

One-Year Clinical Outcomes of the Hybrid CTO Revascularization Strategy After Hospital Discharge: A Subanalysis of the Multicenter RECHARGE Registry
Abstract: Objectives. Percutaneous coronary intervention (PCI) of chronic total occlusion (CTO) has historically been associated with higher event rates during follow-up. The hybrid algorithm and contemporary wiring and dissection re-entry (DR) techniques can potentially improve long-term outcomes after CTO-PCI. This study assessed the long-term clinical outcomes of the hybrid CTO practice, when applied by operators with varying experience levels. Methods. We examined the 1-year clinical events after hospital discharge of the RECHARGE population, according to technical outcome and final technique. The primary endpoint was major adverse cardiac event (MACE) rate. Centers that provided ≥90% complete 12-month follow-up were included. Results. Follow-up data of 1067 out of 1165 patients (92%) were provided by 13 centers. Mean follow-up duration was 362.8 ± 0.9 days. One-year MACE-free survival rate was 91.3% (974/1067). MACE included death (1.9%; n = 20), myocardial infarction (1.4%; n = 15), target-vessel failure (5.9%; n = 63), and target-vessel revascularization (TVR) (5.5%; n = 59). Non-TVR was performed in 6.7% (n = 71). MACE was significantly in favor of successful CTO-PCI (8.0% vs 13%; P=.04), even after adjusting for baseline differences (adjusted hazard ratio, 0.59; 95% confidence interval, 0.36-0.98; P=.04). Other events, including individual MACE components, were comparable with respect to technical outcome and final technique (DR vs non-DR techniques). Conclusions. The use of the hybrid algorithm with contemporary techniques by moderate to highly experienced operators for CTO-PCI is safe and associated with a low 1-year event rate. Successful procedures are associated with a better MACE rate. DR techniques can be used as first-line strategies alongside intimal wiring techniques without compromising clinical outcomes.
J INVASIVE CARDIOL 2018;30(2):62-70. Epub 2017 November 15.
Key words: percutaneous coronary intervention, chronic total occlusion, follow-up
Historically, it is known that percutaneous coronary intervention (PCI) of chronic total occlusion (CTO) lesions is associated with higher event rates during follow-up compared to non-CTO interventions. Higher CTO complexity, unsuccessful CTO-PCI, the use of (older) dissection and re-entry (DR) techniques, and the use of bare-metal stents are known to be associated with a higher event risk during follow-up.1-4 However, positive improvements have already been made with the development of new and better materials and techniques, such as device-based “controlled” antegrade DR (ADR) and retrograde DR (RDR).5-8
The hybrid algorithm has the potential to further improve long-term outcomes after CTO-PCI. The hybrid algorithm emphasizes on the improvement of procedural success and efficiency by applying all feasible contemporary antegrade and retrograde wiring and DR techniques in the most optimal way.9 Studies validating the hybrid algorithm demonstrated improved procedural outcomes for highly and moderately experienced operators.10-12 A recent multicenter report demonstrated improved 1-year outcomes after successful hybrid CTO-PCI, both with wiring and DR techniques.13 Yet, extrapolation of these findings might be limited, as these results focused strictly on successful procedures, which were performed by seasoned operators. Two other recent papers demonstrated improved long-term outcomes with contemporary DR techniques. However, these were retrospective data,14,15 and thus might not be representative of the broader community.
Recently, the in-hospital results of RECHARGE (the European REgistry of CrossBoss and Hybrid procedures in FrAnce, the NetheRlands, BelGium, and UnitEd Kingdom) demonstrated that the hybrid algorithm and current antegrade and retrograde techniques for CTO-PCI are effective and safe to apply for the broader community, including operators with different experience levels.10 Given this difference in experience levels, this RECHARGE substudy focuses on assessing the real-world clinical outcomes of patients treated via the hybrid algorithm and contemporary techniques. To do so, we prospectively examined the 1-year clinical events after hospital discharge according to technical outcomes and evaluated 1-year outcomes according to the use of DR or non-DR techniques.
Methods
Study population. Between January 2014 and October 2015, seventeen centers from Belgium, France, the Netherlands, and the United Kingdom prospectively and consecutively collected data on 1253 hybrid CTO-PCIs performed in 1165 patients.10 All operators are trained in each aspect of CTO-PCI and apply antegrade, retrograde, and ADR techniques according to the hybrid algorithm. During the inclusion period, the mean number of annually performed CTO procedures/operator was 64. The study was granted ethical permission and all patients gave written informed consent according to local institutional guidelines and those of the American Physiological Society.
Study design. The RECHARGE study design and procedure have been previously described.10 Clinical, angiographic, procedural, outcome, and follow-up data (post discharge) were collected using a web-based reporting system (OpenClinica Community, LCC). For this substudy, 1-year follow-up data on clinical major adverse cardiac events (MACE) and complications were collected at prespecified times (1, 3, 6, and 12 months). Centers were included if they provided complete 1-year follow-up of ≥90%. In the absence of any events, the maximum available follow-up was provided according to the prespecified times.
Study definitions and endpoints. A CTO was defined as a lesion of a native coronary artery that exhibited antegrade Thrombolysis in Myocardial Infarction (TIMI) 0 flow for >3 months. CTO complexity was graded using the Japanese CTO (J-CTO) score, prospective global registry for the study of CTO intervention (PROGRESS) score, and RECHARGE score.16-18 Demographic and angiographic characteristics have been previously defined. After hospital discharge, 1-year MACE included death, clinically based myocardial infarction (MI), target-vessel failure (TVF; ie, the vessel was restenosed/reoccluded at follow-up with or without intervention), and target-vessel revascularization (TVR) via PCI or coronary artery bypass graft (CABG) surgery, and were counted mutually exclusively. TVR was defined as the need for repeat intervention, including PCI (ballooning ± stenting; after TVF or if the operator decided to recover any side branches lost during the index procedure), or bypass graft surgery on the target vessel. Complications included major or life-threatening bleeding, major vascular complication, acute renal failure, stroke, and non-TVR interventions. Adverse events were analyzed patient-wise using the index procedure. The index procedure was defined as the first inclusion (ie, treatment of the first CTO lesion). Patients could be included multiple times in the registry, either for a reattempt of the same CTO lesion, a secondary CTO lesion treated at a later time (= non-TVR), or a second CTO lesion treated during the same procedure. In case of the latter, treatment of the first CTO lesion was considered the main index procedure. If any revascularization was needed for the second CTO lesion during follow-up, it was considered a non-TVR. For each patient, the follow-up period was counted from the index procedure date onward, excluding any in-hospital events previously described.10
The primary goal of this substudy was to determine the rate of adverse events at 1-year follow-up according to technical outcome, in patients who were treated according to the hybrid algorithm. The secondary endpoint included the assessment of 1-year outcomes according to the applied strategies (antegrade-wire escalation [AWE], retrograde wire escalation [RWE], ADR, and RDR).
Statistical analyses. Baseline, angiographic, and procedural data were analyzed using descriptive statistics. Numerical values were expressed as mean ± standard deviation or median (interquartile range) as appropriate, while categorical variables were expressed as percentages. Normality was assessed using the Shapiro-Wilk statistic. Comparisons between groups were performed using Pearson’s Chi-square tests for categorical variables and the independent Student’s t-test, one-way analysis of variance, Mann-Whitney U-test, or Kruskal-Wallis H-test for continuous variables, as appropriate. The Kaplan-Meier method was used to construct survival curves, with the log- rank test used for comparison among groups. Cox regression analysis was used to determine independent predictors for the primary outcome. Univariate factors with a P<.10 were forwarded in the multivariate model. Statistical significance was always set at a two-tailed probability level of <.05. All statistical analyses were carried out using SPSS Statistics v. 22 (IBM SPSS, Inc).
rank test used for comparison among groups. Cox regression analysis was used to determine independent predictors for the primary outcome. Univariate factors with a P<.10 were forwarded in the multivariate model. Statistical significance was always set at a two-tailed probability level of <.05. All statistical analyses were carried out using SPSS Statistics v. 22 (IBM SPSS, Inc).
