

Novel Technique of Advancing the Rotational Atherectomy Device: "Single-Operator" Technique
Abstract: Objective. We report the clinical outcomes of the “single-operator” technique, whereby the operator both advances the rotational atherectomy (RA) device and keeps the distal wire in place. Background. Severely calcified lesions are associated with increased ischemic complications during percutaneous coronary intervention. RA, which utilizes a differential cutting mechanism of action for plaque modification, is a valuable treatment option for patients with severely calcified vessels prior to stent implantation. Reasons that may explain the underutilization include lack of operator experience and the availability of a skilled assistant to maintain wire position while the operator advances the device to the lesion. Loss of wire position can lead to increased procedural and fluoroscopic times. Methods. In a prospective single-center study, a total of 67 consecutive patients underwent RA from July 2012 to June 2015. The primary endpoint was successful delivery of the RA device to the lesion without losing wire position with procedural success. Results. The primary endpoint was met in 100% of the patients. The 30-day major adverse cardiac and cerebrovascular event rate was 6.0%, all due to non-fatal myocardial infarction. There was no cardiac death, target lesion revascularization, stroke, stent thrombosis, perforation, or flow-limiting dissection. Five patients had slow flow, but resolved with intracoronary vasodilator therapy and achieved TIMI grade 3 flow. Conclusion. RA can be performed successfully without a skilled assistant to maintain wire position during advancement of the burr, and the absence of an assistant should therefore not eliminate the performance of RA.
J INVASIVE CARDIOL 2016;28(5):183-186
Key words: rotational atherectomy, rotablator, plaque
_____________________________________________
Rotational atherectomy (RA) can be performed after advancing a specialized wire across the target lesion. An assistant is needed to fix and stabilize the wire in position at the end of the catheterization lab table while the primary operator advances the burr and drive shaft. This part is challenging and the technique requires an operator and assistant who work carefully in sync. However, a qualified assistant is not always available or the primary operator may not want to risk the loss of wire position by accidental movements of an inexperienced assistant or trainee. While in theory procedures could be delayed or rescheduled to ensure adequate assistance for the primary operator during these cases, we found that due to busy hospital schedules and limited cath lab time, this can be challenging and is usually not encouraged. Therefore, we developed a “single-operator” technique that allows both delivery and retrieval of an RA device with only one operator. We collected data from 67 cases during which this technique was used and found it to be very safe and effective. We report the outcomes of this single-operator method for the use of RA for severely calcified coronary lesions.
Methods
Study population. A total of 67 consecutive patients underwent RA (Boston Scientific) from July 2012 to June 2015 at the UCLA Medical Center in Los Angeles, California with the one-man technique. Patients were included if the lesion was severely calcified and reference vessel diameter was ≥2.5 mm and ≤5.0 mm, with stenosis of ≥70%. Severely calcified vessels were defined by the presence of radioopacities on fluoroscopy involving both sides of the arterial wall. Patients were excluded if they had ST-elevation myocardial infarction.
Procedures and medical treatment. Percutaneous coronary intervention (PCI) was performed via the transfemoral or transradial approach with standard techniques. Patients were treated with aspirin and clopidogrel prior to RA. Intravenous heparin was administered to maintain the activated clotting time >250 seconds. Assessment of fractional flow reserve was obtained for intermediate coronary lesions. The decision to insert a temporary transvenous pacemaker, administration of preprocedural intracoronary nitroglycerin, and choice of drug-eluting stent (DES) or bare-metal stent were at the operator’s discretion.
