

Microcoil Embolization in Post-Traumatic High-Flow Priapism
ABSTRACT: An 18-year-old male developed post-traumatic priapism subsequent to a fall causing blunt perineal trauma. Color Doppler ultrasound showed a high-flow arterio-venous fistula with feeders from branches of the left internal iliac artery. Selective arteriography of the left internal pudendal artery demonstrated an arterio-venous fistula. A curved-tip 2.3 French microcatheter (Terumo Medical Corporation, Tokyo, Japan) was advanced proximal to the fistula over a 0.014˝ flexible guidewire. The fistula was then embolized with 2 platinum 18-2-2 Hilal Embolization Microcoils (Cook, Bloomington, Indiana). Improvement was noted, with closure of the fistula at check angiography and significant detumescence on table. This was later confirmed on repeat color Doppler imaging. At follow-up 6 and 12 weeks later, he had normal erectile function. Transarterial embolization appears to be a safe and effective treatment for managing patients with high-flow priapism.
J INVASIVE CARDIOL 2011;23:E147–E149
Key words: microcoil embolization, priapism
__________________________________________
High-flow priapism is a nonsexual, persistent erection caused by unregulated cavernous arterial inflow.1–3 Typically, the penis is neither fully rigid nor painful in this condition, and trauma is the most commonly reported etiology resulting in cavernosal artery disruption. Treatment of high-flow priapism is not an emergency, as oxygen supply to the corpora cavernosae is maintained; hence, patients are at a low risk of permanent complications. The pathophysiology resembles that of compartment syndrome, with blood bypassing the capillary system completely and flowing directly into the lacunar spaces leading to persistent penile tumescence. Conservative therapy, such as penile cooling, compression of penile artery and application of vasoconstrictors, is almost always without long-term benefit.4 Surgical treatments are invasive and may also prove ineffective; furthermore, they may be complicated by secondary erectile dysfunction or gangrene.1,2 Transarterial embolization using small-caliber coaxial catheters offers the ability to selectively occlude the fistula without damage to adjacent healthy tissue.3,5–7
The current literature offers only a handful of case reports describing the use of microcoils in the treatment of high-flow priapism.5–7 We report a case of post-traumatic high-flow priapism that underwent successful metallic microcoil embolization.
 Case Report. An 18-year-old army recruit developed painless sustained incomplete erection after blunt perineal trauma subsequent to a fall in a ditch while practicing a jump. Color Doppler ultrasound (detailed report missing at the time of publication) showed high peak systolic velocity of flow and high forward diastolic flow, suggesting an arterio-venous (AV) fistula with feeders from the branches of the left internal iliac artery. He was subsequently subjected to angiography under local anesthesia, the right femoral artery was punctured, and
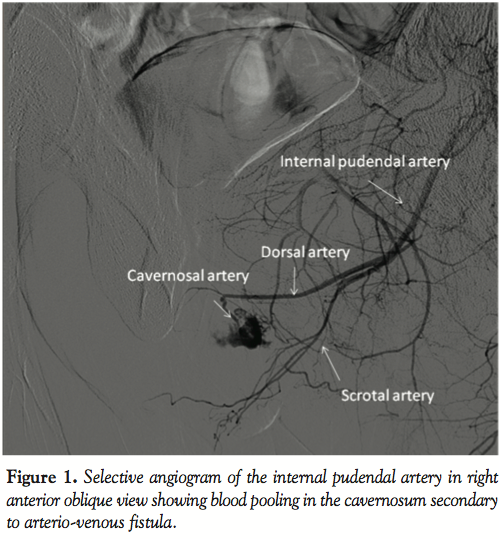
Case Report. An 18-year-old army recruit developed painless sustained incomplete erection after blunt perineal trauma subsequent to a fall in a ditch while practicing a jump. Color Doppler ultrasound (detailed report missing at the time of publication) showed high peak systolic velocity of flow and high forward diastolic flow, suggesting an arterio-venous (AV) fistula with feeders from the branches of the left internal iliac artery. He was subsequently subjected to angiography under local anesthesia, the right femoral artery was punctured, and  a 5 French (Fr) cobra catheter (Cordis Endovascular, Warren, New Jersey) was introduced through a 6 Fr sheath. The left internal pudendal artery was selectively catheterized; using hand injection of contrast medium, the arterio-venous fistula was identified arising from the cavernosal artery (Figure 1). A curved-tip, 2.3 Fr microcatheter (Terumo Medical Corporation, Tokyo, Japan) was advanced coaxially proximal to the fistula over a 0.014˝ flexible Cougar guidewire (Medtronic Endovascular, Santa Rosa, California). The defect was occluded using two platinum coils 0.018˝ in diameter, 2 cm in length and 2 mm in diameter (18-2.0-2 HILAL embolization microcoils, Cook, Bloomington, Indiana) (Figure 2). Improvement was noted with closure of the fistula at check angiography and significant detumescence on table. He was kept in the hospital for 48 hours observation after the procedure and was monitored with repeat color Doppler ultrasound, which showed complete closure of the AV fistula. At 6- and 12-week follow-up, he had normal erectile function.