Results
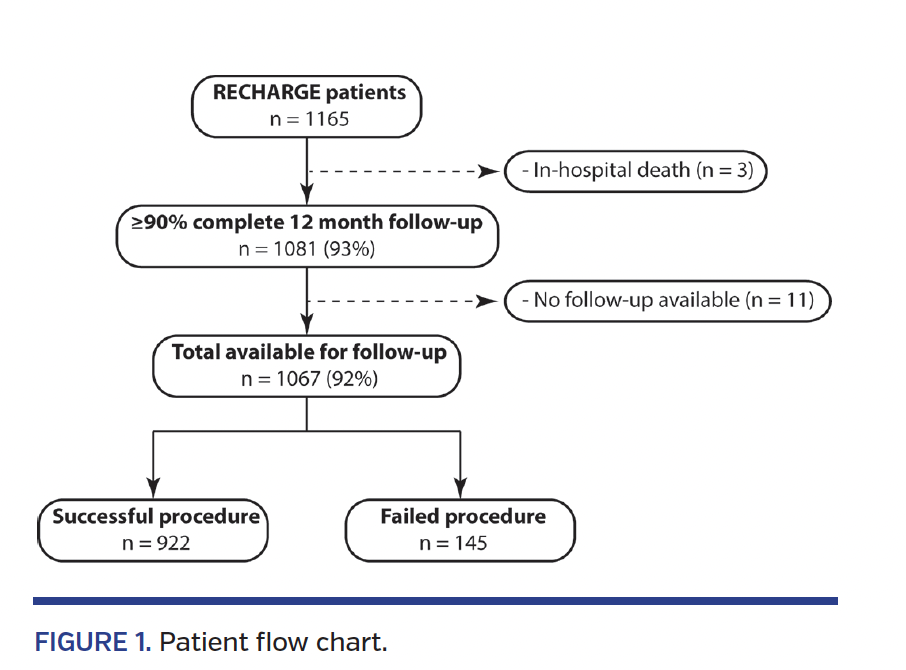
Study population. Follow-up data (≥90% complete follow-up per center) up to 12 months were provided by 13 centers, resulting in a total of 1081 out of 1165 patients (93%) (Figure 1). Three patients were excluded due to postprocedural death (ie, in-hospital event).10 No follow-up data were available for 14 patients; therefore, 1067 out of 1165 patients (92%) were included in this analysis.
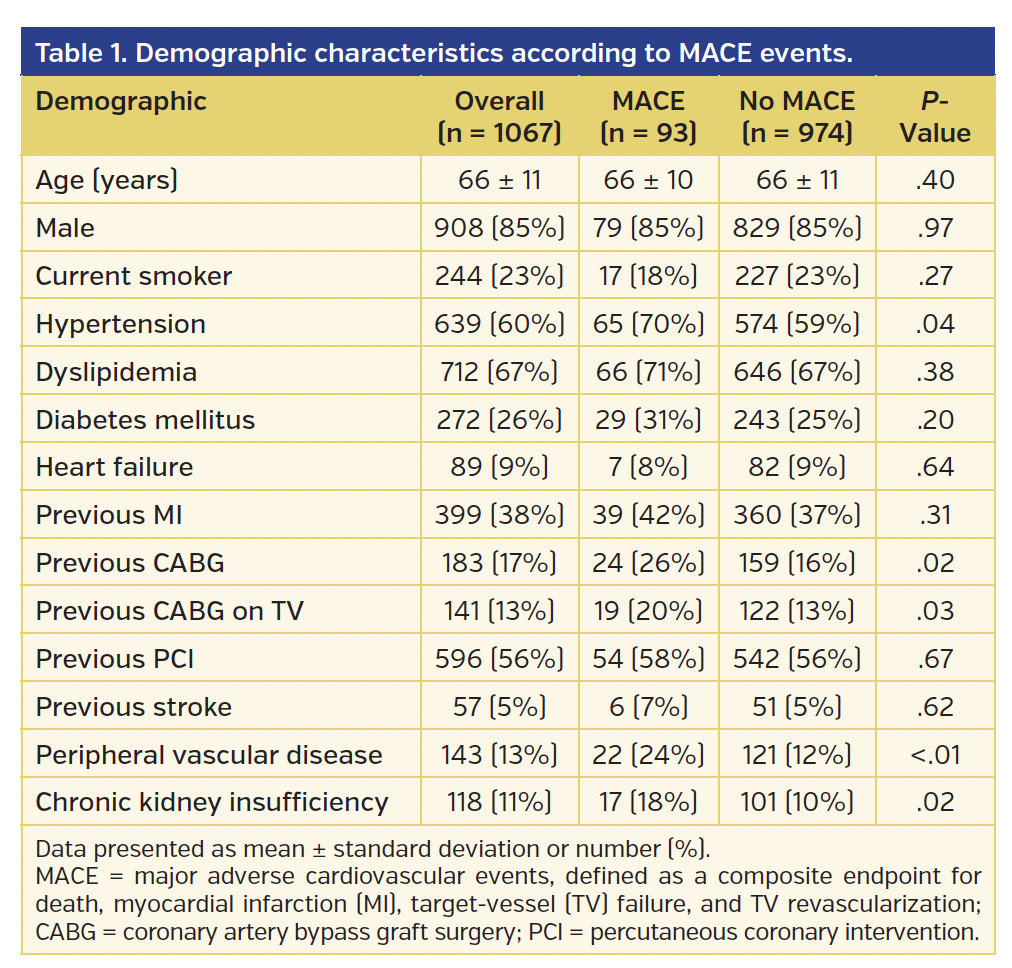
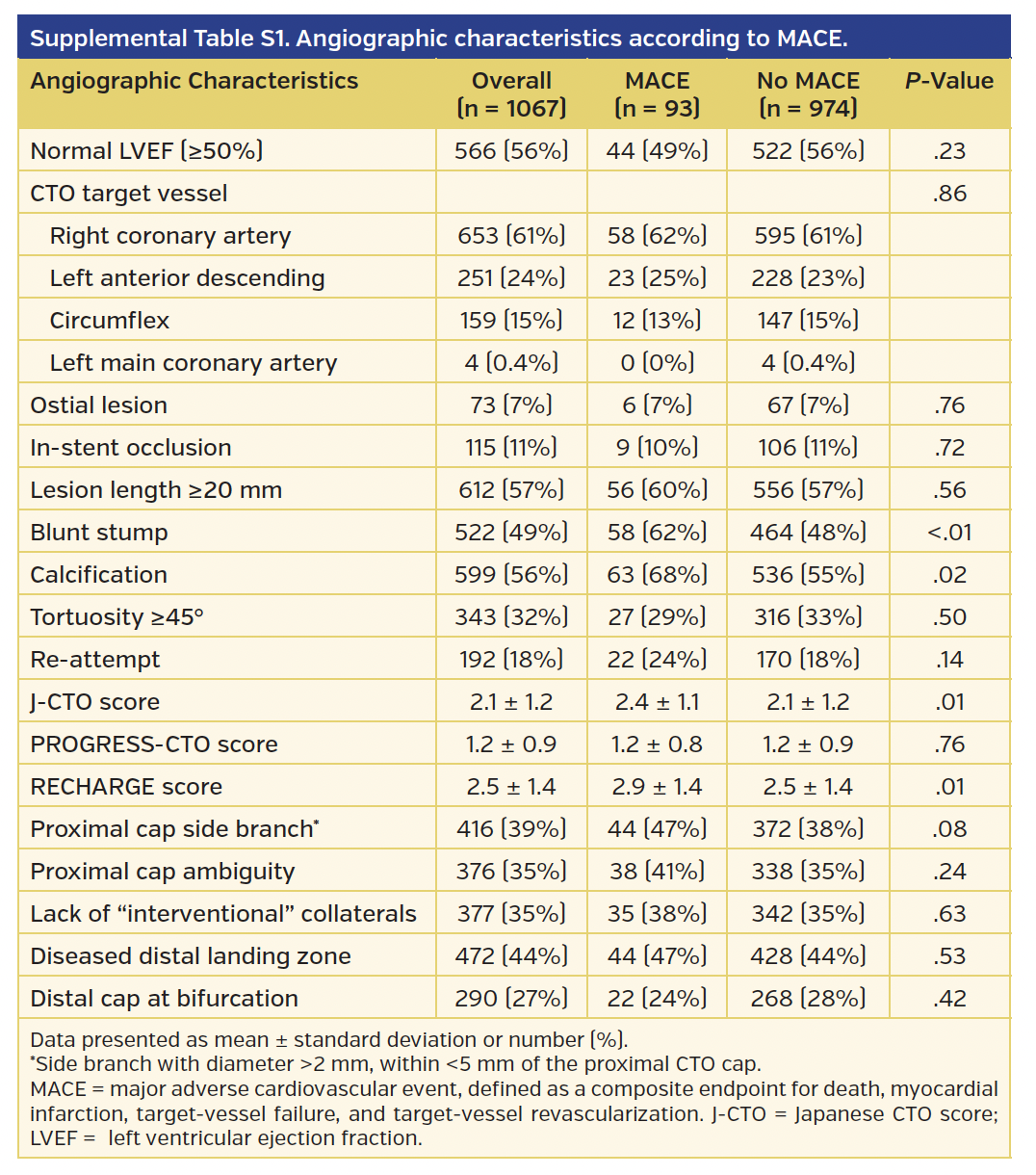
Baseline demographic characteristics (Table 1) are stratified according to the prevalence of MACE during 1-year follow-up. In the MACE group (n = 93), significantly more patients suffered from hypertension, peripheral vascular disease, chronic kidney insufficiency, and a previous history of bypass surgery, as well as bypass surgery on the CTO target vessel. Similarly, angiographic characteristics were stratified according to the prevalence of MACE events (Supplementary Table S1). More than one-half of the patients (56%) had a normal left ventricular ejection fraction, and the most frequently treated CTO target vessel was the right coronary artery (61%), followed by the left anterior descending (24%), circumflex (15%), and left main (0.4%) coronary arteries. No differences were present between MACE and non-MACE patients for these parameters (P=.23 and P=.86, respectively). Angiographic lesion characteristics were distributed similarly between groups, except for a blunt proximal cap stump (62% vs 48%; P<.01) and the presence of calcification (68% vs 55%; P=.02). In addition, the J-CTO (2.4 ± 1.1 vs 2.1 ± 1.2; P=.01) and RECHARGE lesion complexity scores (2.9 ± 1.4 vs 2.5 ± 1.4; P=.01) were considerably higher in the MACE group.
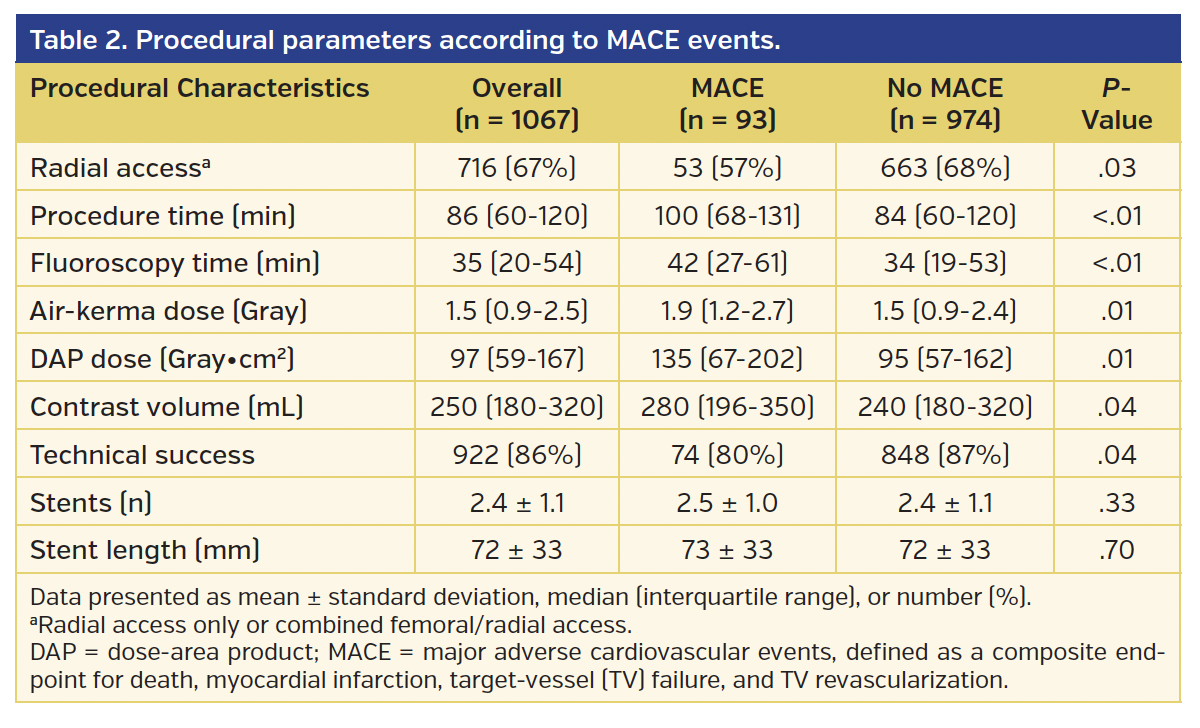
Outcomes and procedural parameters. Procedural parameters are given for the overall study group, as well as stratified according to the prevalence of MACE (Table 2). Overall technical success corresponded to 86% and was significantly higher in the absence of any MACE during follow-up (80% vs 87%; P=.04). In agreement with this finding are the procedural parameters, which are substantially lower in the non-MACE group. Of note, the number of implanted stents and the average total stent length were not significantly different between the two groups.
