

Minimalist Management of Occlusive Spontaneous Coronary Artery Dissection With Workhorse Guidewire: The Prick-and-Wait Technique
J INVASIVE CARDIOL 2021;33(5):E405. doi:10.25270/jic/20.00241
Key words: cardiac imaging, complications, coronary artery dissection
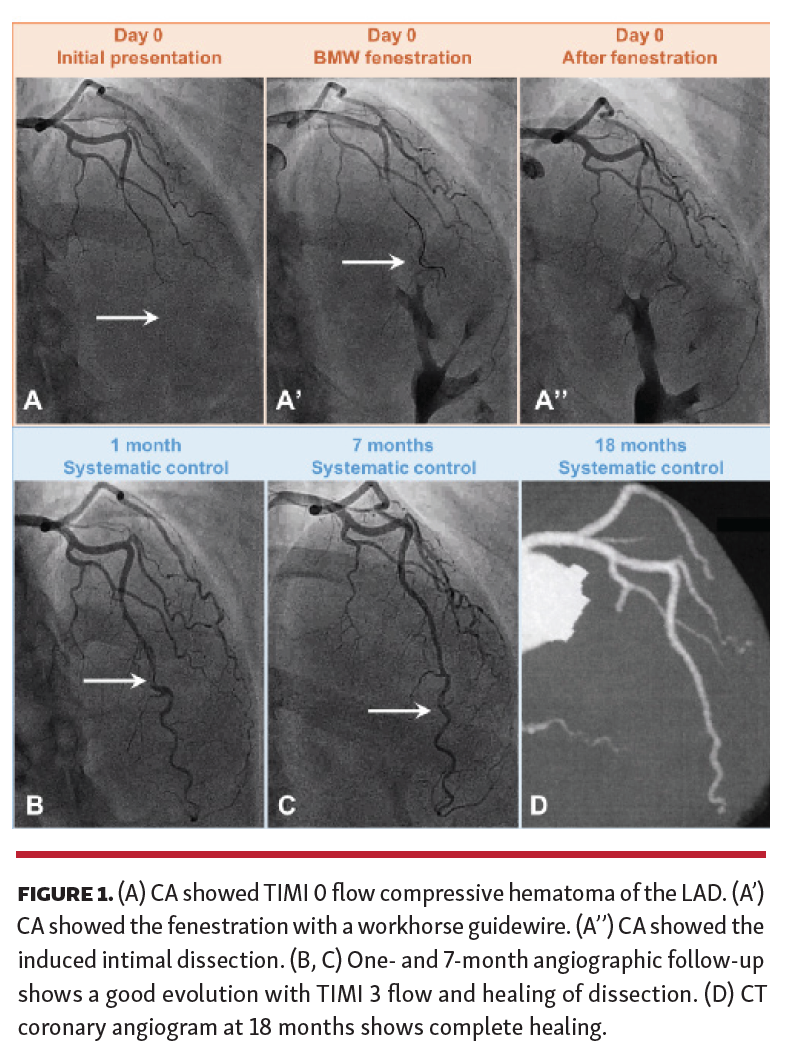
A 42-year-old female with persistent 24-hour chest pain, anterior ST-segment elevation, and apical akinesia underwent a coronary angiography (CA). Intramural hematoma was found with Thrombolysis in Myocardial Infarction (TIMI) 0 flow in the mid left anterior descending (LAD) coronary artery, starting on a septal branch (Figure 1A).
A Workhorse BMW guidewire (Abbott Vascular) (Figure 1A') was chosen to follow the vessel architecture. Several attempts to cross the occlusion failed to reach the distal lumen, but created fenestrations (Figure 1A'), transforming the hematoma into dissection.
The final result of TIMI 2 flow was angiographically partially successful, but due to the disappearance of pain, normalization of the ST-segment, and the impossibility of reaching the distal lumen, the procedure was stopped.
The patient became asymptomatic. CA controls showed TIMI 3 flow and healing of the dissection at 1 and 7 months (Figures 1B and 1C). Echocardiographies, single-photon emission computerized tomography scan at 12 months, and computed tomography scan at 18 months (Figure 1D) showed complete recovery.
This could be a bailout strategy in the event of (1) failure to reach the distal true lumen; (2) slight improvement in the distal flow, but allowing clinical resolution of ST-segment elevation myocardial infarction; and (3) a situation not suited to surgery. Here, this “prick-and-wait” technique led to a complete recovery only with a BMW guidewire and time.
From the 1Cardiology Department, Felix-Guyon University Hospital, Saint-Denis, France; and 2Cardiology Department, Gabriel-Montpied University Hospital, Clermont-Ferrand, France.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted May 7, 2020.
Address for correspondence: Louis-Marie Desroche, MD, CHU, Felix-Guyon, Allée des Topazes, 97400 Saint-Denis France. Email: louis-marie.desroche@chu-reunion.fr









