

Mid-Term Outcomes of Alcohol Septal Ablation for Obstructive Hypertrophic Cardiomyopathy in Patients With Sigmoid Versus Neutral Ventricular Septum
Abstract: Background. The aim of this study was to determine whether the differences in the baseline septal morphology influenced outcomes of patients after alcohol septal ablation (ASA). Methods. A total of 100 consecutive, highly symptomatic patients with HOCM and a neutral or sigmoid septum (74 patients vs 26 patients) underwent ASA and were examined clinically and echocardiographically at baseline and at follow-up (median 30 months vs 24 months). Results. At baseline, a neutral septum morphology was associated with a thicker basal septum [21 (19-24) mm vs 19 (18-20) mm; P<0.01] and higher pressure gradient at rest [59 (39-80) mm vs 43 (33-50) mm; P<0.01], but a similar pressure gradient after provocation [100 (72-120) mmHg vs 97 (70-110) mmHg; P=0.31], and subsequently both resting gradient [10 (10-16) mmHg vs 12 (10-15) mmHg; P=0.67] and provoked gradient after ASA [20 (10-30) mmHg vs 18 (12-25) mmHg; P=0.71]. Four patients died during follow-up (4% vs 4%; NS). Pressure gradient, septum thickness and symptoms decreased significantly in both groups. Conclusions. Patients treated with ASA who had a sigmoid septum were characterized at baseline by a thinner basal septum and lower pressure gradient at rest. However, they showed an identical pressure gradient after provocation and subsequently after ASA. ASA was safe and effective in both groups of patients.
J INVASIVE CARDIOL 2012;24(12):636-640
Key words: ablation, obstruction, hypertrophic cardiomyopathy, sigmoid septum
_________________________________________________________
Hypertrophic cardiomyopathy (HCM) is defined as a primary myocardial hypertrophy in the absence of another causative condition, often with a dynamic left ventricular outflow tract (LVOT) obstruction and a diastolic dysfunction of the left ventricle (LV).1 Patients diagnosed with HCM in their fifth decade or later tend to have a morphological subtype characterized as a sigmoid ventricular septum (SS), which is also referred to as a septal bulge, septal knuckle or upper septal hypertrophy.2 It has been suggested that the SS is associated with less symptoms and occurrence of sudden cardiac death.1,3 Therefore, some authors speculate that HCM in the elderly may stem from a fundamentally distinct disease process and this clinical manifestation might be a variant or forme fruste of HCM.3 Interestingly, most of these patients suffer from significant LV obstruction (hypertrophic obstructive cardiomyopathy – HOCM) and require its elimination.3
Alcohol septal ablation (ASA) is an accepted alternative to surgical myectomy in the treatment of highly symptomatic patients with HOCM.1 The aim of this study was to determine whether the differences in the baseline septal morphology (neutral vs sigmoid) influenced outcomes of patients after ASA.
Methods
Study population. Clinical, interventional and echocardiographic data were obtained prospectively as part of an ongoing institutional database of HCM patients. Written informed consent was obtained from each patient and the local ethics committee approved all study protocols. A total of 100 consecutive patients with sigmoid or neutral septum ablated for HOCM were selected from approximately 200 patients evaluated for ASA.
Clinical and echocardiographic evaluation. Patients with symptomatic HOCM (New York Heart Association class ≥III) and neutral (Group 1) or sigmoid (Group 2) septal morphology receiving maximum medical therapy were consecutively enrolled between January 2000 and December 2010. All patients had to have a basal septal thickness >15 mm and maximal LVOT pressure gradient >30 mmHg at rest or >50 mmHg under provocation (application of isosorbide dinitrate in sublingual form).1,4 Echocardiographic data were acquired and analyzed by a single investigator. The LVOT pressure gradient was derived using the modified Bernoulli’s equation. All pressure gradients provided in this study were maximum gradients measured by continuous Doppler echocardiography. Septal wall thickness was maximum thickness measured in the basal segment of the septum (IVS) and the thinnest basal septal IVS diameter at follow-up. LV end-diastolic diameters were measured from 2-dimensional images as well as LV ejection fractions. All patients were followed-up for at least 12 months. Clinical and echocardiographic examinations were performed at baseline, 1 year after the procedure and at the end of follow-up.
