

New Ventricular Septal Defects Following Balloon-Expandable Transcatheter Aortic Valve Replacement
Abstract: Transcatheter aortic valve replacement (TAVR) has been commercially approved in the United States for the treatment of high-risk and inoperable patients with severe symptomatic aortic stenosis. While TAVR has proven benefits with regard to survival and quality of life in studied populations, the procedure is also associated with several well-described complications including stroke, vascular injury, and paravalvular regurgitation. More infrequent complications are less well described. Here, we report the development of new ventricular septal defects after TAVR in 4 patients with left ventricular outflow tract calcification. We discuss imaging and post-TAVR management of these patients.
J INVASIVE CARDIOL 2016;28(7):E59-E65
Key words: transcatheter aortic valve replacement, VSD
Transcatheter aortic valve replacement (TAVR) is a proven alternative to surgical aortic valve replacement for patients with symptomatic severe calcific aortic stenosis (AS) who are deemed high or extreme risk for traditional surgery.1-4 While TAVR has proven benefits with regard to survival and quality of life in this population, the procedure is also associated with several well-described complications including stroke, vascular injury, paravalvular regurgitation, and conduction disturbances.5 The infrequently encountered complication of ventricular septal defect (VSD) after TAVR is less well described, and the mechanism, risk factors, and treatment of this complication are not well characterized. In this series, we report 4 cases of VSD following balloon-expandable (BE)-TAVR among 1048 consecutive patients who underwent BE-TAVR and self-expanding (SE)-TAVR at our institution.
