

Occlusion of a Left Internal Mammary Artery Graft Side Branch During Attempts to Deliver an Amplatzer Vascular Plug
ABSTRACT: We present a case of angina in a patient with a left internal mammary artery graft that had a large side branch. Closure was attempted using an Amplatzer vascular plug but during attempts to position the device, the side-branch occluded, likely due to dissection, obviating the need for device deployment.
J INVASIVE CARDIOL 2011;23(10):E229–E231
Key words: coronary bypass graft surgery, LIMA graft, devices
_____________________________________
Introduction
Angina after coronary artery bypass grafting (CABG) in which a left internal mammary arterial conduit is used may be due to coronary “steal” through large left internal mammary artery (LIMA) side branches. Occlusion of these branches can be achieved either surgically1,2 or percutaneously and may result in ischemia resolution and angina relief.3 In this case, we attempted to occlude a large LIMA side branch with an Amplatzer vascular plug (AGA Medical), which resulted in side-branch dissection and occlusion before release of the device.
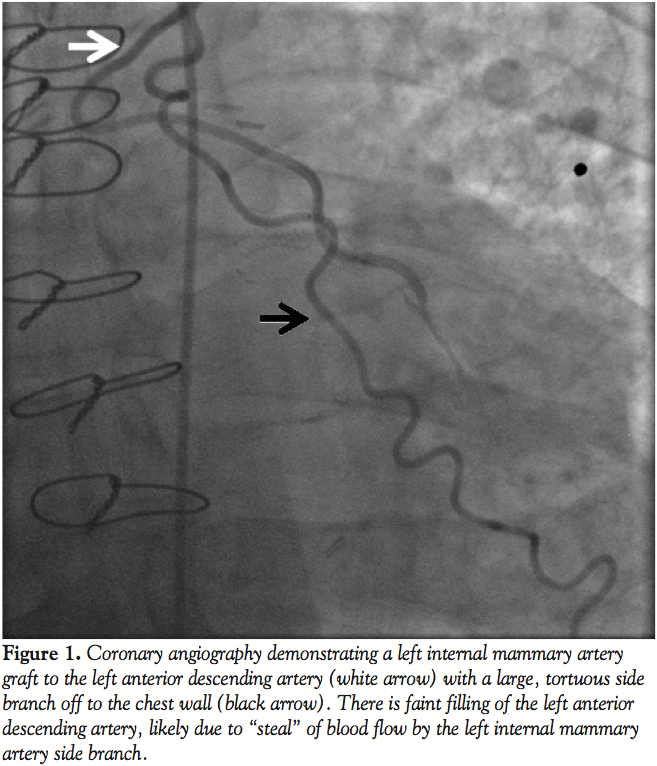 Case Report. A 60-year-old man with a history of diabetes mellitus, hypertension, and paroxysmal atrial fibrillation, presented with angina in spite of intensive antianginal medical therapy. A stress test demonstrated anterior ischemia. He had undergone CABG 7 years prior to presentation with implantation of a LIMA to the left anterior descending artery (LAD) and 2 saphenous vein grafts (SVG) to the posterior descending artery and the second obtuse marginal artery. Although angina improved after CABG, he continued to have exertional chest pain that subsequently worsened. Coronary angiography revealed that all bypass grafts were patent. The LIMA to LAD had a large side branch (Figure 1). In view of the severity of the patient’s symptoms and the lack of other possible culprit lesions, percutaneous occlusion of the LIMA side branch was planned.
Case Report. A 60-year-old man with a history of diabetes mellitus, hypertension, and paroxysmal atrial fibrillation, presented with angina in spite of intensive antianginal medical therapy. A stress test demonstrated anterior ischemia. He had undergone CABG 7 years prior to presentation with implantation of a LIMA to the left anterior descending artery (LAD) and 2 saphenous vein grafts (SVG) to the posterior descending artery and the second obtuse marginal artery. Although angina improved after CABG, he continued to have exertional chest pain that subsequently worsened. Coronary angiography revealed that all bypass grafts were patent. The LIMA to LAD had a large side branch (Figure 1). In view of the severity of the patient’s symptoms and the lack of other possible culprit lesions, percutaneous occlusion of the LIMA side branch was planned.