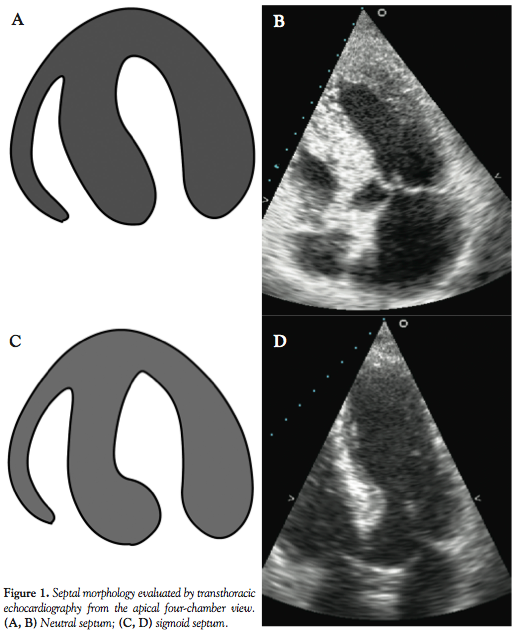 Definitions. The sigmoid septal morphology type was defined as generally an ovoid LV cavity with the protrusion of the left septal endocardium into the LVOT (basal septal bulge) and qualitatively determined at the most thickened area of the basal septum. Neutral septal morphology was defined as a generally straight or slightly convex septum toward the left ventricular cavity (Figures 1A-1D). Septal curvature and cavity contour was evaluated in the apical four-chamber view. Latent obstruction was defined as a resting pressure gradient ≤30 mmHg, which increased markedly after provocation (≥50 mmHg). Absolute delta pressure gradient was defined as follows: pressure gradient at baseline – pressure gradient at follow-up. Relative delta pressure gradient was defined as follows: (pressure gradient at baseline – pressure gradient at follow-up) / pressure gradient at baseline.
Definitions. The sigmoid septal morphology type was defined as generally an ovoid LV cavity with the protrusion of the left septal endocardium into the LVOT (basal septal bulge) and qualitatively determined at the most thickened area of the basal septum. Neutral septal morphology was defined as a generally straight or slightly convex septum toward the left ventricular cavity (Figures 1A-1D). Septal curvature and cavity contour was evaluated in the apical four-chamber view. Latent obstruction was defined as a resting pressure gradient ≤30 mmHg, which increased markedly after provocation (≥50 mmHg). Absolute delta pressure gradient was defined as follows: pressure gradient at baseline – pressure gradient at follow-up. Relative delta pressure gradient was defined as follows: (pressure gradient at baseline – pressure gradient at follow-up) / pressure gradient at baseline.
Alcohol septal ablation. Our myocardial contrast echocardiography guided-ASA technique has been previously published.5-7 Alcohol was injected very slowly in small fractions (0.5 ml/s) into suitable septal branches. Pressure gradient in the LVOT was measured invasively. A temporary pacemaker was placed for at least 24 hours, and all patients were observed in the coronary care unit for 24 to 72 hours. Subsequently, telemetric monitoring was used for the whole post-procedural week. Blood was withdrawn for the MB fraction of creatine kinase (CK-MB) at 6 hour intervals for 2 post-procedural days.
Statistical analysis. Microsoft Excel (Microsoft Corp.) with Analyze-It (Analyze-It Software) was used to create and analyze the study database. Normally distributed data are presented as mean and standard deviation (±SD) and non-normally distributed data as median with interquartile range (IQR). Distribution of data was evaluated by the Kolmogorov-Smirnov test. Student’s t test, Fischer´s test and Mann-Whitney´s U test and Pearson´s correlation test were used when appropriate. Significance was defined by a P value <0.05.
Results
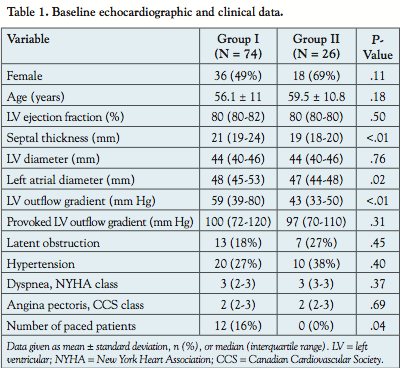 Acute results. The baseline characteristics of both groups are summarized in Table 1. In a total of 100 patients (74 patients with a neutral septum and 26 patients with an SS), alcohol was injected into 115 septal branches. There were no differences in alcohol injection volumes (1.7±0.7 ml vs 1.6±0.7 ml; NS). The peak of CK-MB was 2.4±0.8 µkat/L vs 2.2±0.7 µkat/L (NS), with the normal range of CK-MB being up to 0.42 µkat/L. There was a significant correlation between basal IVS thickness and age at baseline (r=-0.28; P<0.01), but not after the post-procedural LV remodeling (NS).
