

Novel Method of Rescuing Kinked Guide Catheter From Axillary Artery in Transradial Coronary Intervention: The Balloon Retrieval Technique
Abstract: This case illustrates a novel and innovative method of retrieving a kinked guiding catheter in transradial intervention without the need for vascular snare.
J INVASIVE CARDIOL 2012;24(9):E205-E206
Key words: kinked guiding catheter, transradial complication
__________________________________________________________
Case Report
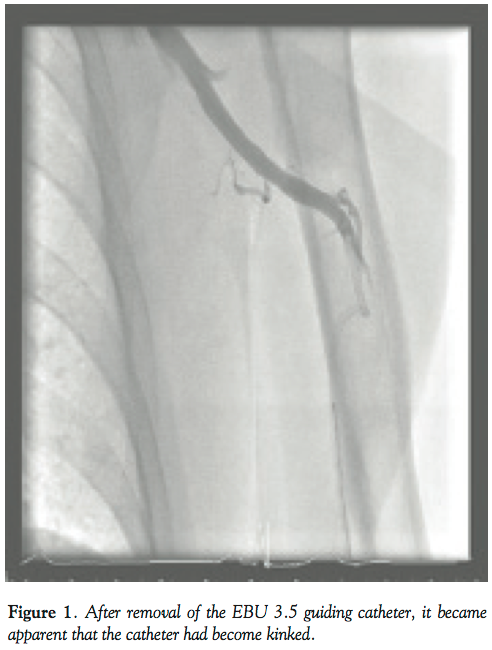 An 86-year-old male with diabetes, hypertension, and peripheral vascular disease presented to our institution with non-ST elevation myocardial infarction (NSTEMI). Coronary angiography performed by the left radial approach demonstrated a severe lesion in the mid left circumflex (LCX) artery and a further lesion in the mid left anterior descending (LAD) artery. Both lesions were successfully treated with percutaneous intervention with the use of bare-metal stents (3.5 x 15 mm in LCX, 3.0 x 28 mm in LAD) with excellent angiographic outcomes. On removal of the EBU 3.5 guiding catheter (Cordis Corporation), it became apparent that the catheter had become kinked (Figure 1) and was unable to be untwisted using conventional techniques involving guide catheter manipulation, the standard 0.035˝ guidewire, a super-stiff wire, and gentle rotation. Despite multiple attempts at unraveling the catheter, it could not be removed through the left radial access point and the patient experienced considerable discomfort with each manipulation.
An 86-year-old male with diabetes, hypertension, and peripheral vascular disease presented to our institution with non-ST elevation myocardial infarction (NSTEMI). Coronary angiography performed by the left radial approach demonstrated a severe lesion in the mid left circumflex (LCX) artery and a further lesion in the mid left anterior descending (LAD) artery. Both lesions were successfully treated with percutaneous intervention with the use of bare-metal stents (3.5 x 15 mm in LCX, 3.0 x 28 mm in LAD) with excellent angiographic outcomes. On removal of the EBU 3.5 guiding catheter (Cordis Corporation), it became apparent that the catheter had become kinked (Figure 1) and was unable to be untwisted using conventional techniques involving guide catheter manipulation, the standard 0.035˝ guidewire, a super-stiff wire, and gentle rotation. Despite multiple attempts at unraveling the catheter, it could not be removed through the left radial access point and the patient experienced considerable discomfort with each manipulation.