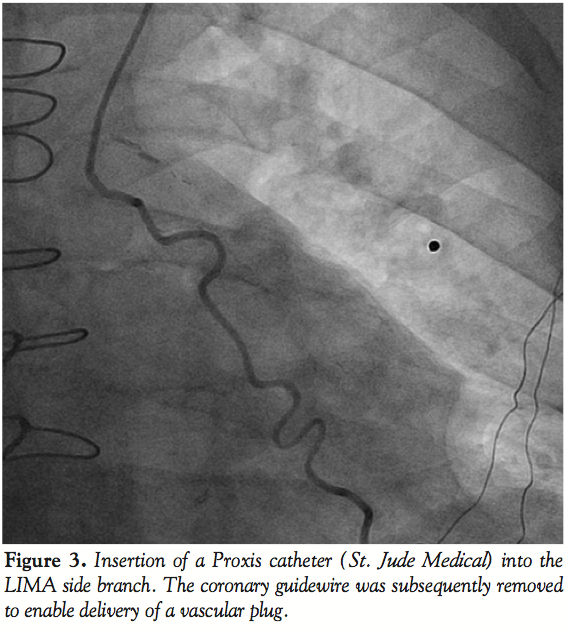
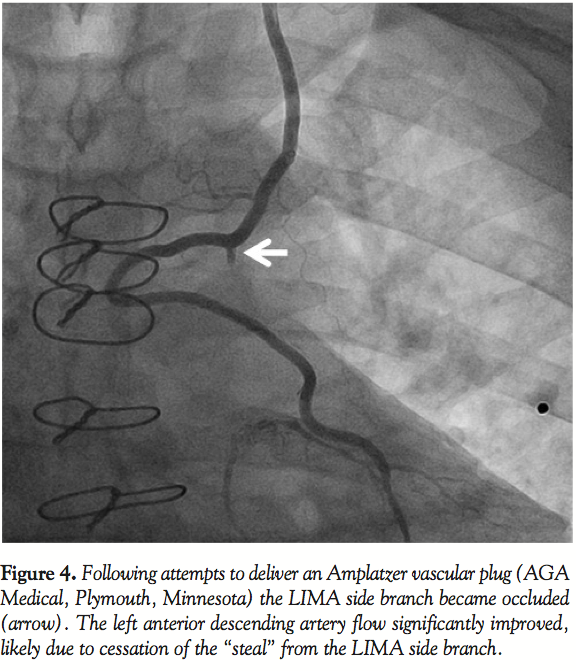
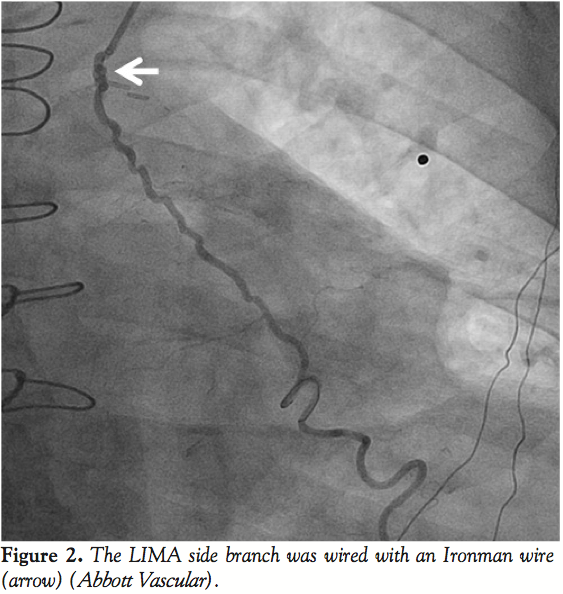 Left radial access was obtained with a 6 Fr sheath. The LIMA was wired with an Ironman wire (Abbott Vascular; Figure 2) and a Proxis catheter (St. Jude Medical) was inserted into the LIMA side branch (Figure 3). We attempted to deliver a 3 mm Amplatzer vascular plug (AGA Medical) through the Proxis catheter in the LIMA side branch, however significant resistance was encountered during delivery attempts. The device was partially deployed but in suboptimal location due to movement of the catheter during delivery. The vascular plug was recaptured and removed. LIMA angiography demonstrated side-branch occlusion. The LIMA side branch remained occluded after 15 minutes of observation. The patient had an uneventful recovery and has had no recurrent angina during 3 months of follow-up.