Case Presentations
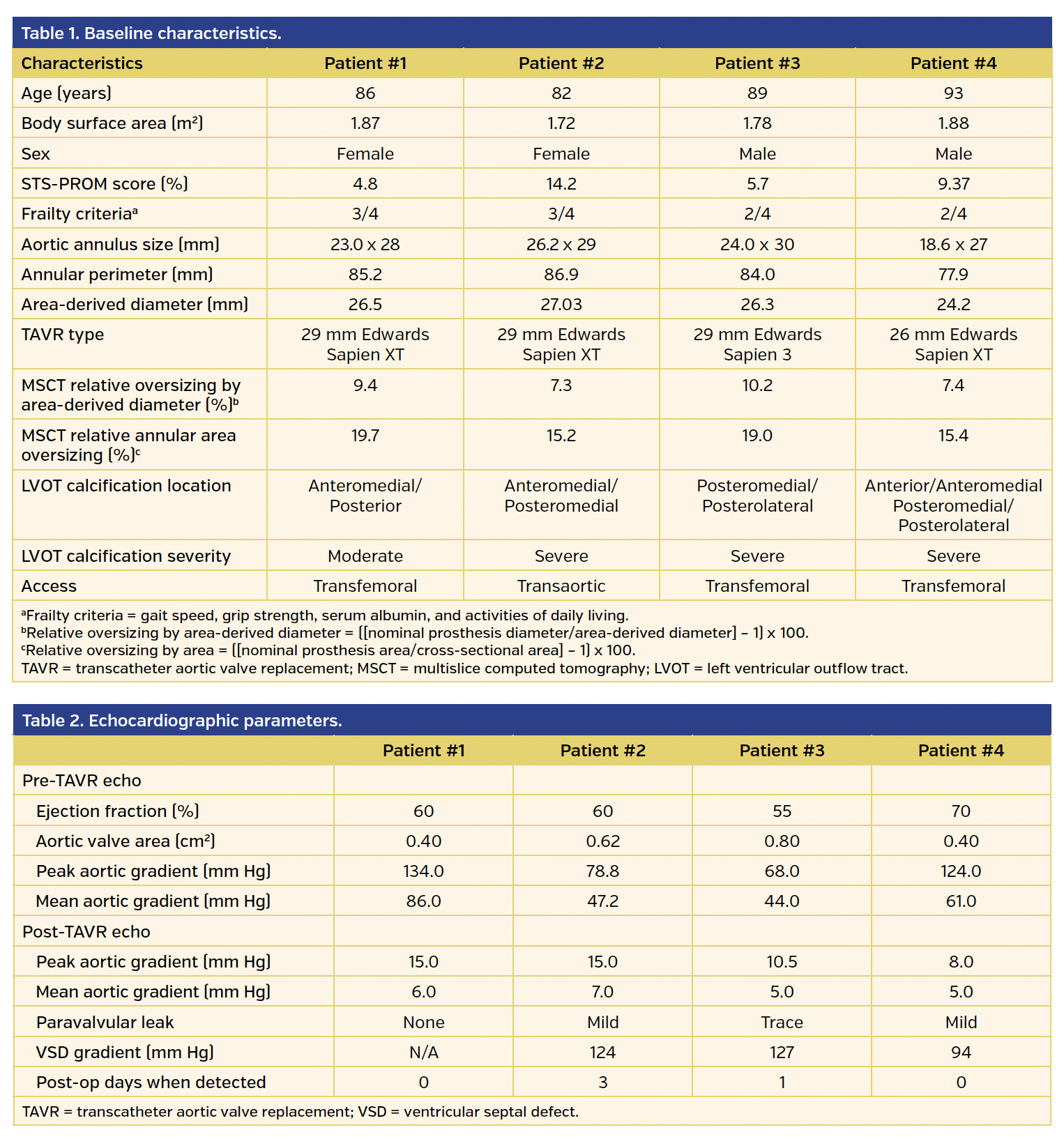
Patient #1. An 86-year-old woman with very severe AS presented to our institution with complaints of lightheadedness and reduction in exercise tolerance. Past medical history included hypertension, stage III chronic kidney disease, chronic obstructive pulmonary disease (COPD), and ankylosing spondylitis. Transthoracic echocardiogram (TTE) revealed left ventricular (LV) ejection fraction of 60% with peak and mean gradients across the aortic valve of 134 and 86 mm Hg, respectively. Aortic valve area (AVA) was calculated as 0.4 cm2. Cardiac catheterization revealed no evidence of obstructive coronary artery disease (CAD). Multislice computed tomography (MSCT) scan with angiography showed a heavily calcified mitral annulus, heavily calcified aortic valve, and atherosclerotic calcifications throughout the aorta and its distal branches, but otherwise patent femoral vessels. Aortic annulus minor and major diameters were 25 x 29 mm, with an area of 552 mm2. Area-derived diameter and perimeter were 26.9 and 85.2 mm, respectively. Oversizing by CT-derived aortic annular area was estimated at 19.7% (Table 1). Moderate anteromedial and posterior left ventricular outflow tract (LVOT) calcification can be seen in Figure 1. Although her STS score was calculated at 4.8%, given that she met three of four criteria for frailty,6 the heart valve team deemed her a more suitable candidate for TAVR.