Acute results. The baseline characteristics of both groups are summarized in Table 1. In a total of 100 patients (74 patients with a neutral septum and 26 patients with an SS), alcohol was injected into 115 septal branches. There were no differences in alcohol injection volumes (1.7±0.7 ml vs 1.6±0.7 ml; NS). The peak of CK-MB was 2.4±0.8 µkat/L vs 2.2±0.7 µkat/L (NS), with the normal range of CK-MB being up to 0.42 µkat/L. There was a significant correlation between basal IVS thickness and age at baseline (r=-0.28; P<0.01), but not after the post-procedural LV remodeling (NS).
 ASA was combined with percutaneous coronary intervention in 4 patients (5% vs 0%; NS). No ASA procedure resulted in an early post-procedural death. Peri-procedural ventricular tachycardia requiring electrical cardioversion occurred in 3 patients (4% vs 0%; NS), and complete heart block in 7 patients (8% vs 8%; NS), which subsequently resulted in an implantation of 3 permanent pacemakers (4% vs 0%; NS). Post-procedural right bundle branch block was present in 58 patients (53% vs 73%; P=0.04). Most patients were discharged 7 days after the intervention. No patient died during hospital stay.
ASA was combined with percutaneous coronary intervention in 4 patients (5% vs 0%; NS). No ASA procedure resulted in an early post-procedural death. Peri-procedural ventricular tachycardia requiring electrical cardioversion occurred in 3 patients (4% vs 0%; NS), and complete heart block in 7 patients (8% vs 8%; NS), which subsequently resulted in an implantation of 3 permanent pacemakers (4% vs 0%; NS). Post-procedural right bundle branch block was present in 58 patients (53% vs 73%; P=0.04). Most patients were discharged 7 days after the intervention. No patient died during hospital stay.
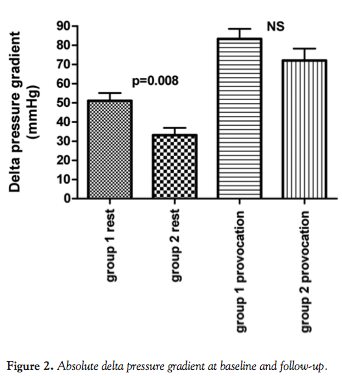 Follow-up. The mean follow-up of the whole cohort was 44±36 months. There was no difference in the length of follow-up (median 30 months vs 24 months; NS). Four patients died during follow-up (4% vs 4%; NS). The outcomes of patients are summarized in Tables 2 and 3. Although there was a significant difference between absolute delta pressure gradient at rest between groups 1 and 2, we did not find significant differences in relative delta pressure gradients between both groups (Figures 2 and 3).
Follow-up. The mean follow-up of the whole cohort was 44±36 months. There was no difference in the length of follow-up (median 30 months vs 24 months; NS). Four patients died during follow-up (4% vs 4%; NS). The outcomes of patients are summarized in Tables 2 and 3. Although there was a significant difference between absolute delta pressure gradient at rest between groups 1 and 2, we did not find significant differences in relative delta pressure gradients between both groups (Figures 2 and 3).

Cardioverter-defibrillator (ICD) was implanted in 7 patients in the neutral septum group based on pre-procedural sudden death risk stratification (9% vs 0%; NS). None of these implantations were required because of worsening ventricular arrhythmias following ASA.
Repeated procedures were necessary in 4 patients (4% vs. 4%; NS); one patient (1%) was later sent for surgical myectomy. None of the patients reported a further deterioration of symptoms. All symptomatic patients remained on beta-blockers or calcium channel blockers.
Discussion
In this study we demonstrated that patients treated with ASA who had a sigmoid septum were characterized by a thinner basal septum at baseline and a lower pressure gradient at rest, but they showed an identical pressure gradient after provocation and subsequently after ASA. Both groups of patients responded to ASA significantly with a marked hemodynamic and clinical improvement during mid-term follow-up.