a 5 French (Fr) cobra catheter (Cordis Endovascular, Warren, New Jersey) was introduced through a 6 Fr sheath. The left internal pudendal artery was selectively catheterized; using hand injection of contrast medium, the arterio-venous fistula was identified arising from the cavernosal artery (Figure 1). A curved-tip, 2.3 Fr microcatheter (Terumo Medical Corporation, Tokyo, Japan) was advanced coaxially proximal to the fistula over a 0.014˝ flexible Cougar guidewire (Medtronic Endovascular, Santa Rosa, California). The defect was occluded using two platinum coils 0.018˝ in diameter, 2 cm in length and 2 mm in diameter (18-2.0-2 HILAL embolization microcoils, Cook, Bloomington, Indiana) (Figure 2). Improvement was noted with closure of the fistula at check angiography and significant detumescence on table. He was kept in the hospital for 48 hours observation after the procedure and was monitored with repeat color Doppler ultrasound, which showed complete closure of the AV fistula. At 6- and 12-week follow-up, he had normal erectile function.
Discussion. Management of traumatic priapism remains a challenging clinical problem. The traditional recommendation of high-flow priapism is observation, long-term resolution rates being up to 62% in reported cases.1,2 Both conservative methods and surgery are associated with a high risk of erectile dysfunction.1,2 Conservative treatments include penile cooling, repeat puncture of corpora cavernosa with blood aspiration and injection of alpha-adrenergic agonist or methylene blue.1 These conservative measures have not been found successful in treating high-flow priapism. Intracavernosal pharmacotherapy usually fails because of rapid wash-out of the agent by the high-flow state or because the injured artery does not constrict enough to stop flow through the fistula. The advantages of interventional therapy lie in its minimally invasive nature; fistulae can be sealed without damage to surrounding healthy tissue or nerves. The recovery is much faster, with less morbidity and shorter hospitalization times.3,5–7
The diagnosis in most cases is established using color Doppler ultrasound, which is as sensitive as pudendal artery angiography, but a little less specific.8 Color Doppler also plays an important role in post-embolization follow-up. If no patent fistula is visualized on color Doppler study, the patient’s prognosis is good despite the possibility of persisting tumescence, which may resolve within a few days.4
 Embolization of the deep artery of the penis (cavernosal artery) is the treatment of choice.1 The goal of superselective arterial embolization therapy is to temporarily interrupt the arterial blood flow feeding the fistula for enough time to allow the injury site to heal without permanently jeopardizing penile erectile function. Embolization can be done using either resorbable (blood clot and gel foam) or non-resorbable (coils or microballoons) material. The majority of priapism cases reported in the literature have been done using resorbable material (Table 1). Overall success rates with embolization are high, with very few complications (Table 1). Single treatment with resorbable material carries a recurrence rate of 20–30%; in contrast, microcoils are more effective and permanent, with negligible recurrence rates.9 In addition, microcoils have the advantage that they can be placed exactly into the branch supplying the arteriocavernosal fistula. Theoretically, microcoils increase the risk of permanent vascular occlusion and subsequent erectile dysfunction. However, this is less common in younger individuals and those who undergo unilateral embolization as a result of infusion from the contralateral artery.2 Studies published to date with a follow-up in the range of 1–60 months have shown a very low incidence of erectile dysfunction (Table 1). This is not surprising because of the potential for collateral formation from the contralateral cavernosal artery, dorsal penile artery, and external pudendal artery. While defects rarely occur bilaterally, successful outcomes have also been reported with bilateral superselective coil embolizations.9–12