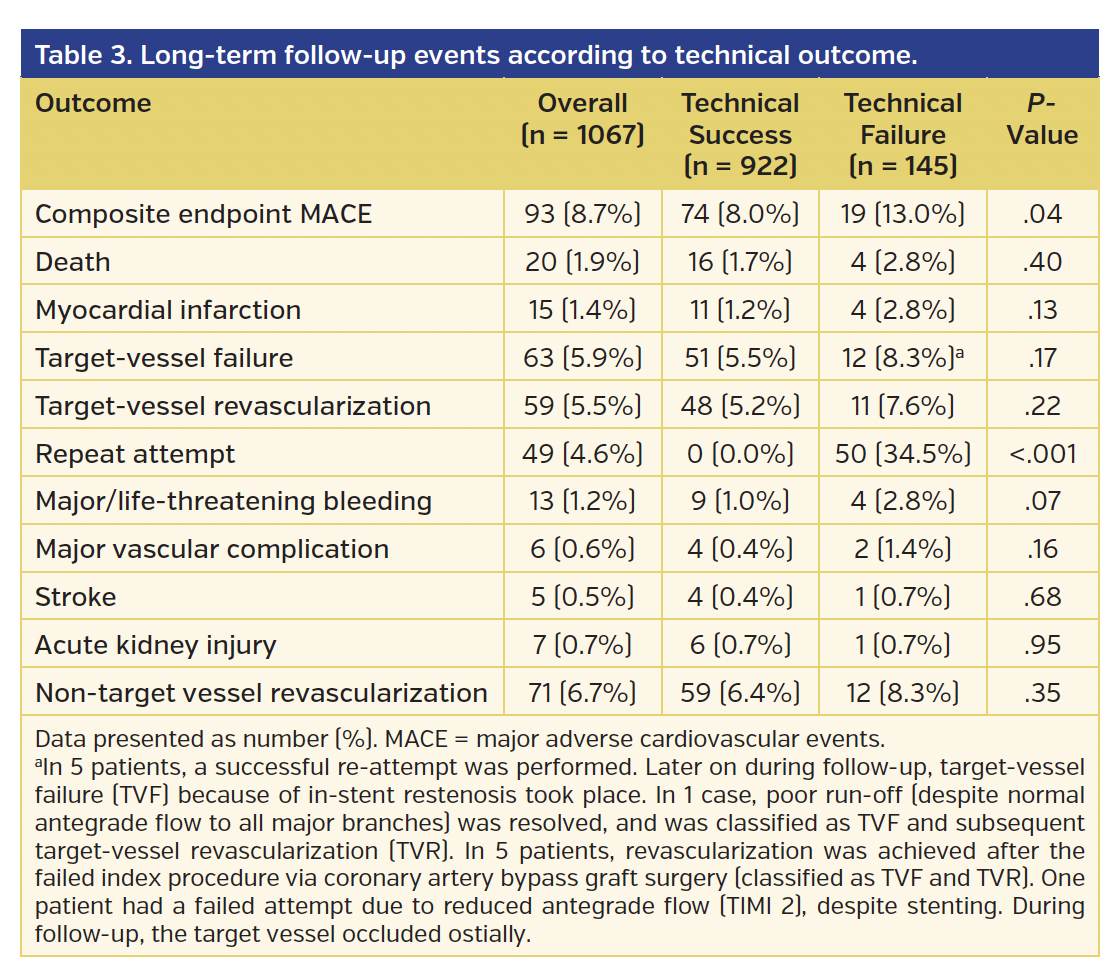
One-year outcomes and technical success. The mean duration of follow-up was 362.8 ± 0.9 days. Overall, 1-year MACE-free survival corresponded to 91.3% (Table 3). Death took place in 20 patients (1.9%); 4 deaths were due to a certain cardiac event, 10 were due to an uncertain cardiac event, and 6 were due to an unknown cause. TVF took place in 63 patients (5.9%), of which 5 (8.0%) were due to in-stent occlusion. Other reasons included malapposition and optimization of the stent (n = 5), stent recoil (n = 1), resolving poor run-off (n = 1), elective non-TLR (n = 3), and picking up non-revascularized side branches (n = 5). In 5 patients, bypass graft surgery was performed after failure of the index procedure. TVR was performed in 59 patients (5.5%), either via PCI (n = 53; 90%) or CABG (n = 6; 10%). An MI occurred in 15 patients (1.4%); 4 were ST-elevation MIs and 11 were non-ST elevation MIs, of which 2 were due to TVF and 10 were due to non-TVF. In 1 case, arrhythmias took place, leading to a non-STEMI and sudden cardiac death (angiography showed no ischemic cause). The patient received a defibrillator and fully recovered. In the remaining 2 patients, no clear cause could be identified. Non-TVR was performed in 71 patients (6.7%), either via PCI (n = 65; 92%) or CABG (n = 6; 8%). Of these, non-TVR via PCI was performed for the treatment of a second CTO lesion during follow-up in 19 out of 65 patients (29%).
Other events included major or life-threatening bleeding, major vascular complication, stroke, and acute kidney injury. Major (n = 10) and life-threatening bleeding (n = 3) occurred in 1.2%. Six patients had gastrointestinal bleeding; 2 patients underwent repeat revascularization attempts that were complicated by tamponade requiring drainage and additional left main stenting in 1 case and a hemoglobin drop and pericarditis in the other; 1 patient suffered a retroperitoneal bleed 1 day post discharge and required transfusion; 1 patient had a non-TVR procedure, which resulted in a wire perforation and tamponade, necessitating emergency bypass surgery; 1 major bleed was associated with contrast-induced nephropathy (as below); and 2 patients had a major bleed for unknown reason. Major vascular complications occurred in 6 patients, of which 4 took place within 10 days post index procedure (post discharge), and 1 took place within 1 month. Five patients had a stroke. Acute kidney injury occurred in 7 patients (0.7%): in 3 patients after index CTO-PCI (post discharge), of which 1 was related to contrast-induced nephropathy and associated with a major bleed; in 1 patient after non-TVR performed during follow-up (patient also had major bleeding, most likely related to the gastrointestinal tract); and in 3 patients for unknown reason (but likely from acute kidney failure). However, concerning the latter, 1 patient underwent a non-TVR procedure 20 days before.
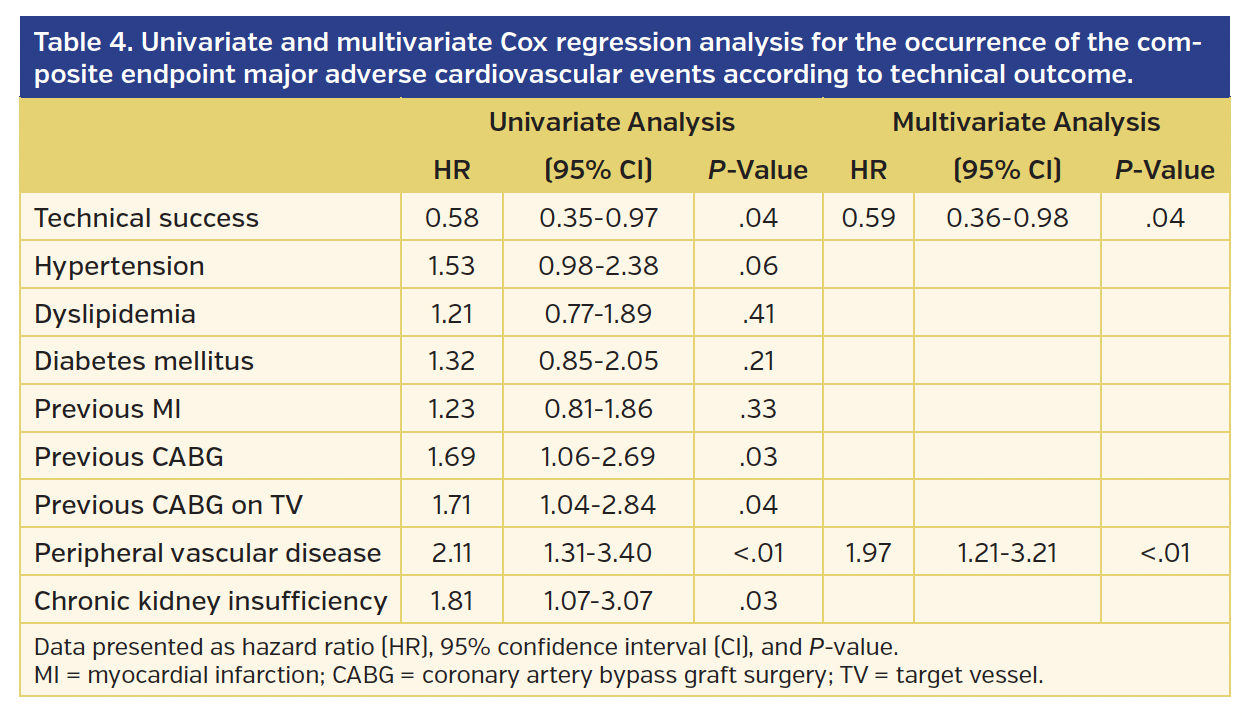
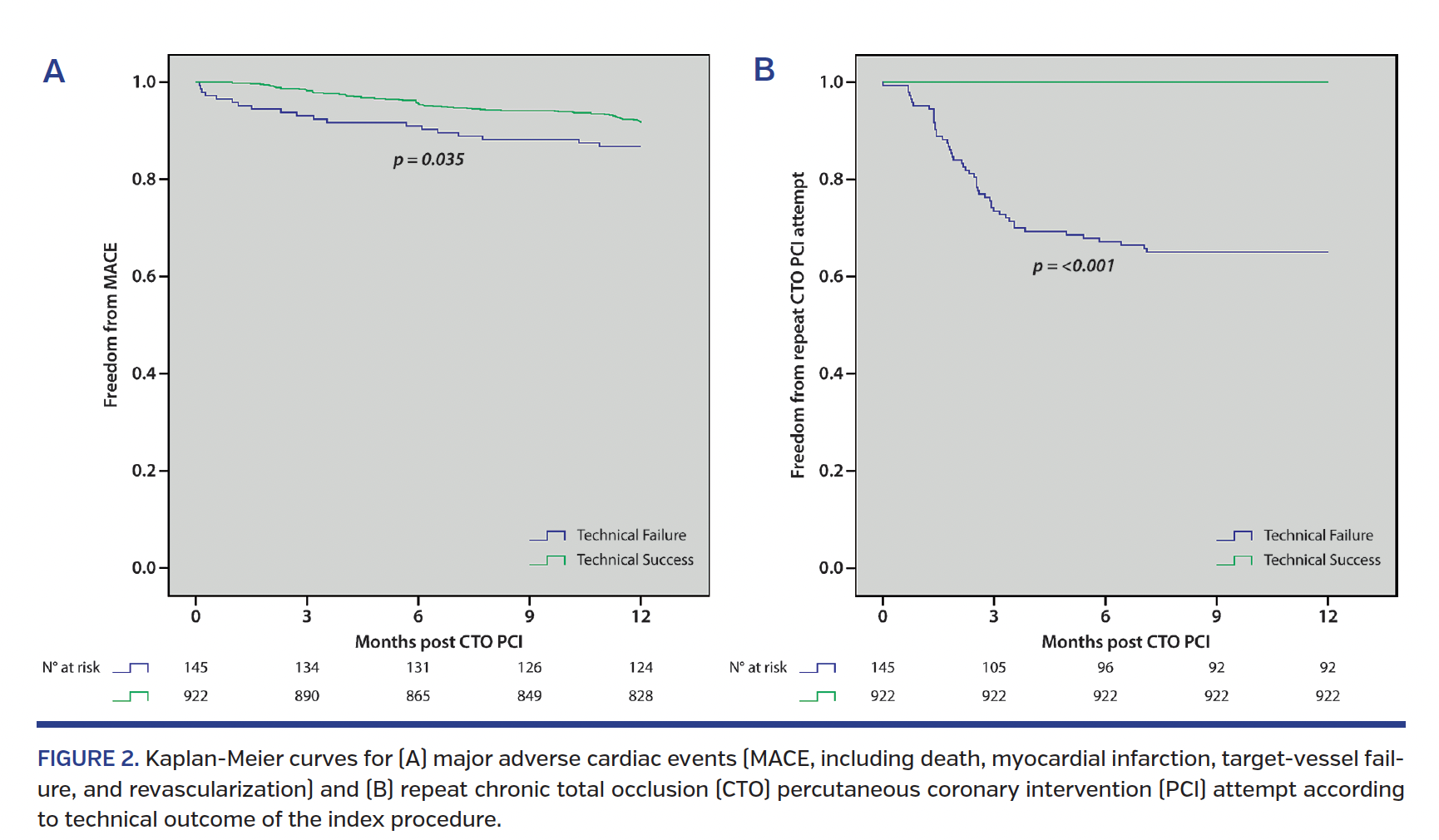
Components of the MACE endpoint were not significantly different between successful and unsuccessful procedures. On the contrary, the composite MACE endpoint itself was significantly in favor of the successful group (8.0% vs 13%; P=.04) (Figure 2), even after adjusting for baseline differences (adjusted hazard ratio, 0.59; 95% confidence interval, 0.36-0.98; P=.04) (Table 4). In addition, the presence of peripheral artery disease was a negative predictor for MACE (adjusted hazard ratio, 1.97; 95% confidence interval, 1.21-3.21; P<.01). Repeat revascularization attempts were performed in 49 patients (4.6%) after technical failure of the index procedure. Although no reattempts could be performed after a successful procedure, this resulted in an important probability value (0% vs 34.5%; P<.001) when comparing both groups (Figure 2).
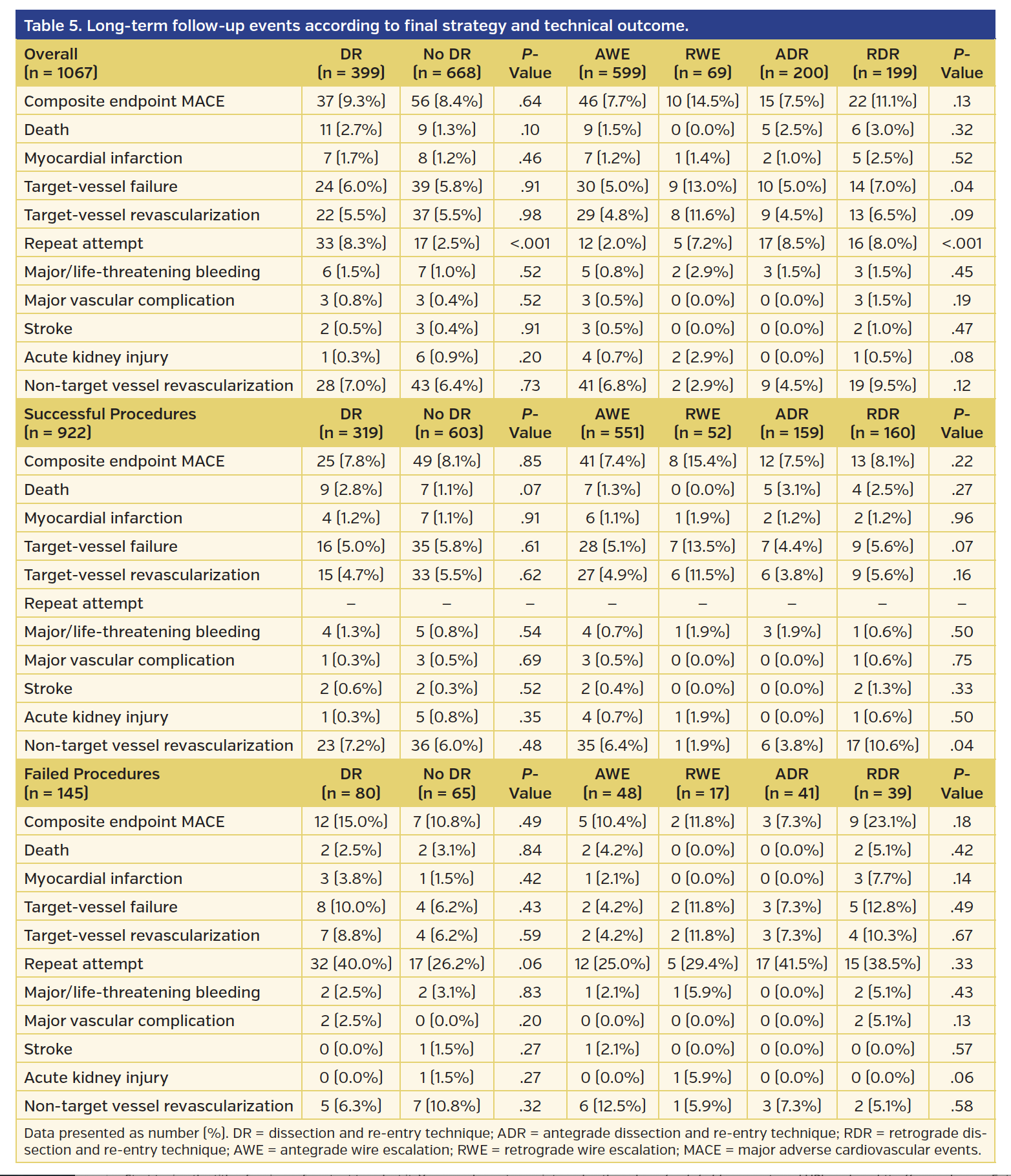
One-year outcomes and techniques. As a secondary endpoint, differences concerning 1-year outcomes between patients were assessed according to the final applied technique (Table 5). Overall (successful + failed procedures), the only statistically significant difference was present for TVF, driven by the higher rate within procedures with RWE as a final applied strategy (AWE 5.0%, RWE 13.0%, ADR 5.0%, RDR 7.0%; P=.04). However, this statistical difference was not present when comparing patients treated with a final DR (ADR or RDR) and non-DR (AWE or RWE) technique (6.0% vs 5.8%; P=.91). Moreover, overall, no other statistical differences were observed for MACE or any other event, except for repeat attempts for the same reason as above. Similarly, when stratifying the results for successful and unsuccessful procedures separately, no differences in 1-year outcome events were present between DR and non-DR groups. However, a higher degree of non-TVR took place when a final successful RDR technique was applied (AWE 6.4%, RWE 1.9%, ADR 3.8%, RDR 10.6%; P=.04).