 We elected to convert to a right femoral approach with a view to rescue the kinked catheter with use of a vascular snare. However, due to a lack of an available appropriately-sized snare and concerns with the use of a large-caliber sheath in an octogenarian with peripheral vascular disease, we explored other options. We elected to use a novel balloon retrieval technique. A 6 Fr JR4 guide was used to enter the left subclavian artery and manipulated to lie within close proximity of the kinked EBU 3.5 catheter. A Whisper MS wire was advanced through the JR4 guide in an attempt to enter the distal end of the kinked guide catheter (Figure 2). Eventually, the Whisper wire passed into the kinked catheter and was manipulated into the proximal limb of the kinked guide. A 3.0 x 15 mm NC balloon was then passed through the JR4 guide over the guidewire into the distal end of the kinked guiding catheter. The balloon was inflated to 16 atm and gentle backward traction was applied to the JR4 guide (Figure 3). Eventually, both the JR4 guide and the kinked catheter were brought back to the ascending aorta (Figure 4). The catheter was untwisted using the JR4/balloon system that enabled controlled manipulation in the ascending aorta, enabling the EBU 3.5 guide to be removed from the left radial sheath with the use of a standard 0.035˝ wire. Following the procedure, the patient had a good radial pulse without complication.
We elected to convert to a right femoral approach with a view to rescue the kinked catheter with use of a vascular snare. However, due to a lack of an available appropriately-sized snare and concerns with the use of a large-caliber sheath in an octogenarian with peripheral vascular disease, we explored other options. We elected to use a novel balloon retrieval technique. A 6 Fr JR4 guide was used to enter the left subclavian artery and manipulated to lie within close proximity of the kinked EBU 3.5 catheter. A Whisper MS wire was advanced through the JR4 guide in an attempt to enter the distal end of the kinked guide catheter (Figure 2). Eventually, the Whisper wire passed into the kinked catheter and was manipulated into the proximal limb of the kinked guide. A 3.0 x 15 mm NC balloon was then passed through the JR4 guide over the guidewire into the distal end of the kinked guiding catheter. The balloon was inflated to 16 atm and gentle backward traction was applied to the JR4 guide (Figure 3). Eventually, both the JR4 guide and the kinked catheter were brought back to the ascending aorta (Figure 4). The catheter was untwisted using the JR4/balloon system that enabled controlled manipulation in the ascending aorta, enabling the EBU 3.5 guide to be removed from the left radial sheath with the use of a standard 0.035˝ wire. Following the procedure, the patient had a good radial pulse without complication.
Discussion
 The transradial approach is an increasingly utilized access site for coronary intervention. Data from the recently published RIVAL study has shown advantages of using the radial approach above the femoral.1 Therefore, the uptake of radial intervention would be expected to increase. Complications of radial intervention will more commonly be observed. We present a novel method for retrieval of a kinked guiding catheter that is useful for clinicians and an alternative to the vascular snare.
The transradial approach is an increasingly utilized access site for coronary intervention. Data from the recently published RIVAL study has shown advantages of using the radial approach above the femoral.1 Therefore, the uptake of radial intervention would be expected to increase. Complications of radial intervention will more commonly be observed. We present a novel method for retrieval of a kinked guiding catheter that is useful for clinicians and an alternative to the vascular snare.
 Specific advantages of the balloon retrieval technique. This technique: (1) Avoided placement of a large-caliber femoral sheath in an elderly man that may have been necessary with the use of a vascular snare; (2) Provided absolute control of both catheters at all times — at no stage did we lose the distal end of trapped catheter. We postulate that this would not have been possible with the snare; and (3) We would argue that this technique should be considered in all patients to retrieve kinked catheters.
Specific advantages of the balloon retrieval technique. This technique: (1) Avoided placement of a large-caliber femoral sheath in an elderly man that may have been necessary with the use of a vascular snare; (2) Provided absolute control of both catheters at all times — at no stage did we lose the distal end of trapped catheter. We postulate that this would not have been possible with the snare; and (3) We would argue that this technique should be considered in all patients to retrieve kinked catheters.
Reference
- Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(9775):1409-1420
__________________________________________________________
From the 1Golden Jubilee National Hospital, Clydebank, Scotland and 2Hairmyres Hospital, East Kilbride, Scotland.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 29 2012, and accepted May 29, 2012.
Address for correspondence: Dr Jamie J. Layland, MBChB, St Vincent’s Hospital, Cardiology, Victoria Parade, Fitzroy, Victoria Vic 3101, Australia. Email: jamielayland@hotmail.com