The patient underwent successful deployment of a 29 mm Sapien XT valve (Edwards Lifesciences) prepared according to standard protocol via a transfemoral approach. Intraoperative transesophageal echocardiography (TEE) showed no paravalvular leak, but a small color Doppler jet from the LV to the right ventricle (RV) originating from below the aortic annulus, which was also confirmed on ventriculography. TTE performed 3 days postoperatively showed peak and mean gradient of 15 mm Hg and 7 mm Hg, respectively, across the prosthetic valve, an aortic root to RV communication, as well as a defect between the LVOT and the RV consistent with an iatrogenic VSD. No paravalvular aortic regurgitation (PAR) was detected. No new conduction abnormalities were noted on electrocardiogram (ECG). She was asymptomatic at the time of discharge.
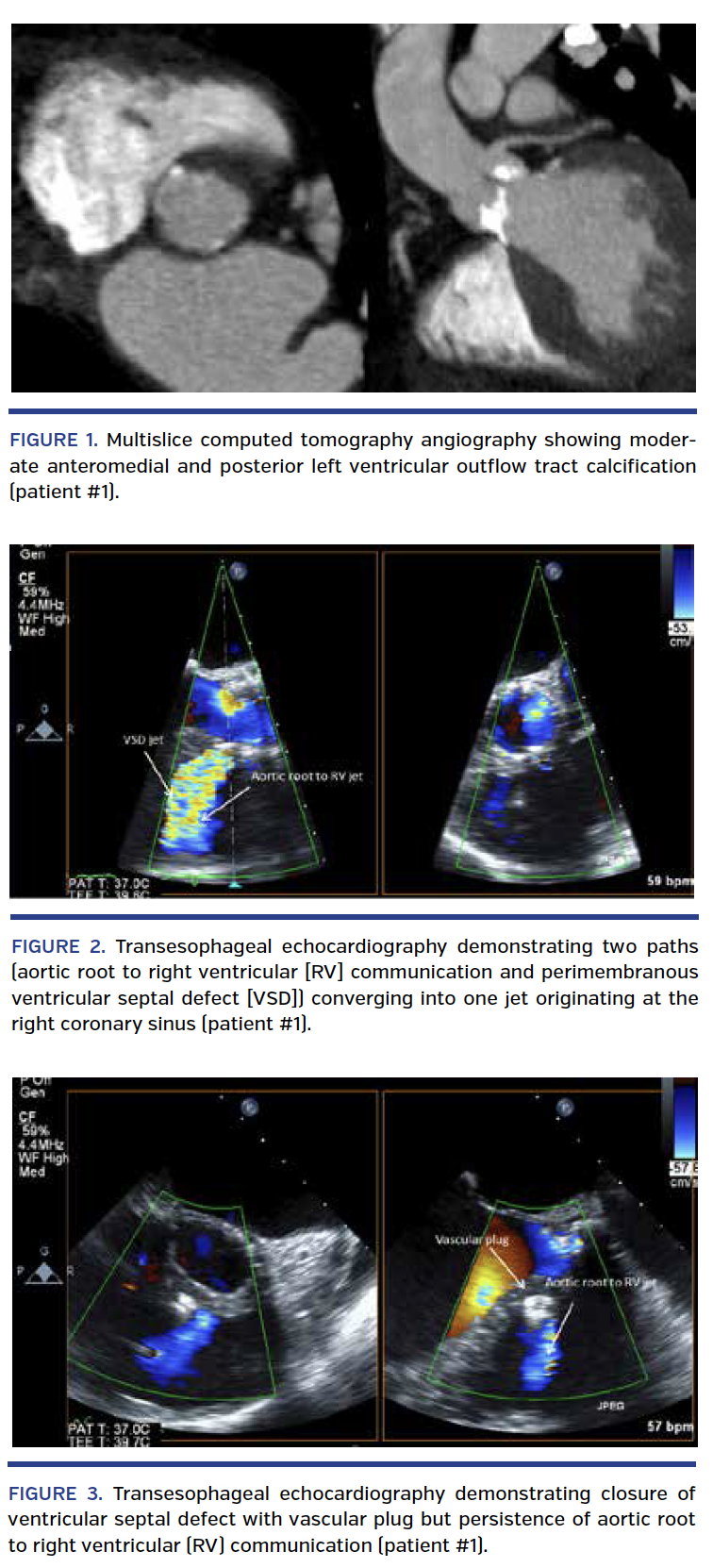
The patient was initially managed conservatively, but she reported significant peripheral edema and persistent dyspnea on exertion at her 1-month follow-up visit. She underwent repeat TEE, which confirmed a moderate-sized fistula from the aortic root to the RV (larger defect) and a perimembranous VSD. Their two paths can be seen converging into one jet originating at the right coronary sinus (Figure 2; Video 1). Repeat cardiac catheterization confirmed left-to-right shunting from the aortic root and LVOT into the RV (Video 2). Pulmonary artery pressures increased from 31/6 mm Hg prior to the TAVR procedure to 65/27 mm Hg at follow-up. Qp/Qs was noted to be 2.3. Given her clinical decompensation and change in hemodynamics, it was decided that percutaneous closure of both defects would be attempted.
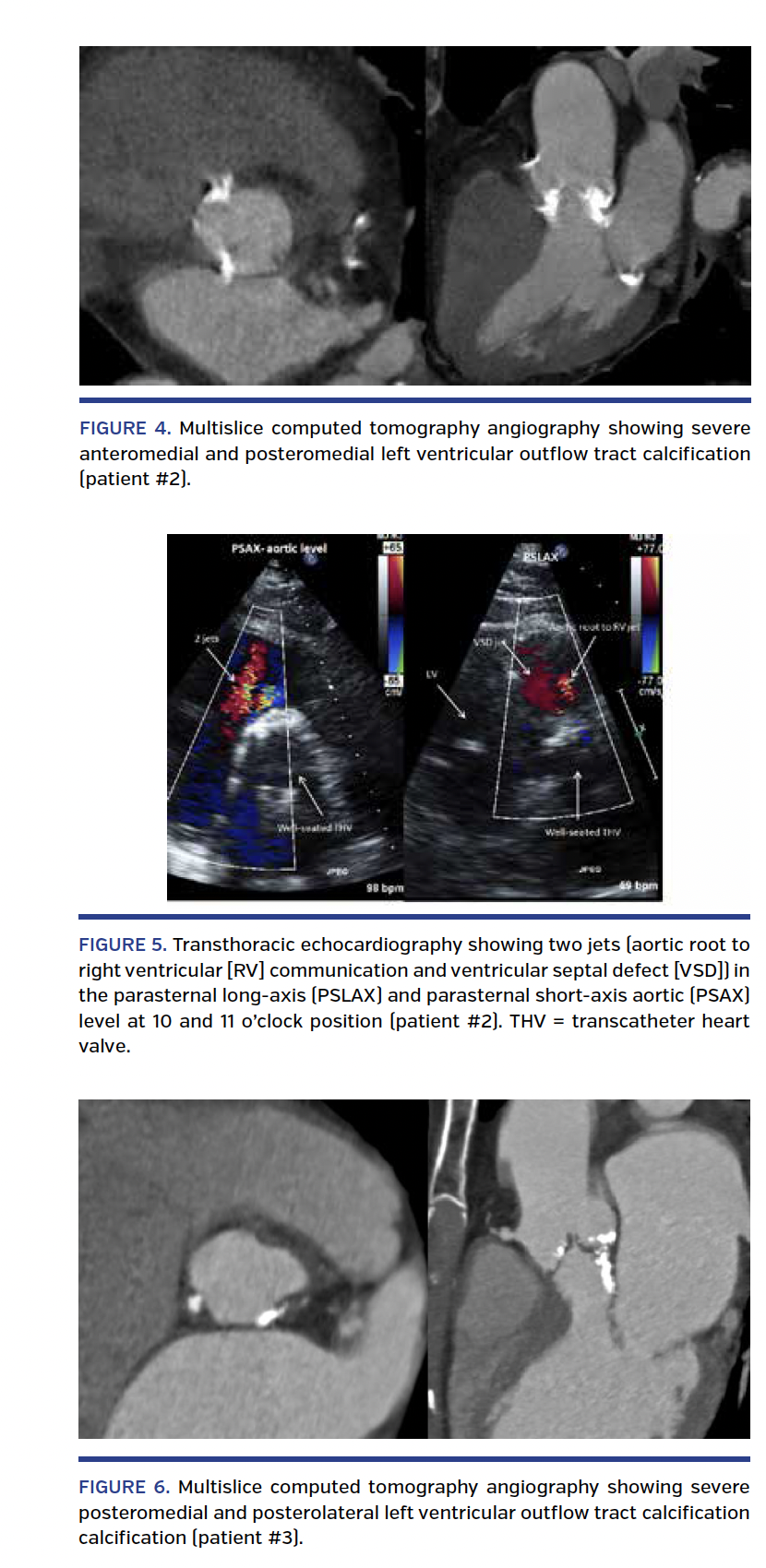
Closure of both defects was attempted under general anesthesia using TEE and angiographic guidance. VSD closure was performed using an 8 mm-diameter Amplatzer vascular plug 2 (St. Jude Medical) via an anterograde arteriovenous loop technique. An attempt to cross the aortic root to RV defect was