Discussion
With this substudy of the RECHARGE registry, we sought to determine the long-term efficacy and safety of hybrid CTO-PCI and its techniques post discharge. Follow-up data were available for 1067 patients, meaning our cohort is currently the largest study to date to report on the 1-year outcomes after contemporary hybrid CTO-PCI to our knowledge. The main findings are: (1) after hospital discharge, a clinical MACE rate <10% was observed after 12 months; (2) compared to failed CTO procedures, a successful hybrid CTO-PCI was associated with lower MACE at 1 year; and (3) the long-term outcomes of subintimal DR techniques are comparable to true-lumen wiring techniques.
Overall study outcomes. Our study demonstrated a favorable overall MACE rate of 8.7% at 1 year post discharge. Furthermore, we report a low TVF rate (5.9%) and low TVR rate (5.5%). These results are comparable with the most recent (and previously largest) published study from Wilson et al, who reported an 8.6% MACE rate (with MACE defined as the composite endpoint of death, MI, and unscheduled TVR) and a TVR rate of 5.0%.13 However, they reported on successful procedures only. Similar to their study, our results were achieved in a complex CTO population (J-CTO score, 2.1 ± 1.2; RECHARGE score, 2.5 ± 1.4). Yet, previous literature demonstrated that lesion complexity was associated with worse long-term outcomes (ie, TLR).19 Both registries do not have systematic angiographic follow-up, which would result in higher TVF/TVR rates. This is a concern especially in CTO patients, where symptoms can be absent or non-anginal (both at baseline in terms of silent ischemia/dyspnea and at follow-up).
In our patient cohort, J-CTO and RECHARGE complexity scores were significantly higher in the MACE group vs the non-MACE group. Most likely, this difference is driven by the significantly greater prevalence of a blunt proximal cap and calcification in the MACE group (as opposed to lesion length, as reported by Wilson et al). Apart from CTO complexity, a medical history of bypass graft surgery (whether or not on the CTO target vessel) was also substantially more prevalent in the MACE group. This group of patients has more comorbidities, more atherosclerotic burden, and higher CTO lesion complexity, and therefore carries a greater risk for procedural failure and adverse events during follow-up.10,18,20-22 Although Toma et al demonstrated that the relative survival benefit after successful CTO-PCI was independent from a history of CABG, Pereg et al showed the presence of a CTO both preoperatively and post surgery was associated with adverse long-term clinical outcomes.23,24 Table 2 illustrates significantly higher procedural parameters and a lower success rate in the MACE cohort, reflecting higher lesion complexity. Stent implantation characteristics (ie, number and length), however, were not significantly different between the two groups.
One-year outcomes and technical success. For the primary endpoint, 1-year adverse events were stratified according to technical outcome. The composite follow-up endpoint of MACE rate was statistically in favor of successful procedures (8.0% vs 13%; P=.04), which is slightly lower compared to the United Kingdom report (8.6%). Nevertheless, lesions were overall more complex in their cohort (J-CTO score: 2.1 ± 1.2 vs 2.4 ± 1.4).
On the other hand, individual MACE components (ie, death, MI, TVF, and TVR) were not statistically different between successful and failed procedures, nor were any other adverse events (apart from repeat revascularization attempts). The duration of follow-up in this substudy might be inadequate to show significant differences between successful and unsuccessful CTO-PCIs, given that very late-term adverse events could not have taken place yet. Also, systematic screening for residual/recurrent ischemia was not mandatory. However, after adjustment for baseline differences, MACE remained independently associated with technical failure (adjusted hazard ratio, 0.59; P=.04). A recent meta-analysis has demonstrated that successful CTO-PCI is associated with improved clinical outcomes, including mortality, MI, CABG, stroke, and angina (but not TVR) during a weighted mean follow-up of 3.11 years,25 although a randomized trial was negative (DECISION).26 However, this trial has important study limitations.
The above-mentioned benefits are multifactorial: (1) successful CTO-PCI results in more complete revascularization, which has previously been shown to result in lower mortality: residual Syntax score after revascularization is a negative prognostic marker and occurs more frequently in patients with CTO;27 (2) successful CTO recanalization can potentially protect better against future events (the “double jeopardy” concept) and improve outcomes afterward;28 (3) the ischemic burden is reduced after successful CTO-PCI,29 as is the risk for arrhythmias;30 and (4) improvements in left ventricular function31-34 and exercise capacity are related with successful CTO-PCI.35 Apart from this, patients in whom procedures failed commonly have higher clinical risk characteristics, as shown previously, among others in our RECHARGE registry.10,25 In this study, the presence of peripheral vascular disease increased the risk for MACE by a factor of 2 (adjusted hazard ratio, 1.97; P<.01). This is further supported by the recently presented randomized EuroCTO trial,36 which showed better quality-of-life for patients receiving CTO-PCI, compared with optimal medical therapy.
Repeat revascularization attempts were performed in one-third of the patients in whom the index procedure failed. Since repeat revascularization attempts are not applicable in cases of successful CTO-PCI, comparing survival curves for successful and unsuccessful cases is highly significant. Although such analyses are biased in favor of successful procedures, the corresponding Kaplan-Meier graph illustrates the need for reintervention in these patients (mostly operator driven apart from clinically driven), which is performed mainly during the first 3 months of follow-up. In addition, the need for reintervention is indicative of higher clinical risk characteristics and lesion complexity, the latter often necessitating the use of more complex techniques, which historically carry a greater risk of complications. In our cohort, repeat attempt on the target vessel was associated with 1 major and 1 life-threatening bleed post procedure.
One-year outcomes and techniques. Previously, we demonstrated that the use of DR techniques (including ADR and RDR) was associated with higher lesion complexity.10,11 Upon higher complexity, a DR technique is needed more often to obtain success, while antegrade and/or retrograde wiring strategies fail to do so. Although early subintimal strategies were associated with a greater risk of adverse events (mainly TVR or TLR), we found no statistically significant differences between patients treated with a final DR or non-DR technique within successful procedures, failed procedures, or overall.
