

Novel Use of a GuideLiner Catheter to Visualize Distal LAD After LIMA Anastomosis in Selective Coronary Angiography
ABSTRACT: We report a case of GuideLiner catheter use during transradial intervention for selective coronary angiography of the distal left anterior descending artery (LAD), beyond the left internal mammary artery (LIMA) anastomosis. The lesion within the LAD was located distal to the anastomosis of a very tortuous LIMA, otherwise unable to be visualized due to competitive flow from the LIMA. Stenting by way of the LIMA could not be performed due to this severe tortuosity as well. Alternatively, performance of the intervention without GuideLiner assistance would have required dual access, with injections both through the LIMA graft and the native LAD for angiography and intervention. Use of the GuideLiner served the purpose of selective LAD angiography to visualize the lesion, as well as delivery of the stent through a proximally calcified LAD. Using this single transradial route allowed the intervention to be completed, while reducing complications due to multiple access sites.
J INVASIVE CARDIOL 2012;24(2):E30-E31
_________________________________
The GuideLiner catheter is a “mother-and-child” guide extension intended to provide extra support needed for balloon or stent delivery. It can be placed over an exchange length (300 cm) or 180 cm guidewire because it is a rapid exchange 145 cm device with a stainless steel shaft and 20 cm single lumen catheter.
 Transradial intervention enables early ambulation, as well as reduced access site complications from percutaneous coronary intervention (PCI).1-3 However, meta-analysis shows that there is an increased crossover rate to a transfemoral approach, as well as increased fluoroscopic time with the transradial route.4 With the introduction of the GuideLiner catheter, it is possible that some of this crossover can be reduced.
Transradial intervention enables early ambulation, as well as reduced access site complications from percutaneous coronary intervention (PCI).1-3 However, meta-analysis shows that there is an increased crossover rate to a transfemoral approach, as well as increased fluoroscopic time with the transradial route.4 With the introduction of the GuideLiner catheter, it is possible that some of this crossover can be reduced.
Case Report
 We report a 76-year-old male patient with a previous history of hypertension, hypercholesterolemia, diabetes mellitus, and ischemic cardiomyopathy. The patient has an automatic implanted cardioverter-defibrillator and coronary artery bypass grafting (LIMA to LAD, saphenous vein graft to right posterior descending artery, and saphenous vein graft to diagonal branch). He presented with symptoms of angina and an abnormal stress test that demonstrated a large anterior wall defect. Coronary angiography was performed by his attending cardiologist, and illustrated a 90% stenosis of the LAD after a tortuous LIMA. The LIMA was only visualized after selective angiography due to competitive flow during native coronary angiography. The saphenous vein graft to the posterior descending artery was patent. The patient had renal insufficiency and was scheduled to return for an intervention of the LAD lesion.
We report a 76-year-old male patient with a previous history of hypertension, hypercholesterolemia, diabetes mellitus, and ischemic cardiomyopathy. The patient has an automatic implanted cardioverter-defibrillator and coronary artery bypass grafting (LIMA to LAD, saphenous vein graft to right posterior descending artery, and saphenous vein graft to diagonal branch). He presented with symptoms of angina and an abnormal stress test that demonstrated a large anterior wall defect. Coronary angiography was performed by his attending cardiologist, and illustrated a 90% stenosis of the LAD after a tortuous LIMA. The LIMA was only visualized after selective angiography due to competitive flow during native coronary angiography. The saphenous vein graft to the posterior descending artery was patent. The patient had renal insufficiency and was scheduled to return for an intervention of the LAD lesion.
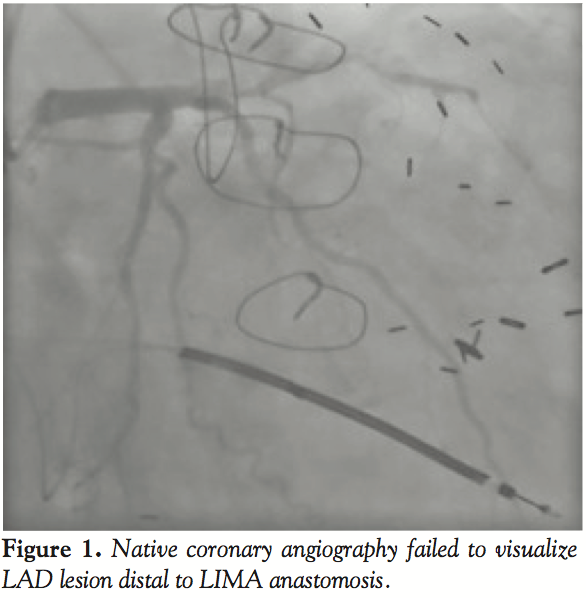
 After a review of the angiographic images, we determined that the lesion in the LAD could not be visualized during native left coronary angiography (Figure 1). PCI of the LAD could not be performed through the LIMA due to its severe tortuosity (Figures 2 and 3).
After a review of the angiographic images, we determined that the lesion in the LAD could not be visualized during native left coronary angiography (Figure 1). PCI of the LAD could not be performed through the LIMA due to its severe tortuosity (Figures 2 and 3).