The phenotypic features of HCM may develop at any age from infancy to adulthood, and are characterized by a great heterogeneity in the extent and distribution of LV hypertrophy.1,3 Generally, older patients with HCM tend to suffer from late-onset LV hypertrophy, characteristically showing an SS and ovoid LV cavity associated with a relatively milder degree of hypertrophy and better prognosis.1,2 Similar to previous findings, we demonstrated an inverse relationship between age and maximum basal septum thickness in both groups of our patients (r=-0.28; P<0.01),8,9 which might explain previously published findings demonstrating a faster LVOT pressure gradient decrease in the early post-procedural phase in older patients.10,11 In addition to a lower septum thickness resulting in a faster post-procedural outflow gradient relief, some authors speculate that the aorto-septal angle (typically ≤100 degrees) might characterize the development of LVOT obstruction in older patients.12,13
It has been suggested that morphological subtypes of LV hypertrophy, namely a sigmoid, neutral and catenoid septum, have implications for the likelihood of detecting myofilament mutation and clinical prognosis. As demonstrated by Binder et al, there was a positive finding in one or more of the eight myofilament-encoding genes in only 8% of the patients with an SS.3 Moreover, this finding was independent of the diagnosis of coexisting hypertension. Also, there were no significant differences in the prevalence of hypertension in both groups in this study. Therefore, it is highly probable that an SS stems from a process pathophysiologically different to HCM that is based primarily on myofilament mutations. However, ASA seemed to be similarly effective in treating both groups of HCM patients.
The therapeutic aim of ASA is widening the obstructed LVOT. It is achieved by immediate myocardial necrosis and stunning, and subsequently by the induction of LV remodeling with thinning of the basal IVS.14 Although both groups of patients had different shapes of IVS, the catheterization technique used in all the patients was identical and post-procedural creatine kinase release was similar. Theoretically, alcohol volume and the number of ablated branches could be lower in the SS group because of the lower amount of myocardium that is needed to be affected. However, this speculation has to be justified by further studies.
Importantly, there was no difference in early post-procedural complications between both groups except for the occurrence of a right bundle branch block (RBBB), which was more frequent in the SS group (53% vs 73%; P=0.04). On the other hand, such a high occurrence of RBBB has not been presented in unselective ASA populations up to now,14-17 which might suggest a higher risk of ASA-associated RBBB in SS patients.
A major long-term concern with ASA is the potentially increased risk of ventricular arrhythmias and sudden death.18 Despite the median of follow-up being only 24 and 30 months, respectively, for the two groups, which did not allow any generalization, post-procedural long-term mortality rates seemed to be close to 1% per year and there was no difference in the need for repeat procedures or myectomy. Seven patients (9%) in the neutral septum group required a subsequent implantation of ICD; however, all these implantations were based on risk stratification that was performed prior to the ASA. Although the difference between both groups did not reach statistical difference, this finding might suggest a higher risk of sudden death in patients with a neutral septum compared to an SS. It is likely that patients with a neutral septum suffer from a “more advanced” form of HCM, which is illustrated by the younger age at diagnosis, greater LV mass associated with a higher risk of sudden death and a higher prevalence and extent of myocardial fibrosis.19
The present findings might have the following implications for clinical cardiologists: first, also patients with an SS should not be echocardiographically examined only at rest, but the stress should be put on provocation with nitrates or physical exercise; second, the hemodynamic and clinical benefit of ASA in these patients is similar to those with a neutral septum, although the persisting dyspnea is significantly worse in the SS group; and third, except for the higher occurrence of RBBB in the SS group, ASA was identically safe in both groups of patients and there were no significant differences in post-procedural follow-up.
Limitations. This study has several limitations. The study cohort was evaluated and treated at a single referral center and therefore, patient characteristics do not reflect the general population of patients with obstructive HCM. Clinically stable or older patients might be underpresented in this cohort. In addition, the small size of this study does not allow any generalization of the demonstrated findings; however, some differences between the two groups of patients are suggestive and supported by previous observations. Specifically, a more pronounced septum thickness, a resting pressure gradient, a lower age at the time of the ASA procedure and a higher rate of implanted ICDs reflect a higher risk profile for neutral septum patients. Another limitation of the present study is the qualitative assessment of the IVS shape. Furthermore, septal morphologies were classified using images available at the time of enrollment into the study database. On the other hand, it is unlikely that an individual’s septal anatomy will change markedly over time. However, this inherent limitation has always been associated with the classification of LV morphologies in HCM patients.3,19
Conclusion
In this study, HOCM patients treated with ASA and with a sigmoid septum compared to a neutral one were characterized by a thinner basal septum at baseline and a lower pressure gradient at rest. However, they showed an identical pressure gradient after provocation and subsequently after ASA. Both groups of patients responded to ASA significantly with a marked hemodynamic and clinical improvement during mid-term follow-up.
Acknowledgments. The authors thank Eva Hansvenclova for the assistance in data analysis.
References
- Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy. J Am Coll Cardiol. 2011;58(25):e212-e260.
- Ranasinghe I, Yeoh T, Yiannikas J. Negative inotropic agents for the treatment of left ventricular outflow tract obstruction due to sigmoid septum and concentric left ventricular hypertrophy. Heart Lung Circ. 2011;20(9):579-586.