unsuccessful, with persistence of significant shunting across the fistula (Figure 3; Video 3). She was seen 2 months after the partial closure and felt improved (New York Heart Association [NYHA] class II-III), but still had significant residual lower-extremity edema. Repeated TTE showed a residual gradient of 94 mm Hg across the aortic root to RV fistula. The patient died 4 months after her partial closure from complications associated with enterococcus bacteremia of an unclear source at a different institution. TEE performed prior to her death showed a well-functioning TAVR with mild PAR without evidence of vegetation.
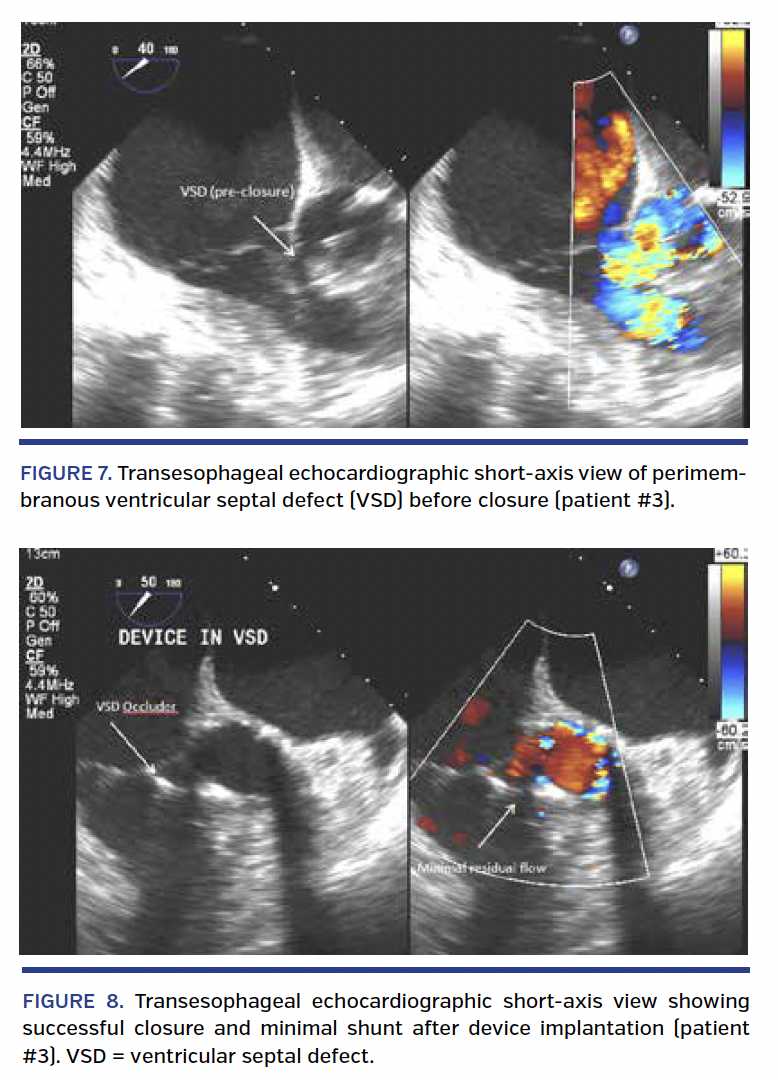
Patient #2. An 82-year-old woman with severe AS presented with symptoms of angina and significant dyspnea on exertion. Her past medical history included CAD, atrial fibrillation, oxygen-dependent COPD, and previous abdominal aortic aneurysm repair. TTE revealed an LV ejection fraction of 60% with peak and mean systolic gradient across the aortic valve of 79 mm Hg and 47 mm Hg, respectively. AVA was calculated at 0.62 cm2. Cardiac catheterization revealed non-obstructive coronary disease in all three vessels. MSCT angiography showed diffuse atherosclerosis throughout the thoracic aorta with dense calcification as well as severe calcification and tortuosity of both iliac and femoral vessels. Aortic annulus minor and major diameters were measured at 26.2 x 29.0 mm with an area of 574 mm2. Perimeter was 86.9 mm and area-derived diameter was 27.03 mm. Oversizing by CT-derived aortic annular area was estimated at 15.2% (Table 1). Severe anteromedial and posteromedial LVOT calcification can be seen on MSCT (Figure 4). Her STS predicted risk of mortality (PROM) score was 14.2%.