This apparent discrepancy can potentially be explained as follows. Early practice of subintimal stenting was performed using the STAR, mini-STAR, and LAST techniques for antegrade subintimal revascularization, and CART technique for retrograde subintimal revascularization. However, these techniques had a low success rate, and in the case of antegrade subintimal techniques, often resulted in poor distal run-off due to unpredictability regarding the re-entry site and loss of side branches. Not surprisingly, early data demonstrated disappointing mid-term and long-term outcomes,1-3 which has been used as an argument against its use by non-supporters of the technique. The development of modern techniques, including reverse CART and controlled ADR (primarily using CrossBoss and Stingray) improved clinical outcomes, similar to conventional intimal wiring strategies.5-8,13,37 In RECHARGE, the (mini-)STAR and LAST techniques occurred rarely, but were typically inadvertent and close to the distal cap of the occlusion.37 Recent investigations by Azzalini et al confirm these improved outcomes, as they performed a direct comparison between old and new DR techniques, demonstrating a decreased risk of MACE with contemporary DR techniques.14,15 Moreover, the J-PROCTOR registry also showed the TVR rate between intimal and subintimal tracking was comparable, in accordance with our study results.38
Although event rates were comparable between final DR and non-DR techniques, a borderline significant difference in overall TVF was found between individual antegrade and retrograde wiring and DR techniques, most likely as a result of a higher rate within RWE techniques. In our study, final retrograde techniques (RWE + RDR) were numerically associated with the highest adverse event rate, similar to the results of Wilson et al.13 Higher TLR rates have been reported before, yet these were hypothesized to relate to longer stent length, which is often mandated, rather than the retrograde technique itself.39,40 Despite the fact that stent length has been identified as an important factor in the risk for in-stent restenosis and reocclusion, stent fracture, and thrombosis,41 there were no statistical differences concerning stent characteristics within the MACE and no-MACE groups in our study. Therefore, one might speculate that the (mainly numerical) higher event rate within retrograde cases is related to the greater complexity of these lesions and worse baseline characteristics, as described previously, as well as an increase of periprocedural acute myocardial infarction and tamponade.10,13 Wilson et al previously noted an association between severe disease proximal and distal to the CTO. While this can result in an overall increase in stent length, it also reflects the fact that there is a higher disease burden.13 This might argue for the use of more antegrade strategies, if feasible. Alternatively, the 1-year follow-up point is incapable of excluding very late adverse events, which might result in greater and potentially important TVF and TVR rate differences between intimal wiring and subintimal DR techniques.
Study limitations. The main limitations of the RECHARGE study have been described previously.10 First, it is an observational study, and is thus susceptible to the effects of unidentified confounders. Second, clinical events during follow-up were operator reported, and there was no central independent adjudication of these events. Nonetheless, all reported clinical events were reviewed by two authors (JM, JD), and consensus regarding the classification of these adverse events was obligatory. Third, not all centers provided follow-up, and follow-up was not 100%. Thus, the adverse event rate could potentially be higher. Moreover, routine imaging was not systematically performed, which could have resulted in an under-estimation of clinical events (eg, asymptomatic restenosis/reocclusion). Last, the rate of DR techniques applied might have been higher, as unintentional subintimal dissection may occur during the application of AWE or RWE techniques. This is usually detected by intravascular ultrasound, which was utilized to a low extent in our registry (12%).
Conclusion
The use of hybrid CTO-PCI by moderate to highly experienced operators is safe and associated with a low 1-year event rate. Successful procedures are associated with a better MACE rate. Application of DR techniques according to the hybrid approach resulted in good long-term outcomes, comparable to wire-escalation techniques, suggesting they can be used as first-line strategies alongside these intimal techniques.
Acknowledgments. We would like to acknowledge the RECHARGE Investigators for their contributions to this work: Alan J. Bagnall, MD, PhD; Mohaned Egred, MD; Paul Kelly, MD; Elliot J. Smith, MD, FRCP; and Julian W. Strange, MD.
References
1. Valenti R, Vergara R, Migliorini A, et al. Predictors of reocclusion after successful drug-eluting stent-supported percutaneous coronary intervention of chronic total occlusion. J Am Coll Cardiol. 2013;61:545-550.
2. Godino C, Latib A, Economou FI, et al. Coronary chronic total occlusions: mid-term comparison of clinical outcome following the use of the guided-STAR technique and conventional anterograde approaches. Catheter Cardiovasc Interv. 2012;79:20-27.
3. Galassi AR, Boukhris M, Tomasello SD, et al. Long-term clinical and angiographic outcomes of the mini-STAR technique as a bailout strategy for percutaneous coronary intervention of chronic total occlusion. Can J Cardiol. 2014;30:1400-1406.
4. Suero JA, Marso SP, Jones PG, et al. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries: a 20-year experience. J Am Coll Cardiol. 2001;38:409-414.
5. Mogabgab O, Patel VG, Michael TT, et al. Long-term outcomes with use of the CrossBoss and Stingray coronary CTO crossing and re-entry devices. J Invasive Cardiol. 2013;25:579-585.
6. Amsavelu S, Christakopoulos GE, Karatasakis A, et al. Impact of crossing strategy on intermediate-term outcomes after chronic total occlusion percutaneous coronary intervention. Can J Cardiol. 2016;32:1239.e1231-1239.e1237.
7. Rinfret S, Ribeiro HB, Nguyen CM, Nombela-Franco L, Ureña M, Rodés-Cabau J. Dissection and re-entry techniques and longer-term outcomes following successful percutaneous coronary intervention of chronic total occlusion. Am J Cardiol. 2014;114:1354-1360.
8. Bijuklic K, Schwencke C, Schofer J. Long-term major adverse cardiac and cerebrovascular events (MACCE) rate: comparison of retrograde and antegrade recanalization of chronic total coronary occlusions. Wien Klin Wochenschr. 2017;129:243-250.
9. Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5:367-379.
10. Maeremans J, Walsh S, Knaapen P, et al. The hybrid algorithm for treating chronic total occlusions in Europe: the RECHARGE registry. J Am Coll Cardiol. 2016;68:1958-1970.
11. Wilson WM, Walsh SJ, Yan AT, et al. Hybrid approach improves success of chronic total occlusion angioplasty. Heart. 2016;102:1486-1493.
12. Christopoulos G, Karmpaliotis D, Alaswad K, et al. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int J Cardiol. 2015;198:222-228.
13. Wilson WM, Walsh SJ, Bagnall A, et al. One-year outcomes after successful chronic total occlusion percutaneous coronary intervention. Catheter Cardiovasc Interv. 2017 Mar 15 (Epub ahead of print).
14. Azzalini L, Dautov R, Brilakis ES, et al. Impact of crossing strategy on mid-term outcomes following percutaneous revascularisation of coronary chronic total occlusions. EuroIntervention. 2017;13:978-985.
15. Azzalini L, Dautov R, Brilakis ES, et al. Procedural and longer-term outcomes of wire- versus device-based antegrade dissection and re-entry techniques for the percutaneous revascularization of coronary chronic total occlusions. Int J Cardiol. 2017;231:78-83.
16. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4:213-221.
17. Christopoulos G, Kandzari DE, Yeh RW, et al. Development and validation of a novel scoring system for predicting technical success of chronic total occlusion percutaneous coronary interventions: the PROGRESS CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention) score. JACC Cardiovasc Interv. 2016;9:1-9.
18. Maeremans J, Spratt JC, Knaapen P, et al. Towards a contemporary, comprehensive scoring system for determining technical outcomes of hybrid percutaneous chronic total occlusion treatment: the RECHARGE score. Catheter Cardiovasc Interv. 2017 May 4 (Epub ahead of print).
19. Tanaka H, Morino Y, Abe M, et al. Impact of J-CTO score on procedural outcome and target lesion revascularisation after percutaneous coronary intervention for chronic total occlusion: a substudy of the J-CTO registry (Multicentre CTO Registry in Japan). EuroIntervention. 2016;11:981-988.
20. Christopoulos G, Menon RV, Karmpaliotis D, et al. Application of the “hybrid approach” to chronic total occlusions in patients with previous coronary artery bypass graft surgery (from a contemporary multicenter US registry). Am J Cardiol. 2014;113:1990-1994.
21. Michael TT, Karmpaliotis D, Brilakis ES, et al. Impact of prior coronary artery bypass graft surgery on chronic total occlusion revascularisation: insights from a multicentre US registry. Heart. 2013;99:1515-1518.
22. Teramoto T, Tsuchikane E, Matsuo H, et al. Initial success rate of percutaneous coronary intervention for chronic total occlusion in a native coronary artery is decreased in patients who underwent previous coronary artery bypass graft surgery. JACC Cardiovasc Interv. 2014;7:39-46.