Embolization of the deep artery of the penis (cavernosal artery) is the treatment of choice.1 The goal of superselective arterial embolization therapy is to temporarily interrupt the arterial blood flow feeding the fistula for enough time to allow the injury site to heal without permanently jeopardizing penile erectile function. Embolization can be done using either resorbable (blood clot and gel foam) or non-resorbable (coils or microballoons) material. The majority of priapism cases reported in the literature have been done using resorbable material (Table 1). Overall success rates with embolization are high, with very few complications (Table 1). Single treatment with resorbable material carries a recurrence rate of 20–30%; in contrast, microcoils are more effective and permanent, with negligible recurrence rates.9 In addition, microcoils have the advantage that they can be placed exactly into the branch supplying the arteriocavernosal fistula. Theoretically, microcoils increase the risk of permanent vascular occlusion and subsequent erectile dysfunction. However, this is less common in younger individuals and those who undergo unilateral embolization as a result of infusion from the contralateral artery.2 Studies published to date with a follow-up in the range of 1–60 months have shown a very low incidence of erectile dysfunction (Table 1). This is not surprising because of the potential for collateral formation from the contralateral cavernosal artery, dorsal penile artery, and external pudendal artery. While defects rarely occur bilaterally, successful outcomes have also been reported with bilateral superselective coil embolizations.9–12
Patients in whom embolization fails must undergo surgery. There are two surgical approaches — extracorporeal and transcorporeal; both techniques carry the risk of impotence in up to 50% of cases.9 Recently, androgen blockade has been reported in the treatment of high-flow priapism, using leuprolide with or without ketaconazole and bicalutamide, with encouraging results.13
In summary, high-flow post-traumatic priapism is a rare condition and is usually due to trauma. It can be elegantly managed by superselective transarterial embolization of the cavernosal artery as a safe and effective treatment with minimal morbidity and preservation of potency.
References
- Broderick GA, Kadioglu A, Bivalacqua TJ, et al. Priapism: Pathogenesis, epidemiology, and management. J Sex Med 2010;7:476–500.
- Huang YC, Harraz AM, Shindel AW, Lue TF. Evaluation and management of priapism: 2009 update. Nat Rev Urol 2009;6:262–267.
- Kim KR, Shin JH, Song HY, et al. Treatment of high-flow priapism with superselective transcatheter embolization in 27 patients: A multicenter study. J Vasc Interv Radiol 2007;18:1222–1226.
- Ilkay A, Levine L. Conservative management of high-flow priapism. Urology 1995;46:419–424.
- Callewaert P, Stockx L, Bogaert G, Baert L. Post-traumatic high-flow priapism in a 6-year-old boy: Management by percutaneous placement of bilateral vascular coils. Urology 1998;52:134–137.
- Mathias K, Jager H, Witkowski M, et al. High-flow priapism following blunt perineal trauma: Interventional therapy. Radiologe 1998;38:710–713.
- Liu B, Xin Z, Zou Y, et al. High flow priapism: Super selective cavernous artery embolization with microcoils. Urology 2008;72:571–574.
- Bertolotto M, Quaia E, Mucelli FP, et al. Color Doppler imaging of post-traumatic priapism before and after selective embolization. Radiographics 2003;23:495–503.
- Montague DK, Jarow J, Broderick GA, et al. Members of the Erectile Dysfunction Guideline Update Panel; Americal Urological Association. J Urol 2003;170(4 Pt. 1):1318–1324.
- Sandlera G, Chennapragadaa SM, Soundappana SSV, Cassa D. Pediatric high-flow priapism and super-selective angiography — An Australian perspective. J Pediatr Surg 2008;43:1898–1901.
- Görich J, Ermis C, Krämer SC, et al. Interventional treatment of traumatic priapism. J Endovasc Ther 2002;9:614–617.
- Lee YC, Shen JT, Shih MC, et al. Bilateral superselective arterial microcoil embolization in post-traumatic high-flow priapism: A case report. Kaohsiung J Med Sci 2003;19:79–83.
- Mwamukonda KB, Chi T, Shindel AW, Lue TF. Androgen blockade for the treatment of high-flow priapism. J Sex Med 2010;7:2532–2537.
_____________________________________
From 1the Division of Cardiology, Command Hospital, Bangalore, Karnataka, India, 2the Division of Radiology, Command Hospital, Udhampur, Jammu and Kashmir, India, and 3the Division of Urology, Command Hospital, Pune, Maharashtra, India.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 1, 2010, provisional acceptance given July 1, 2010, final version accepted October 27, 2010.
Address for correspondence: Davinder S. Chadha, MD, DM, Department of Cardiology, Command Hospital, Bangalore, Karnataka 560017 India. Email: agiamu@gmail.com


