

Operator Pelvic Radiation Exposure During Percutaneous Coronary Procedures
Abstract: Objectives. To evaluate operator pelvic radiation exposure during percutaneous coronary procedures. Background. During percutaneous coronary procedures, the operator’s pelvic region is close to the x-ray source and is probably exposed to more radiation than the operator’s thorax. However, no data are available on the pelvic radiation exposure of interventional cardiologists. Methods. The RADIANT study (NCT01974453) is a prospective, single-center, observational study evaluating operator radiation exposure during percutaneous coronary procedures using electronic dosimeters placed at thorax level. In the last period of the study enrollment, a single operator was also equipped with an adjunctive electronic dedicated dosimeter to evaluate pelvic radiation exposure. Results. From a total of 2028 procedures included in the RADIANT study, operator pelvic doses were available for 138 procedures (68 right radial, 55 left radial, and 15 transfemoral). Median fluoroscopy time was 226 sec (interquartile range [IQR], 117-407 sec) and the dose-area product (DAP) was 15.3 Gy•cm2 (IQR, 9.3-27.8 Gy•cm2). Radiation dose at pelvic region was significantly higher (40.1 µSv; IQR, 22.7-76.3 µSv) compared to thorax dose (5.6 µSv; IQR, 1.5-12 µSv; P<.001) even after normalization by DAP (2.98 µSv/Gy•cm2 [IQR, 1.6-4.6 µSv/Gy•cm2] at pelvic vs 0.33 µSv/Gy•cm2 [IQR, 0.11-0.81 µSv/Gy•cm2] at thorax level; P<.001). No significant differences were observed comparing pelvic dose in right radial (42 µSv), left radial (39 µSv), or femoral access (40 µSv; P=.43). Conclusions. Operator radiation exposure to the pelvic region during percutaneous coronary procedures is significantly higher compared to thorax radiation dose independently of the vascular access site employed.
J INVASIVE CARDIOL 2018;30(2):71-74. Epub 2017 December 15.
Key words: radiation dose, transradial, pelvic, coronary procedures, PCI
Interventional cardiologists are chronically exposed to x-rays during their work, with possible associated deterministic1 and stochastic2 risks. Although the evidence supporting an increase in radiation-induced cancer among interventional cardiologists remains inconclusive, molecular studies showed that interventional cardiologists have a 2-fold increase of chromosomal damage in circulating lymphocytes compared to clinical cardiologists,3 increasing concerns about x-ray exposure. Moreover, other non-cancer effects of radiation have been detected in cardiac catheterization laboratory staff.4,5 Recently, a large survey showed that concern about radiation exposure is an important reason for young physicians (particularly women) to decide against specializing in interventional cardiology.6
Many factors have been associated with a possible higher radiation exposure during percutaneous coronary procedures.7-9 Recently, a large, randomized trial showed a significant higher radiation exposure at thorax level associated with transradial compared to transfemoral access.10 Globally, in this study, the increase in radiation exposure was low, but the difference was not negligible for some operators.
Another important determinant of radiation exposure is the distance from the radiation source; in general, the closer the distance, the higher the dose.11 For interventional cardiology operators, the pelvic region is very close to the radiation source and to the patient, with a higher radiation exposure, which we documented in a previous phantom study.12 This region could be of particular importance for young cardiologists – especially women – due to gonad exposure. However, there are no data available on operator pelvic radiation exposure during percutaneous coronary procedures, in particular during transradial approach. Therefore, the aim of this prospective study was to evaluate the operator pelvic radiation exposure, compared to the thorax dose, during percutaneous coronary procedures performed through transradial or transfemoral access.
Methods
Study design and population. The RADIANT (RAdiation Dose In percutANeous Coronary Procedures Through Transradial Approach) study (NCT01974453) is a single-center prospective, observational study designed to evaluate radiation dose absorbed by operators during percutaneous coronary procedures using different vascular access sites.9 Operator radiation exposure was measured using wearable personal electronic dosimeters placed at the left wrist (RADOS-RAD60; Laurus Systems, Inc), and at the thorax level outside the pocket of the lead apron and in the middle front (PM1610; Polimaster). During the last part of the study, another PM1610 dosimeter became available and was used by a single operator to record the radiation dose at pelvic level (outside the lead apron) in all consecutive procedures performed. The cardiologist involved was a high-volume transradial operator (>250 transradial procedures/year) who is 185 cm tall. In all procedures, standard operator radioprotection was ensured using a lead apron, a thyroid lead collar, a lower-body x-ray curtain fixed on the angiographic table, a suspended protective lead shield, and leaded glasses. In some cases, adjunctive protective drapes placed on the patient were used.