The patient underwent successful delivery of a 29 mm Sapien XT (prepared according to standard protocol) via a transaortic approach. Repeat angiography initially revealed mild-moderate PAR, also confirmed by TEE. A second balloon inflation was performed with an additional 2 cc in the balloon. Final angiography revealed mild PAR (Video 4). Following the procedure, she developed complete heart block and required permanent pacemaker placement.
Repeat TTE performed 3 days postoperatively showed mild PAR and a communication from the anterior aspect of the aortic root into the RV, as well as a perimembranous VSD seen at the 10 and 11 o’clock position on the parasternal short-axis view (Figure 5; Videos 5-7). The peak gradient across the VSD by TTE was estimated at 124 mm Hg. Peak and mean gradients across the aortic valve prosthesis were normal (Table 2). Based on the lack of symptoms, the decision was made to manage her conservatively. She died from pneumonia-related septic shock 1 month after her TAVR procedure at an outside hospital. Unfortunately, due to the limited amount of clinical information, we’re unable to establish a connection between her VSD and this event.
Patient #3. An 89-year-old man with severe AS presented with symptoms of chest pressure on exertion.7 His past medical history included atrial fibrillation, moderate mitral regurgitation, myelodysplastic syndrome, and gastric lymphoma status post radiation and chemotherapy 5 years prior to presentation. TTE showed an LV ejection fraction of 55%, as well as peak and mean systolic gradients across the aortic valve of 68 mm Hg and 44 mm Hg, respectively. AVA was calculated at 0.8 cm2. MSCT angiography demonstrated severe posteromedial and severe posterolateral LVOT calcification (Figure 6). Aortic annulus minor and major diameters measured at 24 x 30 mm, with an area of 546 mm2. Area-derived diameter was 26.3 mm and perimeter was 84 mm. Oversizing by CT-derived aortic annular area was estimated at 19%. The STS-PROM score was 5.7%, and he was enrolled in the PARTNER Sapien 3 intermediate-risk study.
The patient underwent successful deployment of a 29 mm Sapien S3 valve via a transfemoral approach. There were no intraoperative complications. Repeat angiography and intraoperative TEE showed no significant paravalvular leak. The VSD was not detected at the time of the procedure. Following the procedure, he was noted to be in complete heart block for which he underwent permanent pacemaker implantation. TTE performed the following day revealed a perimembranous VSD with an estimated peak gradient of 127 mm Hg. Peak and mean gradients across the aortic valve prosthesis were noted to be 10.5 mm Hg and 5 mm Hg, respectively. There was trivial anterior and posterior PAR.
The patient was initially managed conservatively, but was subsequently readmitted with progressive heart failure symptoms 1 month after his TAVR procedure. Repeat TTE showed worsening LV systolic function with estimated LV ejection fraction of 35%-40%. TEE showed normally functioning TAVR with moderate-sized left to right shunt with flow from the LVOT to the RV consistent with a VSD (Figure 7; Video 8). Cardiac catheterization revealed a Qp/Qs of 1.6 with an estimated left-to-right shunt flow of 3.8 L/min. Pulmonary artery pressures were 45/13 mm Hg with a mean of 28 mm Hg, which were unchanged from his prior measurements. Given clinical decompensation and significant left-to-right shunt, it was decided to proceed with percutaneous closure of the VSD as previously reported.7
Closure of the VSD was performed under general anesthesia using TEE and angiographic guidance with a 10-mm diameter Amplatzer VSD occluder (St. Jude Medical, Inc) via an anterograde arteriovenous loop technique. Following deployment of the device, there was significant decrease in color flow across the VSD with residual mild shunt (Figure 8; Video 9). At his 1-month follow-up visit after VSD closure, the patient reported significant improvement in exertional dyspnea (NYHA class II). He was last seen in clinic 14 months after the VSD closure and has remained in NYHA class II clinically. Repeat TTE showed a mildly reduced LV ejection fraction of 45%, without any residual VSD.
Patient #4. A 93-year-old man with very severe AS presented with complaints of progressive dyspnea with minimal exertion. His past medical history was notable for paroxysmal atrial fibrillation, heart failure with preserved ejection fraction, hypertension, chronic kidney disease, deep vein thrombosis, and myeloproliferative disorder. TTE showed an LV ejection fraction of 70% with peak and mean systolic gradients of 124 mm Hg and 61 mm Hg, respectively. AVA was calculated at 0.4 cm2. Coronary angiography revealed no obstructive CAD. Aortic annulus major and minor diameters measured at 27 x 18.6 mm, with an area of 460 mm2 on MSCT angiography. Area-derived diameter was 24.2 mm, and perimeter was 77.9 mm. Oversizing by CT-derived aortic annular area was estimated at 15.4% (Table 1). MSCT angiography demonstrated severe anterior, anteromedial, posteromedial, and posterolateral LVOT calcification (Figure 9). STS score was 9.37%.