- Binder J, Ommen SR, Gersh BJ, et al. Echocardiography-guided genetic testing in hypertrophic cardiomyopathy: septal morphological features predict the presence of myofilament mutations. Mayo Clin Proc. 2006;81(4):459-467.
- Zemánek D, Tomašov P, Homolová S, Linhartová K, Veselka J. Sublingual isosorbide dinitrate for the detection of obstruction in hypertrophic cardiomyopathy. Eur J Echocardiogr. 2011;12(9):684-687.
- Veselka J, Zemánek D, Tomašov P, Duchonová R, Linhartová K. Alcohol septal ablation for obstructive hypertrophic cardiomyopathy: ultra-low dose of alcohol (1 ml) is still effective. Heart Vessels. 2009;24(1):27-31.
- Veselka J, Zemánek D, Fiedler J, Šváb P. Real-time myocardial contrast echocardiography for echo-guided alcohol septal ablation. Arch Med Sci. 2009;5:271-272.
- Veselka J, Duchonová R, Procházková Š, et al. Effects of varying ethanol dosing in percutaneous septal ablation for obstructive hypertrophic cardiomyopathy on early hemodynamic changes. Am J Cardiol. 2005;95(5):675-678.
- Maron BJ, Casey SA, Hurrell DG, Aeppli DM. Relation of left ventricular thickness to age and gender in hypertrophic cardiomyopathy. Am J Cardiol. 2003;91(10):1195-1198.
- Thaman R, Gimeno JR, Reith S, et al. Progressive left ventricular remodeling in patients with hypertrophic cardiomyopathy and severe left ventricular hypertrophy. J Am Coll Cardiol. 2004;44(2):398-405.
- Gietzen FH, Leuner CJ, Obergassel L, Strunk-Muller C, Kuhn H. Transcoronary ablation of septal hypertrophy for hypertrophic obstructive cardiomyopathy: feasibility, clinical benefit, and short term results in elderly patients. Heart. 2004;90(6):638-644.
- Veselka J. Duchonová R, Pálenícková J, et al. Age-related hemodynamic and morphologic differences in patients undergoing alcohol septal ablation for hypertrophic obstructive cardiomyopathy. Circ J. 2006;70(7):880-884.
- Bolca O, Ozer N, Eren M, et al. Dobutamine induced dynamic left ventricular outflow tract obstruction in patients with hypertrophic nonobstructive cardiomyopathy. Tohoku J Exp Med. 2002;198(2):79-87.
- Goor D, Lillehei CW, Edwards JE. The “sigmoid septum”: variation in the contour of the left ventricle. Am J Roentgenol Radium Ther Nucl Med. 1969;107(2):366-376.
- Veselka J. Alcohol septal ablation for hypertrophic obstructive cardiomyopathy: a review of the literature. Med Sci Monit. 2007;13(4):RA62-RA8.
- Rigopoulos AG, Seggewiss H. A decade of percutaneous septal ablation in hypertrophic cardiomyopathy. Circ J. 2011;75(1):28-37.
- Faber L, Welge D, Fassbender D, et al. Percutaneous septal ablation for symptomatic hypertrophic obstructive cardiomyopathy: managing the risk of procedure-related AV conduction disturbances. Int J Cardiol. 2007;119(2):163-167.
- Lawrenz T, Obergassel L, Lieder F, et al. Transcoronary ablation of septal hypertrophy does not alter ICD intervention rates in high risk patients with hypertrophic obstructive cardiomyopathy. Pacing Clin Electrophysiol. 2005;28(4):295-300.
- Kuhn H, Lawrenz T, Lieder F, et al. Survival after transcoronary ablation of septal hypertrophy in hypertrophic obstructive cardiomyopathy (TASH): a 10 year experience. Clin Res Cardiol. 2008;97(4):234-243.
- Turer AT, Samad Z, Valente AM, et al. Anatomic and clinical correlates of septal morphology in hypertrophic cardiomyopathy. Eur J Echocardiogr. 2011;12(2):131-139.
_____________________________________________________________
From the Department of Cardiology, 2nd Medical School, Charles University and University Hospital Motol, Czech Republic.
Funding: Supported by the project (Ministry of Health, Czech Republic) for conceptual development of research organization 00064203 (University Hospital Motol, Prague, Czech Republic)
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 18, 2012, provisional acceptance given May 11, 2012, final version accepted May 29, 2012.
Address for correspondence: Prof. J. Veselka, MD, PhD, Dept. of Cardiology, University Hospital Motol, V uvalu 84, Prague 5, 15000, Czech Republic. Email: josef.veselka@fnmotol.cz












