

Multimodality Imaging To Diagnose Pulmonary Vein Stenosis Following Atrial Fibrillation Ablation
ABSTRACT: Atrial fibrillation (AF) is increasing in prevalence. Although experienced centers performing radiofrequency pulmonary vein isolation procedures have reported success rates approaching 72%, in rare instances it is complicated by stenosis of one or more pulmonary veins. In this report we present a case of recurrent pulmonary vein stenosis (PVS) following radiofrequency ablation for AF.
J INVASIVE CARDIOL 2011;23:E214–E215
Key words: Pulmonary vein stenosis, lung perfusion scanning, paroxysmal atrial fibrillation
_________________________________
Atrial fibrillation (AF) is increasing in prevalence.1 Although experienced centers performing radiofrequency pulmonary vein isolation procedures have reported success rates of 75% to 87%,2,3 in rare instances it is complicated by stenosis of one or more pulmonary veins. In this report we present a case of pulmonary vein stenosis (PVS) following radiofrequency ablation for atrial fibrillation.
 Case Report. A 66-year-old man underwent radiofrequency pulmonary vein isolation for paroxysmal atrial fibrillation. A wide area of circumferential radiofrequency ablation encircling the right and left pulmonary veins (PV) was performed using real time intracardiac echocardiogram guidance. He was continued on oral anticoagulation with warfarin after the procedure. Eight months following the procedure, he presented with mildly decreased exercise tolerance despite sustained normal sinus rhythm. Transthoracic echocardiogram revealed normal systolic and diastolic function, and myocardial perfusion imaging revealed no perfusion abnormality.
Case Report. A 66-year-old man underwent radiofrequency pulmonary vein isolation for paroxysmal atrial fibrillation. A wide area of circumferential radiofrequency ablation encircling the right and left pulmonary veins (PV) was performed using real time intracardiac echocardiogram guidance. He was continued on oral anticoagulation with warfarin after the procedure. Eight months following the procedure, he presented with mildly decreased exercise tolerance despite sustained normal sinus rhythm. Transthoracic echocardiogram revealed normal systolic and diastolic function, and myocardial perfusion imaging revealed no perfusion abnormality.
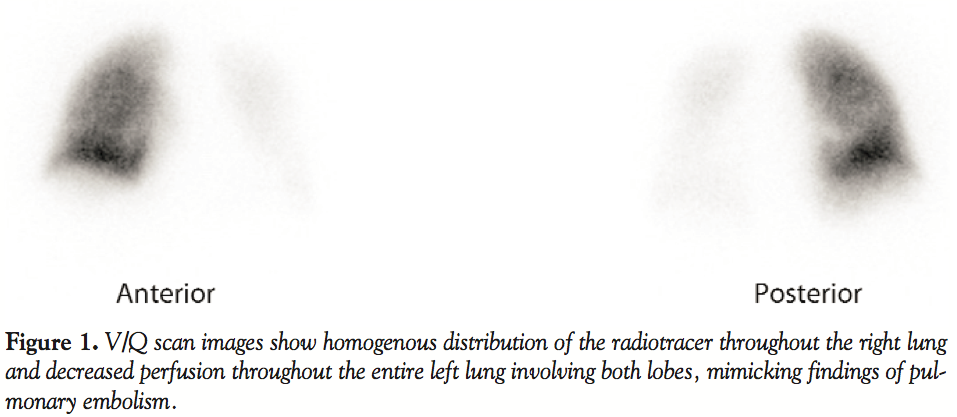
![]() Nuclear ventilation perfusion scan (V/Q) showed decreased perfusion throughout the entire left lung mimicking profound pulmonary embolism (Figure 1). CT angiography revealed severe stenosis of the left superior pulmonary vein and complete occlusion of the left inferior pulmonary vein. The patient was subsequently brought to the catheterization laboratory where pulmonary angiography confirmed the above findings. Percutaneous balloon angioplasty and stenting of the left superior and inferior pulmonary veins was performed using 2 bare metal balloon expandable Palmaz Genesis™ stents (Cordis, Johnson & Johnson) (Figure 2). The patient was subsequently started on aspirin and clopidogrel. Repeat V/Q scan 2 months after the procedure revealed significant improvement in the previously noted global hypoperfusion within the left lung (Figure 3). The patient described complete resolution of his symptoms.
Nuclear ventilation perfusion scan (V/Q) showed decreased perfusion throughout the entire left lung mimicking profound pulmonary embolism (Figure 1). CT angiography revealed severe stenosis of the left superior pulmonary vein and complete occlusion of the left inferior pulmonary vein. The patient was subsequently brought to the catheterization laboratory where pulmonary angiography confirmed the above findings. Percutaneous balloon angioplasty and stenting of the left superior and inferior pulmonary veins was performed using 2 bare metal balloon expandable Palmaz Genesis™ stents (Cordis, Johnson & Johnson) (Figure 2). The patient was subsequently started on aspirin and clopidogrel. Repeat V/Q scan 2 months after the procedure revealed significant improvement in the previously noted global hypoperfusion within the left lung (Figure 3). The patient described complete resolution of his symptoms.