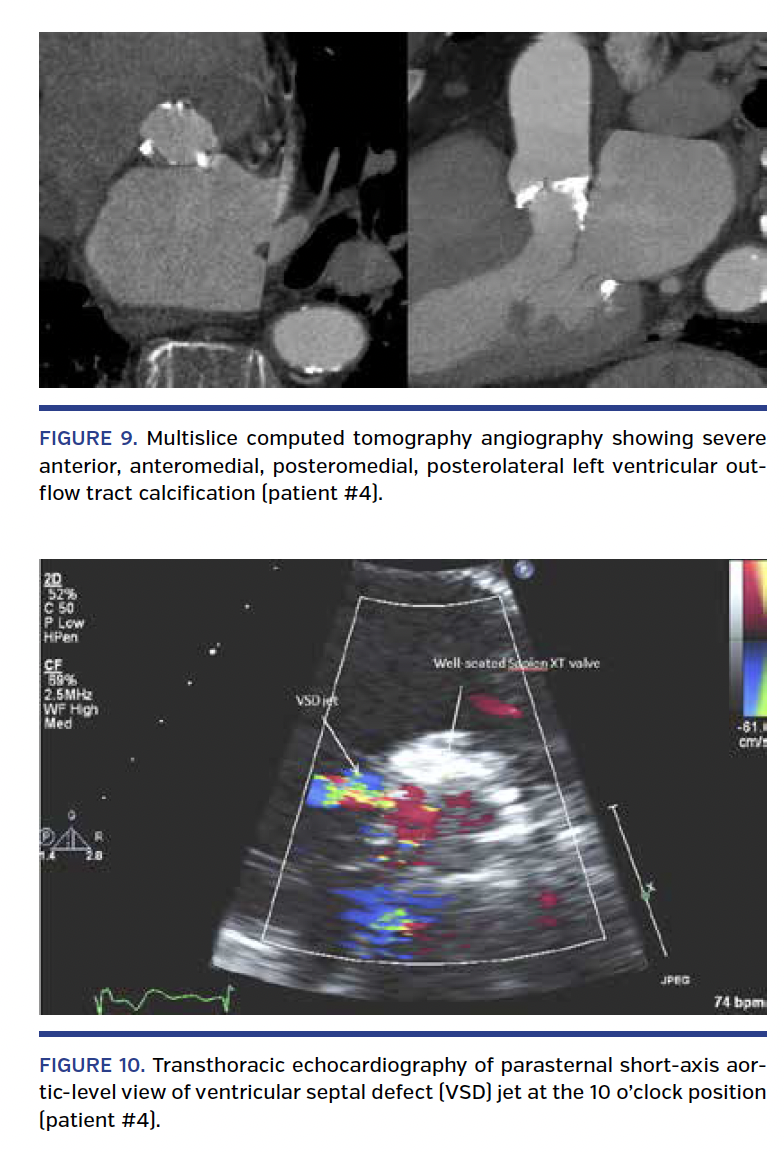
He underwent successful deployment of a 26 mm Sapien XT valve (prepared according to standard protocol) via a transfemoral approach. There were no intraoperative complications. Repeat angiography showed trace to mild PAR. Postoperative TTE demonstrated mild PAR along the basal anteroseptum and the aorto-mitral continuity and a left to right shunt from the LVOT into the RV and a gradient of 94 mm Hg consistent with a restrictive perimembranous VSD seen at the 10 o’clock position in the parasternal short-axis view (Figure 10; Videos 10 and 11). No new conduction abnormalities were noted on ECG. Given the lack of symptoms at that time, he was managed conservatively. He was seen in clinic at 1-month follow-up and continued to be asymptomatic.
Discussion
Post-TAVR VSDs are an uncommon but potentially clinically significant complication. Prompt recognition and careful assessment of these defects using both hemodynamic and echocardiographic measures are necessary to guide management decisions. As delineated in 2 out of 4 cases, clinical deterioration can occur in a delayed fashion, including several weeks following the initial procedure. As such, close clinical follow-up should be maintained.
To date, there have been 1048 TAVRs performed at our institution (932 BE and 116 SE). In this case series, we present 3 new cases and 1 previously reported case7 of perimembranous VSD post TAVR with an incidence of 0.4% for BE-TAVRs. Ten prior cases of post-TAVR VSD have been reported in the literature to date: 3 transapical TAVRs8-10 and 7 transfemoral TAVRs.11-15 One case series reported a post-TAVR VSD incidence of 4%.11 Of the reported cases, 8 were perimembranous VSDs11-15 and 2 were muscular VSDs.8,9 The two reported muscular VSDs were associated with transapical TAVRs. Two cases occurred with the CoreValve SE aortic bioprosthesis12,13 and 8 cases occurred with BE valves.8-11,14,15 In the 2 cases of VSD associated with the SE aortic bioprosthesis, balloon postdilation was used to treat the patient. In light of the predominant usage of BE valves at our institution, it is possible that we noted post-TAVR VSDs with BE valves simply due to selection bias. Whether perimembranous VSDs are more likely to occur than muscular VSDs with a retrograde approach (transfemoral, transaortic) remains to be determined.