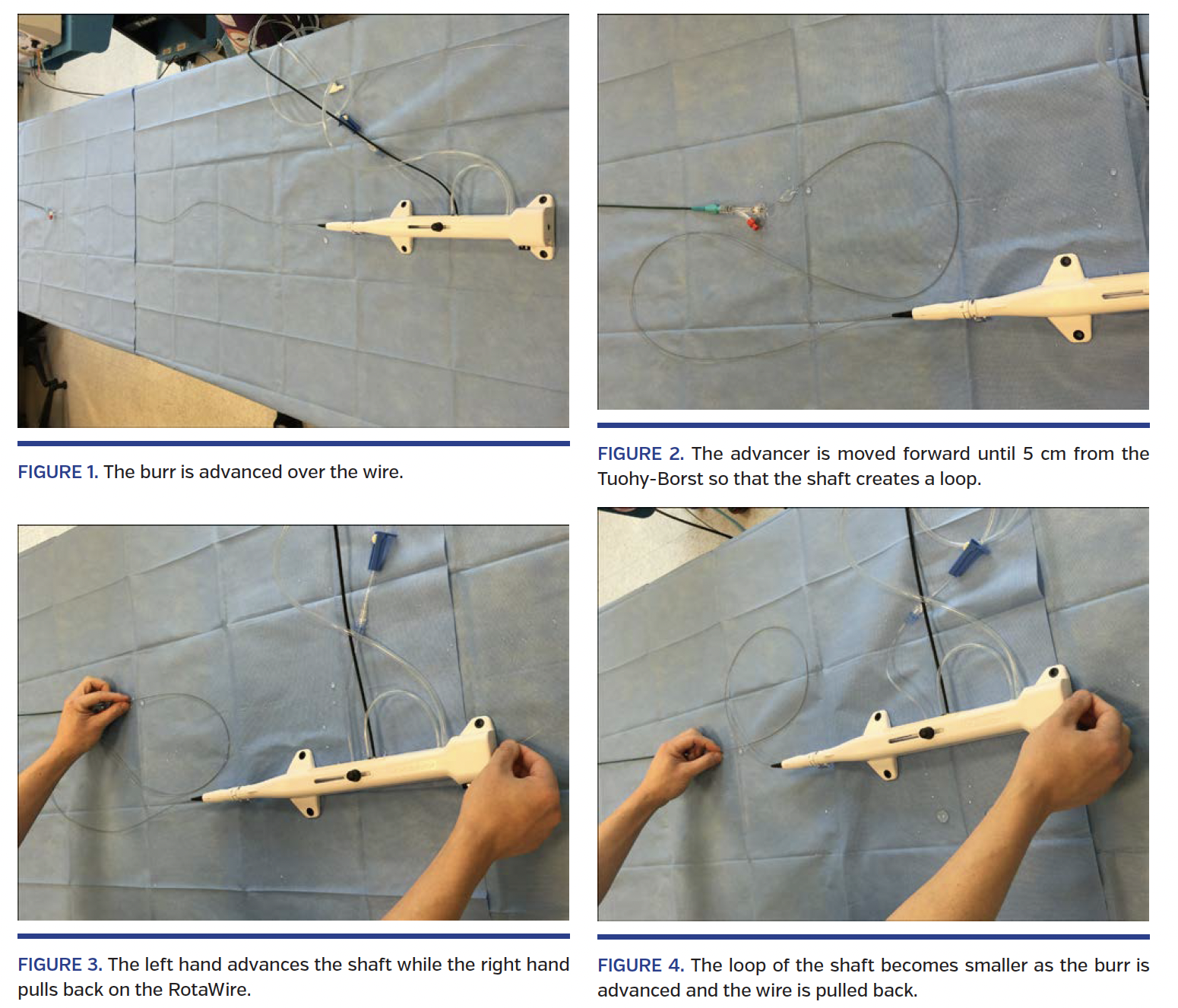
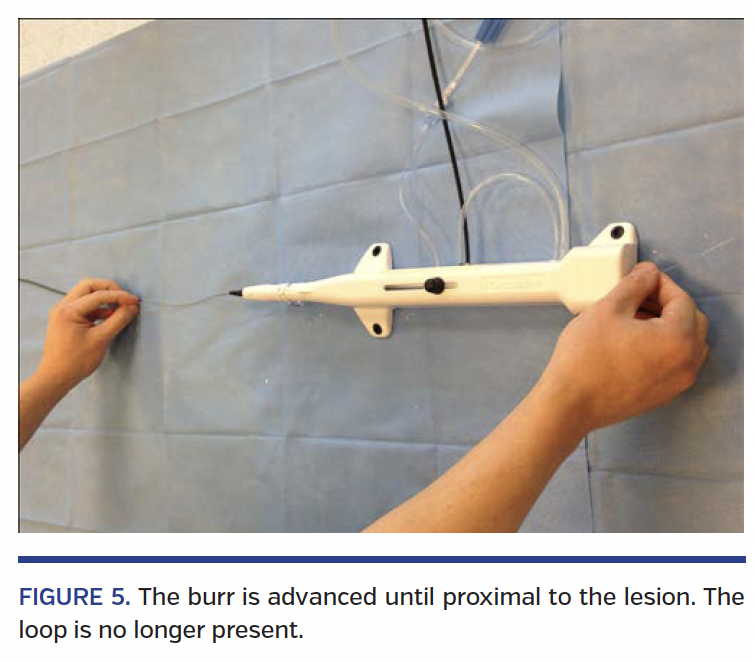
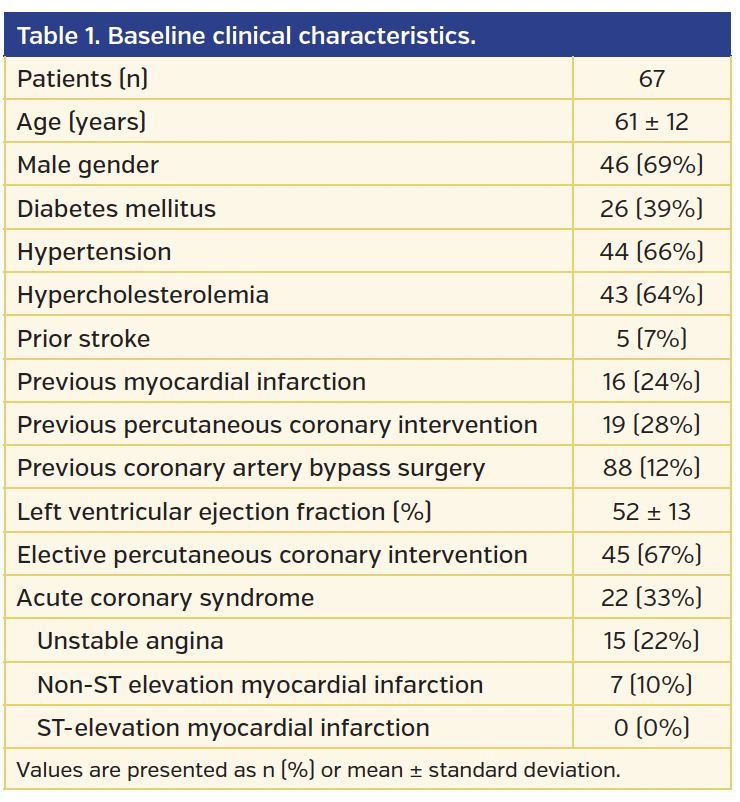
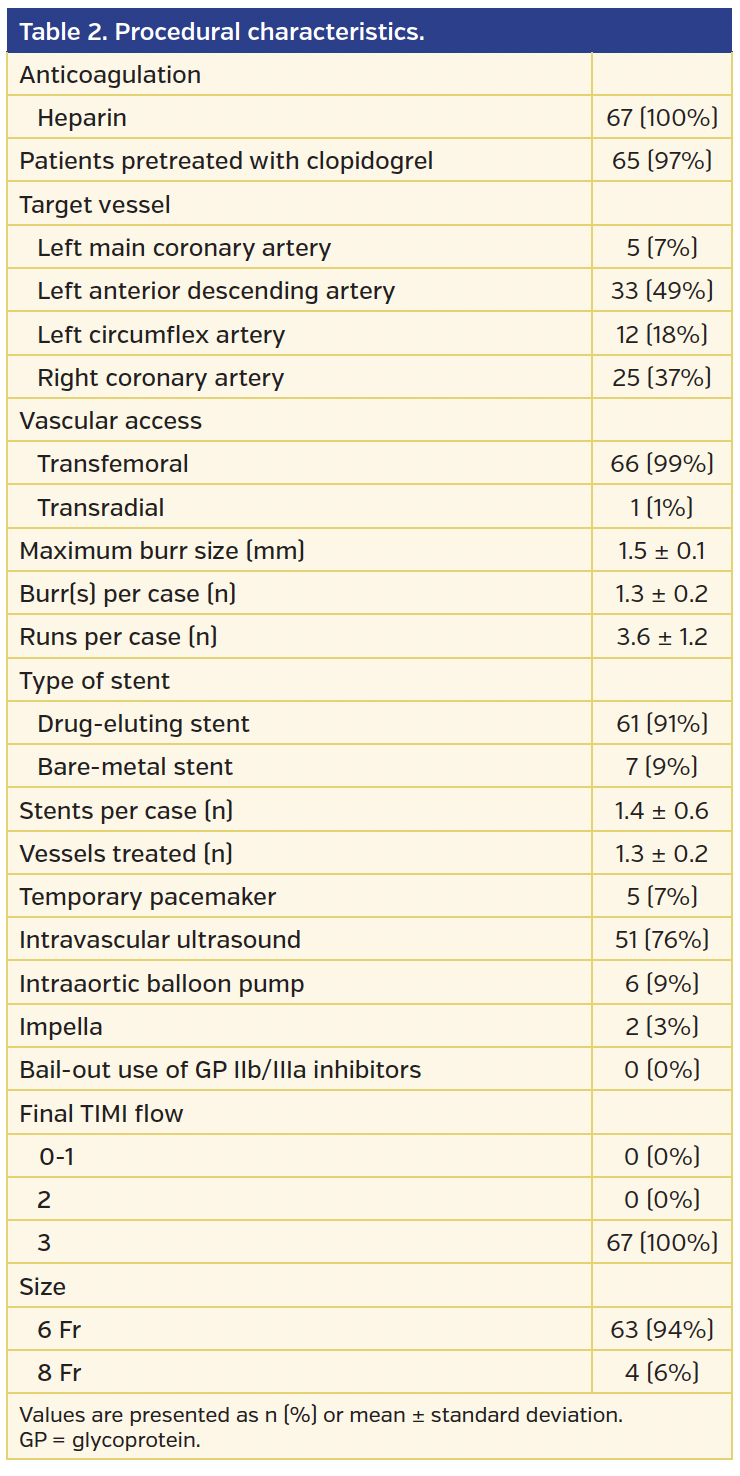
The burr is attached to a driveline and spins at high speeds. The size of the burr was approximately 50% of the reference vessel diameter.1,2 A 6 Fr guiding catheter was used to accommodate a 1.25 mm or 1.5 mm burr, while a 7 Fr or 8 Fr guiding catheter was used to accommodate a 1.75 mm or 2 mm burr. A Rota-floppy wire (Boston Scientific) was used for all cases. A Telfa non-adherent pad (Tyco Healthcare) was used to wipe the Rota-floppy wire thoroughly to remove the grit when it was removed from the package and in between exchanges to larger burrs. The benefit of using a Telfa pad is that it does not shed lint like a conventional 4 x 4 gauze that may adhere to the RotaWire Floppy guidewire. The rota-flush contained 10,000 units of heparin in a 1 L bag of normal saline. The burr was tested and primed prior to insertion into the guiding catheter at 150,000 to 170,000 rpm while mounted on the wire. After the burr is advanced through the Tuohy Borst (Figure 1), the shaft is looped in an “S” configuration and the advancer is placed next to the Tuohy Borst (Figure 2). The burr is advanced over the wire with the left hand while the right hand simultaneously pulls the RA wire back, while monitoring the wire position under fluoroscopy (Figures 3-5; Video 1). Each pass with the burr across the lesion was limited to 20 seconds or less. After plaque modification is completed, the burr can also be removed by the single-operator technique by opening the Tuohy Borst and just pushing the RA wire (Video 2).
Dual-antiplatelet therapy was continued for at least 1 month for bare-metal stent and 1 year for drug-eluting stent. All patients were treated with optimal medical therapy including beta-blockers, angiotensin-converting enzyme inhibitors, or angiotensin II receptor blockers, and statins, unless contraindicated.
Study endpoints and clinical follow-up. The primary endpoint was procedural success without the need to take the burr off the RotaWire to reposition it. Procedural success was defined as residual stenosis ≤30% and TIMI flow grade 3 without death, emergency coronary artery bypass graft surgery, and/or PCI during the first 24 hours. Major adverse cardiac and cerebral events were defined as the composite of cardiac death, non-fatal myocardial infarction, target-lesion revascularization, and stroke. Death was considered cardiac in origin unless a non-cardiac origin was documented. Myocardial infarction was defined as recurrent symptoms with new ST-segment elevation or re-elevation of cardiac markers to at least twice the upper limit of normal. Target-lesion revascularization was defined as repeat revascularization of the target lesion within the stent or in the 5 mm distal or proximal segments.
Patient data were collected from medical records, and adverse clinical events were recorded into a dedicated PCI database.
Statistical analysis. Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as percentages. All data were processed with SPSS version 20.0 (SPSS-PC, Inc).
Results
Baseline characteristics. Baseline characteristics of the 67 patients are presented in Table 1. The mean age was 64.3 ± 12.1 years. Procedural characteristics are presented in Table 2. The mean number of burrs used was 1.3 ± 0.2. The mean maximum burr size was 1.5 ± 0.1 mm. The mean number of stents used was 1.6 ± 0.4.