The initial plan was to obtain dual access for LIMA angiography and LAD intervention. This would obviously increase the chance of access site complication and add to the complexity of seating a catheter in the LIMA with dual injections.
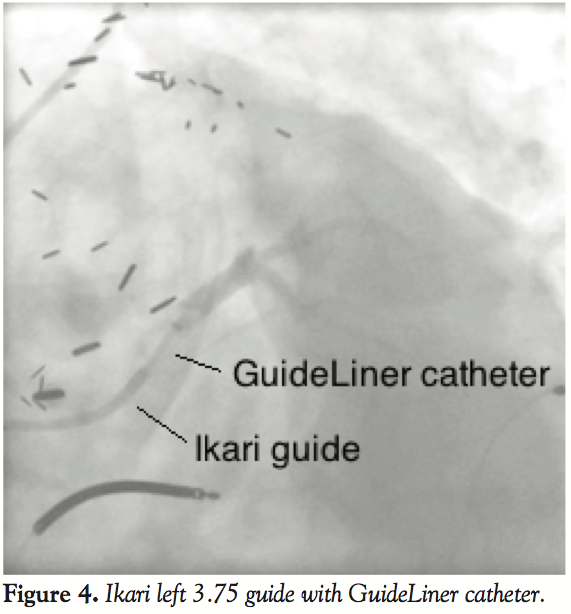 Instead, a right radial approach was used for the intervention. An Ikari Left 3.75 guide catheter (Terumo) was utilized along with a GuideLiner for selective LAD angiography. This allowed for superior visualization of the LAD lesion (Figures 4 and 5), and facilitated stent delivery through a calcified proximal LAD. A Runthrough™ NS wire (Terumo) was used to cross the lesion. Difficulty in-stent advancement though the native proximal LAD was encountered, and therefore predilation was performed. A 3.0 x 15 mm Xience V stent (Abbott) was deployed. Excellent angiographic results followed (Figure 6), and the patient was discharged the next day without any access site complications or rise in serum creatinine level. The case was converted from complex to straightforward.
Instead, a right radial approach was used for the intervention. An Ikari Left 3.75 guide catheter (Terumo) was utilized along with a GuideLiner for selective LAD angiography. This allowed for superior visualization of the LAD lesion (Figures 4 and 5), and facilitated stent delivery through a calcified proximal LAD. A Runthrough™ NS wire (Terumo) was used to cross the lesion. Difficulty in-stent advancement though the native proximal LAD was encountered, and therefore predilation was performed. A 3.0 x 15 mm Xience V stent (Abbott) was deployed. Excellent angiographic results followed (Figure 6), and the patient was discharged the next day without any access site complications or rise in serum creatinine level. The case was converted from complex to straightforward.
Discussion
 The GuideLiner catheter is a new device in the coronary interventional field that has been used for assistance with device delivery. Usually, it has been used as a “bail-out” device if a stent cannot cross. As the device is a guide extension, it selectively intubates the coronary artery. This specific property was utilized in this case to visualize a lesion in the LAD that was not seen due to competitive flow from the LIMA. This simplified the procedure for the patient, and reduced the risks associated with multiple access sites.
The GuideLiner catheter is a new device in the coronary interventional field that has been used for assistance with device delivery. Usually, it has been used as a “bail-out” device if a stent cannot cross. As the device is a guide extension, it selectively intubates the coronary artery. This specific property was utilized in this case to visualize a lesion in the LAD that was not seen due to competitive flow from the LIMA. This simplified the procedure for the patient, and reduced the risks associated with multiple access sites.
 Although the GuideLiner catheter was useful in this case for selective coronary angiography, one must be cautious while advancing this catheter into coronary arteries. There is an inherent risk of plaque disruption, which could lead to vessel dissection. Acknowledging this, the GuideLiner is still a valuable tool in the field of interventional cardiology.
Although the GuideLiner catheter was useful in this case for selective coronary angiography, one must be cautious while advancing this catheter into coronary arteries. There is an inherent risk of plaque disruption, which could lead to vessel dissection. Acknowledging this, the GuideLiner is still a valuable tool in the field of interventional cardiology.
Conclusion
The GuideLiner catheter can be used for selective LAD angiography in cases where there is competitive flow from the LIMA present.
References
- Kiemeneij F, Laarman GJ. Percutaneous transradial artery approach for coronary stent implantation. Catheter Cardiovasc Diagn.1993 Oct;30(2):173-178.
- Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J. 2009 Jan;157(1):132-140.
- Vorobcsuk A, Kónyi A, Aradi D, et al. Transradial versus transfemoral percutaneous coronary intervention in acute myocardial infarction systematic overview and meta-analysis. Am Heart J. 2009 Nov;158(5):814-821.
- Saito S, Miyake S, Hosokawa G, et al. Transradial coronary intervention in Japanese patients. Catheter Cardiovasc Interv. 1999 Jan;46(1):37-41;discussion 42.
_________________________________
From the Department of Cardiology, West Suburban Medical Center, Oak Park, Illinois.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 21, 2011, provisional acceptance given July 18, 2011, final version accepted July 27, 2011.
Address for correspondence: Asif Serajian, DO, FACC, 1000 W Adams, #603, Chicago, IL, 60607. Email: aserajian1@gmail.com