All procedures were performed using a dedicated coronary angiography system (IGS 520; GE Healthcare). The radiation doses were recorded at the beginning and end of each procedure. For patients who underwent percutaneous coronary intervention (PCI) after the diagnostic procedure, the fluoroscopy time, dose-area product (DAP), and dose of the wearable dosimeter measurements were reset at the end of the diagnostic procedure and restarted at the beginning of the PCI.
To take into account possible differences in patient radiation dose affecting the operator exposure, the DAP-normalized operator dose was also calculated.
The study enrolled all patients >18 years old who underwent diagnostic or interventional percutaneous coronary procedures. Only patients with hemodynamic instability were excluded.
All patients signed informed consent to perform the procedure and the Institutional Ethics Committee approved the protocol.
Radiation measurement. Radiation measurements recorded were fluoroscopy time and DAP. The DAP is the product of the absorbed dose to air (air Kerma) and the cross-sectional area of the x-ray field for all segments of an interventional radiology procedure, and is expressed in Gy•cm2. Operator radiation exposure was directly detected on the dosimeter screen and is expressed in µSv.
Study endpoint. The primary endpoint of the study was the operator radiation dose absorbed at pelvic level compared to the thorax dose.
Statistical analysis. Continuous variables are reported as mean and standard deviation for variables normally distributed and as median with interquartile range (IQR) for those not normally distributed, and were compared using t-test if normally distributed or Kruskal-Wallis and Mann-Whitney U-test if