23. Toma A, Stähli BE, Gick M, et al. Long-term follow-up of patients with previous coronary artery bypass grafting undergoing percutaneous coronary intervention for chronic total occlusion. Am J Cardiol. 2016;118:1641-1646.
24. Pereg D, Fefer P, Samuel M, et al. Long-term follow-up of coronary artery bypass patients with preoperative and new postoperative native coronary artery chronic total occlusion. Can J Cardiol. 2016;32:1326-1331.
25. Christakopoulos GE, Christopoulos G, Carlino M, et al. Meta-analysis of clinical outcomes of patients who underwent percutaneous coronary interventions for chronic total occlusions. Am J Cardiol. 2015;115:1367-1375.
26. Park SJ. Drug-eluting stent versus optimal medical therapy in patients with coronary chronic total occlusion: DECISION CTO randomized trial. Presented at ACC 2017. March 18, 2017. Washington, DC.
27. Garcia S, Sandoval Y, Roukoz H, et al. Outcomes after complete versus incomplete revascularization of patients with multivessel coronary artery disease: a meta-analysis of 89,883 patients enrolled in randomized clinical trials and observational studies. J Am Coll Cardiol. 2013;62:1421-1431.
28. Claessen BE, van der Schaaf RJ, Verouden NJ, et al. Evaluation of the effect of a concurrent chronic total occlusion on long-term mortality and left ventricular function in patients after primary percutaneous coronary intervention. JACC Cardiovasc Interv. 2009;2:1128-1134.
29. Safley DM, Koshy S, Grantham JA, et al. Changes in myocardial ischemic burden following percutaneous coronary intervention of chronic total occlusions. Catheter Cardiovasc Interv. 2011;78:337-343.
30. Nombela-Franco L, Mitroi CD, Fernandez-Lozano I, et al. Ventricular arrhythmias among implantable cardioverter-defibrillator recipients for primary prevention: impact of chronic total coronary occlusion (VACTO Primary Study). Circ Arrhythm Electrophysiol. 2012;5:147-154.
31. Danchin N, Angioi M, Cador R, et al. Effect of late percutaneous angioplastic recanalization of total coronary artery occlusion on left ventricular remodeling, ejection fraction, and regional wall motion. Am J Cardiol. 1996;78:729-735.
32. Sirnes PA, Myreng Y, Molstad P, Bonarjee V, Golf S. Improvement in left ventricular ejection fraction and wall motion after successful recanalization of chronic coronary occlusions. Eur Heart J. 1998;19:273-281.
33. Chung CM, Nakamura S, Tanaka K, et al. Effect of recanalization of chronic total occlusions on global and regional left ventricular function in patients with or without previous myocardial infarction. Catheter Cardiovasc Interv. 2003;60:368-374.
34. Hoebers LP, Claessen BE, Elias J, Dangas GD, Mehran R, Henriques JPS. Meta-analysis on the impact of percutaneous coronary intervention of chronic total occlusions on left ventricular function and clinical outcome. Internat J Cardiol. 2015;187:90-96.
35. Mashayekhi K, Neuser H, Kraus A, et al. Successful percutaneous coronary intervention improves cardiopulmonary exercise capacity in patients with chronic total occlusions. J Am Coll Cardiol. 2017;69:1095-1096.
36. Werner G. A randomized multicentre trial to evaluate the utilization of revascularization or optimal medical therapy for the treatment of chronic total coronary occlusions (EuroCTO). EuroIntervention. Abstract presented at EuroPCR Congress 2017.
37. Maeremans J, Dens J, Spratt JC, et al. Antegrade dissection and reentry as part of the hybrid chronic total occlusion revascularization strategy: a subanalysis of the RECHARGE registry (registry of CrossBoss and hybrid procedures in France, the Netherlands, Belgium and United Kingdom). Circ Cardiovasc Interv. 2017;10(6).
38. Muramatsu T, Tsuchikane E, Oikawa Y, et al. Incidence and impact on midterm outcome of controlled subintimal tracking in patients with successful recanalisation of chronic total occlusions: J-PROCTOR registry. EuroIntervention. 2014;10:681-688.
39. Michael TT, Mogabgab O, Alomar M, et al. Long-term outcomes of successful chronic total occlusion percutaneous coronary interventions using the antegrade and retrograde approach. J Interv Cardiol. 2014;27:465-471.
40. Hasegawa K, Tsuchikane E, Okamura A, et al. Incidence and impact on midterm outcome of intimal versus subintimal tracking with both antegrade and retrograde approach in patients with successful recanalization of chronic total occlusions: J-PROCTOR2 study. EuroIntervention. 2017;12:e1868-e1873.
41. Prasad A, Rihal CS, Lennon RJ, Wiste HJ, Singh M, Holmes DR Jr. Trends in outcomes after percutaneous coronary intervention for chronic total occlusions: a 25-year experience from the Mayo Clinic. J Am Coll Cardiol. 2007;49:1611-1618.
From the 1Faculty of Medicine and Life Sciences, Universiteit Hasselt, Hasselt, Belgium; 2Department of Cardiology, Ziekenhuis Oost-Limburg, Genk, Belgium; 3Department of Cardiology, Clinique de Marignane, Marignane (Marseille), France; 4Department of Cardiology, Belfast City Hospital, Belfast, United Kingdom; 5Department of Cardiology, VU University Medical Center, Amsterdam, Netherlands; 6Department of Cardiology – Groupe Hospitalier Mutualiste, Grenoble, France; 7Department of Cardiology, Universitair Medisch Centrum Utrecht, Utrecht, The Netherlands; 8Department of Cardiology, St. Antonius Hospital, Nieuwegein, Netherlands; 9Department of Cardiology, Nouvelles Cliniques Nantaises, Nantes, France; 10Department of Cardiology, Universitair Ziekenhuis Brussel, Brussels, Belgium; 11Department of Cardiology, Universitair Ziekenhuis, Gent, Belgium; 12Department of Cardiology, Morriston Hospital, Swansea, United Kingdom; 13Department of Cardiology, Golden Jubilee National Hospital, Glasgow, United Kingdom; 14Department of Cardiology – Nottingham University Hospital, Nottingham, United Kingdom; 15Department of Cardiology, Ninewells Hospital, Dundee, United Kingdom; 16Department of Cardiology, Forth Valley Royal Hospital, Edinburgh, United Kingdom; and 17Department of Cardiology, St. George’s University Hospitals NHS Foundation Trust, London, United Kingdom.
Funding. This research project is supported by a research grant from Boston Scientific. Joren Maeremans is a researcher for the Limburg Clinical Research Program (LCRP) UHasselt-ZOL-Jessa, supported by the foundation Limburg Sterk Merk (LSM), Hasselt University, Ziekenhuis Oost-Limburg and Jessa Hospital.
Disclosure. The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Dens reports grants from TopMedical (distributor of Asahi Intecc company materials), Boston Scientific, Vascular Solutions, and Orbus Neich for teaching courses and proctoring; advisory board for Boston Scientific. Drs Walsh, Hanratty, and Spratt are consultants for Abbott Vascular, Boston Scientific, Medtronic and Vascular Solutions. Dr Walsh reports research funding from Abbott Vascular, Boston Scientific, and Nitiloop. Drs Knaapen and Bressollette report honoraria from Boston Scientific for proctoring. Dr Avran reports grants form Abbott Vascular, Boston Scientific, and Biosensor for teaching courses and proctoring. Dr Irving is a proctor for Boston Scientific and Vascular Perspectives. Dr Faurie is a proctor for Boston Scientific; consultant for Cordis. Dr Kelly is a member of the advisory board of Boston Scientific and Abbott Vascular. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted August 17, 2017, provisional acceptance given August 24, 2017, final version accepted September 1, 2017.
Address for correspondence: Jo Dens, MD, PhD, Department of Cardiology, Ziekenhuis Oost-Limburg, Schiepse Bos 6, 3600 Genk, Belgium. Email: jo.dens@zol.be