Discussion. Stenosis of one or more pulmonary veins following radiofrequency pulmonary vein isolation has been reported in 1–3% of cases4 and the incidence of complete pulmonary vein occlusion in 0.3% to 1.3%.5 The mechanism is thought to be periadventitial inflammation and collagen deposition.6 The presentation and clinical course of PVS varies widely from asymptomatic in two-thirds of cases to mild to severe dyspnea in a third of cases.7 Symptoms seem to correlate with the number of the stenotic veins, the severity of the stenosis, the time course of the stenosis, compensatory mechanisms and development of collaterals where the more severe stenosis and the more stenosed veins result in more symptoms.4 Patients with single-vessel occlusion are mostly asymptomatic, while involvement of other ipsilateral veins involves more symptoms. The left superior PV has the greatest incidence of total occlusion (54.2%), followed by the left inferior PV (29.2%), right inferior PV (8.3%) and right superior PV (8.3%).5 Symptoms present 2–5 months after the procedure. Late diagnosis is common and likely related to the nonspecific nature of the symptoms. PVS may be commonly misdiagnosed as pulmonary embolism, bronchitis, pneumonia, asthma, and lung cancer. It is common for patients with PVS to receive multiple unnecessary interventions including bronchoscopy, thoracentesis of pleural effusions, inferior vena caval filters, and partial lung resection or antibiotic treatment for pneumonia.5
Pulmonary vein angiography is the gold standard for diagnosis of pulmonary vein stenosis or occlusion.8 Pulmonary vein stenosis can be assessed noninvasively by using anatomical and functional imaging using computed topography, magnetic resonance imaging, transesophageal echo, or lung perfusion scanning.
Lung perfusion scanning is of particular value in the diagnosis of iatrogenic PVS. The sudden occlusion of a pulmonary vein is soon followed by gradual decline and then cessation of arterial flow to the affected segment due to increased resistance in the pulmonary vascular bed.4,5 Perfusion defects are observed when the degree of stenosis is greater than 65%, resulting in at least 25% reduction in perfusion of the affected lung segment.4,9 This degree of perfusion defect correlates with severity of symptoms.4,9 Lung perfusion scan is less operator- and technique-dependent and is associated with less radiation exposure compared to CT angiography.10
It appears that lung perfusion scanning is an effective tool in the diagnosis and follow-up of patients with iatrogenic PVS. In this case segmental perfusion defects on V/Q scan correlated well with the anatomical location of the stenosis and severity of occlusion of the pulmonary veins.
References
- Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gender of patients with atrial fibrillation. Analysis and implications. Arch Intern Med. 1995;155(5):469-473.
- Piccini JP, Lopes RD, Kong MH, et al. Pulmonary vein isolation for the maintenance of sinus rhythm in patients with atrial fibrillation: a meta-analysis of randomized, controlled trials. Circ Arrhythm Electrophysiol. 2009;2(6):626-633.
- Calkins H, Brugada J, Packer DL, et al. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: Recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); In collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace. 2007;9(6):335-379.
- Holmes DR Jr, Monahan KH, Packer D. Pulmonary vein stenosis complicating ablation for atrial fibrillation: clinical spectrum and interventional considerations. JACC Cardiovasc Interv. 2009;2(4):267-276.
- Di Biase L, Fahmy TS, Wazni OM, et al. Pulmonary vein total occlusion following catheter ablation for atrial fibrillation: clinical implications after long-term follow-up. J Am Coll Cardiol 2006;48(12):2493-2499.
- Taylor GW, Kay GN, Zheng X, Bishop S, Ideker RE. Pathological effects of extensive radiofrequency energy applications in the pulmonary veins in dogs. Circulation. 2000;101(14):1736-1742.
- Saad EB, Rossillo A, Saad CP, et al. Pulmonary vein stenosis after radiofrequency ablation of atrial fibrillation: functional characterization, evolution, and influence of the ablation strategy. Circulation. 2003;108(25):3102-3107.
- Prieto LR, Kawai Y, Worley SE. Total pulmonary vein occlusion complicating pulmonary vein isolation: diagnosis and treatment. Heart Rhythm. 2010;7(9):1233-1239.
- Barrett CD, Di Biase L, Natale A. How to identify and treat patient with pulmonary vein stenosis post atrial fibrillation ablation. Curr Opin Cardiol. 2009;24(1):42-49.
- Freeman LM, Stein EG, Sprayregen S, et al. The current and continuing important role of ventilation-perfusion scintigraphy in evaluating patients with suspected pulmonary embolism. Semin Nucl Med. 2008;38(6):432-440.
_________________________________
From the Department of Medicine, George Washington University, Washington, D.C.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. No authors reported conflicts regarding the content herein.
Manuscript submitted December 13, 2011, provisional acceptance given December 21, 2011, final version accepted February 8, 2011.
Address for correspondence: Amr Mohsen, MD, George Washington University Medical Center, Department of Medicine, 2150 Pennsylvania Avenue, NW, Ambulatory Care Center, Suite 5 – 411, Washington, DC, 20037. Email: mohsen@gwu.edu