Left radial access was obtained with a 6 Fr sheath. The LIMA was wired with an Ironman wire (Abbott Vascular; Figure 2) and a Proxis catheter (St. Jude Medical) was inserted into the LIMA side branch (Figure 3). We attempted to deliver a 3 mm Amplatzer vascular plug (AGA Medical) through the Proxis catheter in the LIMA side branch, however significant resistance was encountered during delivery attempts. The device was partially deployed but in suboptimal location due to movement of the catheter during delivery. The vascular plug was recaptured and removed. LIMA angiography demonstrated side-branch occlusion. The LIMA side branch remained occluded after 15 minutes of observation. The patient had an uneventful recovery and has had no recurrent angina during 3 months of follow-up.
 Discussion. Our case demonstrates an unconventional method for occluding a LIMA side branch by causing dissection of the side branch during attempts to place an Amplatzer vascular plug.
Discussion. Our case demonstrates an unconventional method for occluding a LIMA side branch by causing dissection of the side branch during attempts to place an Amplatzer vascular plug.
The LIMA often possesses pectoral branches that perfuse the chest wall. Kern4 estimated the prevalence of large LIMA side branches to be approximately 10% to 20%. Bauer et al reviewed 459 patients who underwent LIMA grafting and found large side branches in 41 (9%).5 The prevalence of large LIMA side branches may be higher among patients undergoing minimally invasive CABG due to partial LIMA visualization compared to median sternotomy.
 Whether coronary “steal” through a LIMA side branch can cause angina after CABG remains debatable. Flow via the LIMA side branches occurs mainly during systole, whereas the majority of flow to the coronary target vessel occurs during diastole.6 No significant change in LAD flow or LIMA coronary flow reserve has been demonstrated after balloon occlusion of the LIMA side branches7 or adenosine-induced hyperemia.8 However, there are several reports of anginal improvement and resolution of ischemia on myocardial perfusion imaging after successful occlusion of a large LIMA side branch. Abdo et al described 43 cases of presumptive coronary steal published between 1980 and 2005 and found that 72% of the patients derived symptomatic benefit after closure of a significant side branch.3 Fourteen of those patients who derived symptomatic benefit from therapy also demonstrated reduction in ischemia, as assessed by stress testing. Similarly, our patient experienced complete angina relief after LIMA side-branch occlusion.
Whether coronary “steal” through a LIMA side branch can cause angina after CABG remains debatable. Flow via the LIMA side branches occurs mainly during systole, whereas the majority of flow to the coronary target vessel occurs during diastole.6 No significant change in LAD flow or LIMA coronary flow reserve has been demonstrated after balloon occlusion of the LIMA side branches7 or adenosine-induced hyperemia.8 However, there are several reports of anginal improvement and resolution of ischemia on myocardial perfusion imaging after successful occlusion of a large LIMA side branch. Abdo et al described 43 cases of presumptive coronary steal published between 1980 and 2005 and found that 72% of the patients derived symptomatic benefit after closure of a significant side branch.3 Fourteen of those patients who derived symptomatic benefit from therapy also demonstrated reduction in ischemia, as assessed by stress testing. Similarly, our patient experienced complete angina relief after LIMA side-branch occlusion.
Several techniques have been used to occlude a LIMA side branch. Guzon et al9 reviewed the methods utilized in the treatment of 42 patients presenting with angina post-CABG, presumably due to coronary steal. While the majority received percutaneous closure of the LIMA side branch, surgical closure of the side branch with either direct ligation or surgical clipping was utilized in 11 patients. Percutaneous closure is still preferred as it can be achieved with shorter hospitalization, lower cost, and lower procedural risk.10
Though we utilized the Amplatzer vascular plug to achieve occlusion of the branch, closure may also be achieved percutaneously with the use of coil embolization or the implantation of a covered stent across the origin of the LIMA side branch. Multiple coils are usually required while only a single Amplatzer vascular plug is necessary. Utilization of an insufficient number of coils may also result in partial side-branch recanalization.11 The Amplatzer vascular plug can be positioned more accurately and can be retrieved after expansion but before it is released. It is used extensively in the management of peripheral embolizations and aneurysm management, but it is also shown to be efficacious in LIMA grafts. Specifically, it was utilized successfully to occlude a LIMA side branch in patients with refractory angina post-CABG12 and also to occlude the LIMA in a patient in whom the LIMA was inadvertently anastomosed to the anterior interventricular vein.13
Our case highlights 3 important technical issues when attempting to close LIMA side branches. First, LIMA tortuosity may make access to the LIMA side branch challenging. Straightening of the tortuosity through wire and catheter insertion may result in slow flow or complete cessation of flow, which can hinder visualization of the target vessel14 and impede delivery of the occlusive device. In our patient, difficulty in delivery of the Amplatzer vascular plug likely contributed to LIMA side-branch dissection and occlusion. Use of fixed landmarks, such as surgical clips could aid in delivering the occlusion device to the desired location. Second, a long distance may exist between the LIMA ostium and the side-branch ostium, as in our case, further complicating delivery of an Amplatzer plug. In such circumstances, use of radial access or using coils that require a smaller delivery microcatheter may be advantageous. Third, it might be safest to insert a guidewire into the LIMA past the ostium of the side branch to allow prompt treatment of the LIMA if inadvertent injury occurs during attempts to close the side branch.