In addition to developing VSDs, 2 of our patients also developed aortic root to RV fistulas. The timing and proximity of these lesions suggest that the traumatic mechanism responsible for the development of VSD post TAVR may be similar to that of aortic annular rupture. Nonetheless, it is unclear whether the risk factors are exactly the same for both lesions. A few reports have suggested that the risk of VSD post TAVR may be increased by postdilation of the prosthesis.12,13,16 Barbanti et al16 examined a series of patients who experienced LVOT/annular/aortic contained/non-contained rupture after BE-TAVR and found that moderate to severe LVOT calcification and annular area oversizing by >20% were associated with these complications. A study of 72 patients who underwent TAVR using an Edwards Sapien prosthesis noted that contained aortic root rupture was more common in patients with valve oversizing using MSCT, especially in patients with relative oversizing >20% of their annulus diameter.17
In our series, only 1 patient required postdilation for the treatment of residual PAR. In addition, we used recommended CT-derived annular area and perimeter for prosthesis sizing. The degree of oversizing in these cases was 17.3% on average (range, 15.2%-19.7%) by aortic annular area and 8.6% (range, 7.3%-9.4%) by diameter. No patient met the ≥20% oversizing threshold by annular area that had been previously identified as a possible risk factor for aortic root rupture.16,17 LVOT calcification was the only common denominator seen in all 4 patients that has been previously identified as a risk factor for aortic root rupture. In our series, all patients were noted to have moderate-severe medial LVOT calcification, with 3 out of 4 patients having LVOT calcification just underneath the right coronary cusp. While location of the LVOT calcification may play a role in predicting post-TAVR VSD, further study will be needed to clarify the exact mechanism by which LVOT calcification leads to damage of the perimembranous septum during BE-TAVR.
The transcatheter aortic valve size selected is ideally larger than the native annulus, resulting in annular oversizing to help reduce the risk of PAR.18,19 For the CoreValve device, the recommended ideal device/annulus oversizing is 15% of the aortic basal ring diameter. For the Edwards Sapien valve, the recommended device/annulus oversizing is 15%-25% of the area and 7%-12% of the mean diameter.18-21 This degree of oversizing of the transcatheter heart valve has been shown to provide the best risk-benefit ratio with regard to paravalvular and conduction disorders,18-21 but does not take into consideration the risk of other complications such as VSD or other mechanical complications. In our series, all of our patients developed VSD despite receiving BE heart valves that were within the recommended range of oversizing. It is possible that LVOT calcification may significantly increase the risk of post-TAVR complications even when adhering to the currently acceptable oversizing ranges.
Two of our patients with VSD post TAVR eventually became symptomatic. Whenever feasible, percutaneous closure of VSD should be considered the preferred option given the risk profile of these patients. In concordance with three previously described reports,10,13,15 our institutional experience confirms that closure of the VSD post TAVR can be successfully attempted using well-established percutaneous techniques under TEE guidance in the setting of a favorable anatomy, as seen in patient #3.7 Although the more commonly used devices for percutaneous VSD closure are the Amplatzer Cribiform septal occluder and the Amplatzer muscular VSD occluder, the Amplatzer vascular plug II device can also be used in an off-label manner for percutaneous closure of an LVOT to RV defect. Otherwise, in the setting of an unfavorable anatomy and rapid hemodynamic decompensation, an open surgical option may perhaps be best.22
As the number of TAVR procedures performed continues to increase, it is important to remain vigilant for less common complications such as VSD. Diagnosis should be made on the basis of clinical findings, hemodynamic assessment, and multimodality imaging. Percutaneous closure should be guided by degree of shunt and patient clinical characteristics. As demonstrated in 2 of our 4 cases, clinical deterioration can occur several weeks after diagnosis, necessitating close follow-up.
Conclusion
We describe 4 cases of a relatively uncommon complication of the TAVR procedure. While certain common features (medial LVOT calcification, annular area oversizing of 15%-20%) were present among patients with this complication, delineating definitive risk factors from this series remains speculative. Management of this complication must be individualized based on the clinical scenario and percutaneous closure remains a feasible treatment option in selected patients with favorable anatomy.
References
1. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597-1607.
2. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198.
3. Adams DH, Popma JJ, Reardon MJ. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;371:967-968.
4. Popma JJ, Adams DH, Reardon MJ, et al. Transcatheter aortic valve replacement using a self-expanding bioprosthesis in patients with severe aortic stenosis at extreme risk for surgery. J Am Coll Cardiol. 2014;63:1972-1981.