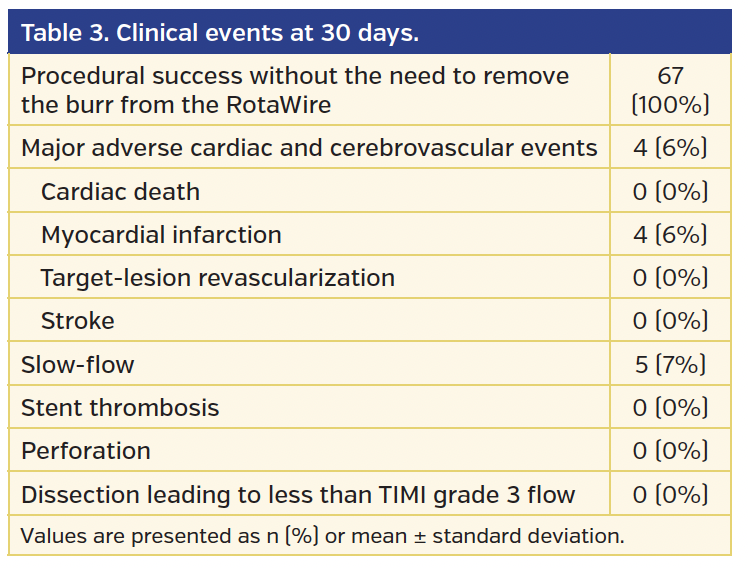
Clinical outcomes at 30 days. All 67 patients had procedural success (Table 3). Major adverse cardiac-cerebral events occurred in 6.0%, all due to non-fatal myocardial infarction. There was no death, target-lesion revascularization, or stroke. Five patients had slow-flow, but resolved with intracoronary vasodilator therapy and achieved TIMI grade 3 flow. There was no stent thrombosis, perforation, or flow-limiting dissection.
Discussion
Underutilization of RA is in part due to the requirement of special equipment, conflicting data on its clinical benefit, and the need for a skilled operator and assistant.3,4 The single-operator technique, whereby a single operator advances the RA system while simultaneously maintaining wire position, is safe and effective and obviates the need for an assistant who is skilled with this technology. All patients underwent successful RA without loss of wire position during advancement of the rotablator burr. Maintenance of wire position in cases where RA is used is critical, since loss of wire position can lead to increased procedural and fluoroscopic times. If the wire is inadvertently pulled back, it is difficult to advance and appropriately reposition the wire if the burr is on it, and may necessitate removal of the burr to re-advance the wire. More serious consequences could result if the wire is pulled back proximal to the lesion, potentially making it unfeasible to traverse the lesion if there is a dissection, which may lead to ischemia, the inability to complete the PCI successfully, and possibly the need for emergent coronary artery bypass surgery. If the wire is not held firmly in place while advancing the RA burr, the guiding catheter could be disengaged from the ostium of the coronary artery.
The learning curve for this technique is steep. Personally speaking, the comfort level for this technique was reached within the first 3 cases. When a case requires upsizing to a larger burr, it may be difficult to advance the burr given the increase in friction and resistance, especially when a third burr is needed for a case. We therefore recommend constant wiping of the RotaWire with a wet Telfa pad in between burr exchanges, which can minimize the formation of grit from dried contrast and blood that develops on the wire and therefore increase procedural success.
Conclusion
RA using the single-operator technique is a feasible, safe, and an effective treatment option for severely calcified lesions. Although mastery of this technique may take several cases, it makes RA user friendly, and an invaluable technique when a skilled assistant is not available, and removes a barrier to its use.
Study limitations. This was a non-randomized study from a single center by a single operator (MSL) with a small number of patients. The vast majority of cases were performed using the transfemoral approach. Therefore, the reproducibility of this technique using the transradial approach has not been validated. The results of our study need to be validated in a multicenter study with long-term follow-up. Postprocedural cardiac biomarkers were not drawn on all patients. Therefore, periprocedural myocardial infarction may have been underdiagnosed.
References
1. Safian RD, Feldman T, Muller DW, et al. Coronary angioplasty and Rotablator atherectomy trial (CARAT): immediate and late results of a prospective multicenter randomized trial. Catheter Cardiovasc Interv. 2001;53:213-220.
2. Whitlow PL, Bass TA, Kipperman RM, et al. Results of the study to determine rotablator and transluminal angioplasty strategy (STRATAS). Am J Cardiol. 2001;87:699-705.
3. Sharma SK, Kini A, Mehran R, Lansky A, Kobayashi Y, Marmur JD. Randomized trial of rotational atherectomy versus balloon angioplasty for diffuse in-stent restenosis (ROSTER). Am Heart J. 2004;147:16-22.
4. Abdel-Wahab M, Richardt G, Joachim Buttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6:10-19.
_________________________________________
From the ¹Division of Cardiology, University of California, Los Angeles Medical Center, Los Angeles, California; and 2Cardiovascular Center, Korea University Guro Hospital, Seoul, Republic of Korea.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Lee is on the speaker’s bureau of CSI. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 10, 2015, provisional acceptance given November 30, 2015, final version accepted December 10, 2015.
Address for correspondence: Dr Michael S. Lee, 100 Medical Plaza, Suite 630, Los Angeles, CA 90095. Email: mslee@mednet.ucla.edu











