns of drug-eluting stent restenosis and one-year outcomes after treatment with repeated percutaneous coronary intervention. Am J Cardiol. 2008;102(3):311-315.
- Cosgrave J, Melzi G, Corbett S, et al. Repeated drug-eluting stent implantation for drug-eluting stent restenosis: the same or a different stent. Am Heart J. 2007;153(3):354-359.
- Tagliareni F, La Manna A, Saia F, et al. Long-term clinical follow-up of drug-eluting stent restenosis treatment: retrospective analysis from two high volume catheterisation laboratories. EuroIntervention. 2010;5(6):703-708.
- Singh IM, Filby SJ, Sakr FE, et al. Clinical outcomes of drug-eluting versus bare-metal in-stent restenosis. Catheter Cardiovasc Interv. 2010;75(3):338-342.
- Rathore S, Kinoshita Y, Terashima M, et al. A comparison of clinical presentations, angiographic patterns and outcomes of in-stent restenosis between bare-metal stents and drug-eluting stents. EuroIntervention. 2010;5(7):841-846.
- Mehilli J, Byrne RA, Tiroch K, et al. Randomized trial of paclitaxel- versus sirolimus-eluting stents for treatment of coronary restenosis in sirolimus-eluting stents: the ISAR-DESIRE 2 (intracoronary stenting and angiographic results: drug-eluting stents for in-stent restenosis 2) study. J Am Coll Cardiol. 2010;55(24):2710-2716.
- Kastrati A, Mehilli J, von Beckerath N, et al. Sirolimus-eluting stent or paclitaxel-eluting stent vs balloon angioplasty for prevention of recurrences in patients with coronary in-stent restenosis: a randomized controlled trial. JAMA. 2005;293(2):165-171.
- Alfonso F, Perez-Vizcayno MJ, Hernandez R, et al. Sirolimus-eluting stents versus bare-metal stents in patients with in-stent restenosis: results of a pooled analysis of two randomized studies. Catheter Cardiovasc Interv. 2008;72(4):459-467.
- Stone GW, Ellis SG, O’Shaughnessy CD, et al. Paclitaxel-eluting stents vs vascular brachytherapy for in-stent restenosis within bare-metal stents: The TAXUS V ISR randomized trial. JAMA. 2006;295(11):1253-1263.
- Kedhi E, Joesoef KS, McFadden E, et al. Second-generation everolimus-eluting and paclitaxel-eluting stents in real-life practice (COMPARE): a randomised trial. Lancet. 2010;375(9710):201-209.
- Aminian A, Kabir T, Eeckhout E. Treatment of drug-eluting stent restenosis: an emerging challenge. Catheter Cardiovasc Interv. 2009;74(1):108-116.
- Scheller B, Hehrlein C, Bocksch W, et al. Two year follow-up after treatment of coronary in-stent restenosis with a paclitaxel-coated balloon catheter. Clin Res Cardiol. 2008;97(10):773-781.
- Vaquerizo B, Serra A, Miranda-Guardiola F, et al. One-year outcomes with angiographic follow-up of paclitaxel-eluting balloon for the treatment of in-stent restenosis: insights from Spanish multicenter registry. J Interv Cardiol. 2011;24(6):518-528.
- Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972.
- Torguson R, Sabate M, Deible R, et al. Intravascular brachytherapy versus drug-eluting stents for the treatment of patients with drug-eluting stent restenosis. Am J Cardiol. 2006;98(10):1340-1344.
- Feres F, Munoz J, Abizaid A, et al. Angiographic and intravascular ultrasound findings of the late catch-up phenomenon after intracoronary beta-radiation for the treatment of in-stent restenosis. J Invasive Cardiol. 2005;17(9):473-477.
- Waksman R, Ajani AE, White RL, et al. Five-year follow-up after intracoronary gamma radiation therapy for in-stent restenosis. Circulation. 2004;109(3):340-344.
- Adamian M, Colombo A, Briguori C, et al. Cutting balloon angioplasty for the treatment of in-stent restenosis: a matched comparison with rotational atherectomy, additional stent implantation and balloon angioplasty. J Am Coll Cardiol. 2001;38(3):672-679.
- Mehran R, Dangas G, Abizaid AS, et al. Angiographic patterns of in-stent restenosis: classification and implications for long-term outcome. Circulation. 1999;100(18):1872-1878.
- Corbett SJ, Cosgrave J, Melzi G, et al. Patterns of restenosis after drug-eluting stent implantation: insights from a contemporary and comparative analysis of sirolimus- and paclitaxel-eluting stents. Eur Heart J. 2006;27(19):2330-2337.
- Dangas GD, Claessen BE, Caixeta A, et al. In-stent restenosis in the drug-eluting stent era. J Am Coll Cardiol. 2010;56(23):1897-1907.
- Aoki J, Nakazawa G, Tanabe K, et al. Incidence and clinical impact of coronary stent fracture after sirolimus-eluting stent implantation. Catheter Cardiovasc Interv. 2007;69(3):380-386.
- Kandzari DE, Rao SV, Moses JW, et al. Clinical and angiographic outcomes with sirolimus-eluting stents in total coronary occlusions: the ACROSS/TOSCA-4 (approaches to chronic occlusions with sirolimus-eluting stents/total occlusion study of coronary arteries-4) trial. JACC Cardiovasc Interv. 2009;2(2):97-106.
- Stone GW, Ellis SG, Cannon L, et al. Comparison of a polymer-based paclitaxel-eluting stent with a bare-metal stent in patients with complex coronary artery disease: a randomized controlled trial. JAMA. 2005;294(10):1215-1223.
- Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with st-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update): a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation. 2009;120(22):2271-2306.
- Lee SW, Park SW, Kim YH, et al. Drug-eluting stenting followed by cilostazol treatment reduces late restenosis in patients with diabetes mellitus the DECLARE-DIABETES trial (a randomized comparison of triple antiplatelet therapy with dual antiplatelet therapy after drug-eluting stent implantation in diabetic patients). J Am Coll Cardiol. 2008;51(12):1181-1187.
___________________________________________
From the 1Department of Cardiology, Nagoya Daini Red Cross Hospital, Nagoya, Japan, and the 2Cardiovascular Research Center, Mount Sinai School of Medicine, New York, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted January 2, 2012, provisional acceptance given January 17, 2012, final version accepted January 25, 2012.
Address for correspondence: Kiyotake Ishikawa, MD, Cardiovascular Research Center, Mount Sinai School of Medicine, One Gustave L. Levy Place, Box 1030, New York, NY 10029-6574. Email: kiyotake1@hotmail.com