5. Genereux P, Head SJ, Van Mieghem NM, et al. Clinical outcomes after transcatheter aortic valve replacement using valve academic research consortium definitions: a weighted meta-analysis of 3,519 patients from 16 studies. J Am Coll Cardiol. 2012;59:2317-2326.
6. Green P, Woglom AE, Genereux P, et al. The impact of frailty status on survival after transcatheter aortic valve replacement in older adults with severe aortic stenosis: a single-center experience. JACC Cardiovasc Interv. 2012;5:974-981.
7. Mark SD, Prasanna V, Ferrari VA, Herrmann HC. Percutaneous ventricular septal defect closure after Sapien 3 transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2015;8:e109-e110. Epub 2015 May 20.
8. Al-Attar N, Ghodbane W, Himbert D, et al. Unexpected complications of transapical aortic valve implantation. Ann Thorac Surg. 2009;88:90-94.
9. Massabuau P, Dumonteil N, Berthoumieu P, et al. Left-to-right interventricular shunt as a late complication of transapical aortic valve implantation. JACC Cardiovasc Interv. 2011;4:710-712.
10. Levi DS, Salem M, Suh W. Transcatheter closure of an iatrogenic ventricular septal defect after Sapien valve implantation. Catheter Cardiovasc Interv. 2015;85:E90-E94. Epub 2014 May 7.
11. Patel Y, Vassileva C, Mishkel G. Rare complication of ventricular septal defect in three patients following transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2014;83:497-501.
12. Tzikas A, Schultz C, Piazza N, van Geuns RJ, Serruys PW, de Jaegere PP. Perforation of the membranous interventricular septum after transcatheter aortic valve implantation. Circ Cardiovasc Interv. 2009;2:582-583.
13. Gerckens U, Latsios G, Pizzulli L. Percutaneous treatment of a post-TAVI ventricular septal defect: a successful combined procedure for an unusual complication. Catheter Cardiovasc Interv. 2013;81:E274-E277.
14. Aminian A, Lalmand J, Dolatabadi D. Late contained aortic root rupture and ventricular septal defect after transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2013;81:E72-E75.
15. Mauri L, Aldebert P, Cuisset T, Quilici J, Fraisse A. Percutaneous closure of a poorly tolerated post-transcatheter aortic valve implantation ventricular septal defect. Ann Thorac Surg. 2014;98:1823-1826.
16. Barbanti M, Yang TH, Rodes Cabau J, et al. Anatomical and procedural features associated with aortic root rupture during balloon-expandable transcatheter aortic valve replacement. Circulation. 2013;128:244-253.
17. Blanke P, Reinohl J, Schlensak C, et al. Prosthesis oversizing in balloon-expandable transcatheter aortic valve implantation is associated with contained rupture of the aortic root. Circ Cardiovasc Interv. 2012;5:540-548.
18. Piazza N, de Jaegere P, Schultz C, Becker AE, Serruys PW, Anderson RH. Anatomy of the aortic valvar complex and its implications for transcatheter implantation of the aortic valve. Circ Cardiovasc Interv. 2008;1:74-81.
19. Athappan G, Patvardhan E, Tuzcu EM, et al. Incidence, predictors, and outcomes of aortic regurgitation after transcatheter aortic valve replacement: meta-analysis and systematic review of literature. J Am Coll Cardiol. 2013;61:1585-1595.
20. Kasel AM, Cassese S, Bleiziffer S, et al. Standardized imaging for aortic annular sizing: implications for transcatheter valve selection. JACC Cardiovasc Imaging. 2013;6:249-262.
21. Litmanovich DE, Ghersin E, Burke DA, Popma J, Shahrzad M, Bankier AA. Imaging in transcatheter aortic valve replacement (TAVR): role of the radiologist. Insights Imaging. 2014;5:123-145.
22. Garrido JM, Ferreiro A, Samaranch N, Salido L, Garcia-Andrade I. Interventricular septal rupture after transcatheter aortic valve implantation: surgical and perioperative management. J Card Surg. 2014;29:478-481.
From the 1Division of Cardiology, 2Division of Cardiovascular Surgery, and 3Division of Radiology, the University of Pennsylvania Medical Center, Philadelphia, Pennsylvania.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Giri reports research support from St. Jude Medical. Dr Jha reports speaker fees from Toshiba Medical Systems. Dr Herrmann reports grants to his institution from Abbott Vascular, Boston Scientific, Edwards Lifesciences, St. Jude Medical, and Medtronic (relevant to the work herein) as well as from Gore, Siemens, Cardiokinetx, University of Laval, and Mitraspan (outside the submitted work); consulting fees from Edwards Lifesciences (relevant to the work herein) and from Siemens, Wells Fargo, and Leerink (outside the submitted work). Dr Anwaruddin reports consulting/speaker’s fees from Edwards Lifesciences and Medtronic (outside the submitted work). The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 14, 2016, and accepted March 23, 2016.
Address for correspondence: Saif Anwaruddin, MD, FACC, FSCAI, 3400 Spruce 9 Gates, Philadelphia, PA 19104. Email: saif.anwaruddin@uphs.upenn.edu