Long-term follow-up will be important in the event that spontaneous recanalization of the dissected side branch occurs.
References
- Singh RN, Magovern GJ. Internal mammary graft: Improved flow resulting from correction of a steal phenomenon. J Thorac Cardiovasc Surg. 1982;84:146-149.
- Spanos PK, Bisbos AD, Arditis II. Treatment of internal thoracic artery steal syndrome with supraclavicular approach. J Thorac Cardiovasc Surg. 1998;115:464-465.
- Abdo N, Curran PJ, Kumar V, Tobis JM. Coronary steal syndrome with coil embolization of a large LIMA side branch: Radionucleide evidence for reversible ischemia. Catheter Cardiovasc Interv. 2005;66:360-363.
- Kern MJ. Mammary side branch steal: Is this a real or even clinically important phenomenon? Ann Thorac Surg. 1998;66:1873-1875.
- Bauer EP, Bono MC, von Segesser LK, et al. Internal mammary artery anomalies. Thorac Cardiovasc Surg. 1990;38(5):312-315.
- Kern MJ, Bach RG, Donohue TJ, et al. Role of large pectoralis branch artery in flow through a patent left internal mammary artery conduit. Catheter Cardiovasc Diagn. 1995;34:240-244.
- Abhyankar A, Mitchell AS, Bernstein L. Lack of evidence for improvement in internal mammary graft flow by occlusion of side branch. Catheter Cardiovasc Diagn. 1997;42:291-293.
- Luise R, Teodori G, Di Giammarco G. Persistence of mammary artery branches and blood supply to the left anterior descending artery. Ann Thoracic Surg. 1997;63:1759-1769.
- Guzon OJ, Klatte K, Moyer A, et al. Fallacy of thoracic side-branch steal from the internal mammary artery. Catheter Cardiovasc Interv. 2004;61:20-25.
- Ayres RW, Lu C, Benzuly KH, et al. Transcatheter embolization of an internal mammary artery bypass graft sidebranch causing coronary steal syndrome. Catheter Cardiovasc Diagn. 1994;31:301-303.
- Eisenhauer MD, Mego DM, Cambier PA. Coronary steal by IMA bypass graft side-branches. Catheter Cardiovasc Diagn. 1998;45:301-306.
- Weinberg N, French WJ, Shavelle DM. Use of the Amplatzer vascular plug for treatment of coronary steal. Int J Cardiol. 2008;124:109-111.
- Badhey N, Banerjee S, Brilakis ES. Amplatzer vascular plugs for occlusion of a left internal mammary artery graft anastomosed to the anterior interventricular vein. Catheter Cardiovasc Interv. 2010;75:742-747.
- Lichtenwalter C, Banerjee S, Brilakis ES. Dual guide catheter technique for treating native coronary artery lesions through tortuous internal mammary grafts: Separating equipment delivery from target lesion visualization. J Invasive Cardiol. 2010;22:E78-E81.
_____________________________________
From the VA North Texas Healthcare System and University of Texas Southwestern Medical Center, Dallas, Texas.
The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. 1Dr. Moin reports no conflicts of interest regarding the content herein. 2Dr. Banerjee reports speaker honoraria from St. Jude Medical, Medtronic, and Johnson & Johnson, and research support from Boston Scientific and The Medicines Company. 3Dr. Brilakis reports speaker honoraria from St Jude Medical; research support from Abbott Vascular; and salary (spouse is an employee of Medtronic).
Manuscript submitted February 7, 2011, provisional acceptance given March 7, 2011, final version accepted March 15, 2011.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Dallas VA Medical Center (111A), 4500 South Lancaster Road, Dallas, TX 75216. Email: esbrilakis@yahoo.com