not. Categorical variables are indicated as the absolute number and percentage and were compared by Pearson’s Chi-square test or with the Fisher’s exact test if the number of expected patients was <5. The clinical patient characteristics were analyzed at patient level, whereas procedural characteristics and dosimetric data were analyzed at procedural level. All analyses were performed with SPSS 21.0 software (SPSS).
Results
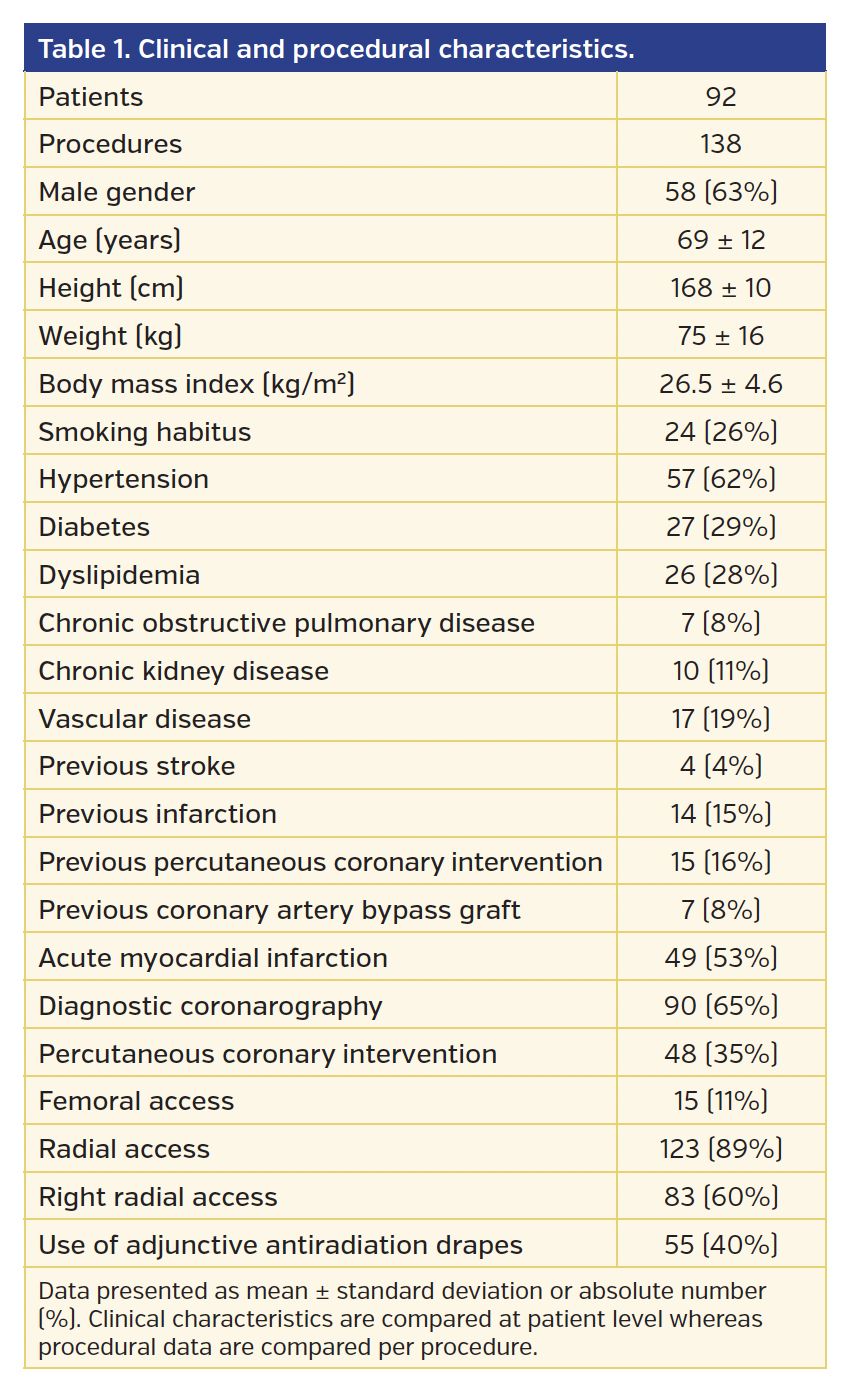
From a total of 2028 procedures performed in 1508 patients included in main RADIANT study, operator pelvic radiation exposure was available in 138 procedures performed in 92 patients. Clinical characteristics of the patients and procedural data are presented in Table 1. Most of the procedures were performed in male patients (63%) with a mean age of 69 ± 12 years and a body mass index of 26.5 ± 5 kg/m2. Radial access was performed in 123 procedures (68 right radial access and 55 left radial access) and femoral access was used in 15 procedures. The high percentage of left radial access reflects the standard of the enrolling center. Adjunctive protective antiradiation drapes placed on the patient’s pelvic region were used in 55 procedures. Median fluoroscopy time was 226 sec (IQR, 117-407 sec) and median DAP was 15.3 Gy•cm2 (IQR, 9.3-27.8 Gy•cm2).
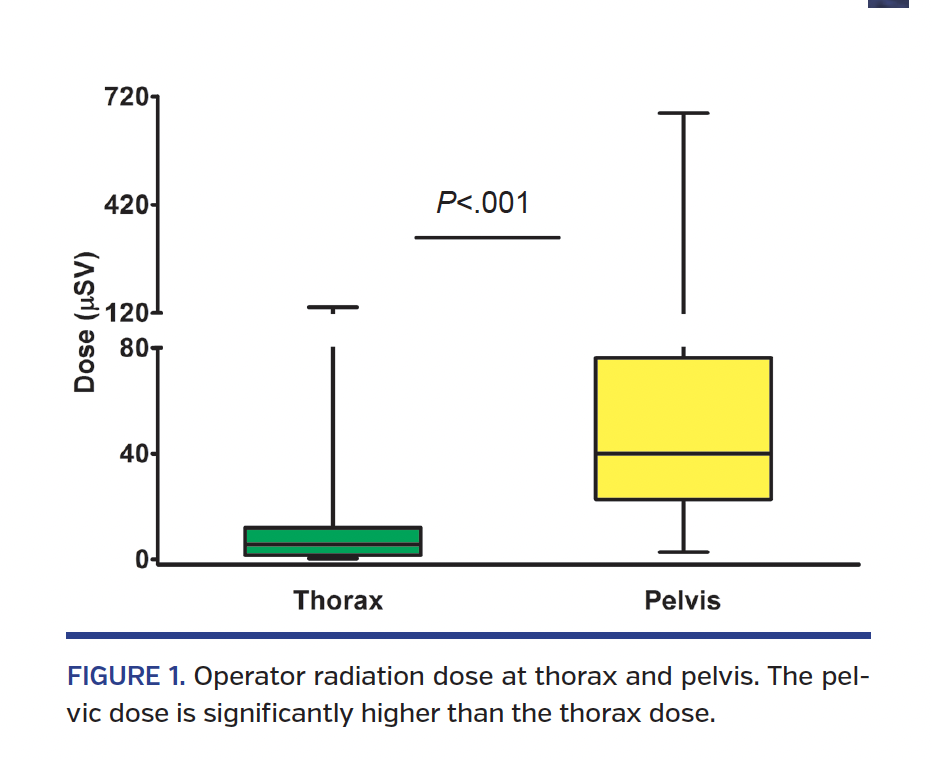
Operator radiation dose. In the entire population, radiation dose at pelvic region was significantly higher (40.1 µSv [IQR, 22.7-76.3 µSv]) compared to thorax dose (5.6 µSv [IQR, 1.5-12 µSv]; P<.001) (Figure 1). The difference still persisted after normalization by DAP, with a 9-fold higher dose in the pelvic region (2.98 µSv/Gy•cm2 [IQR, 1.6-4.6 µSv/Gy•cm2]) compared to thorax region (0.33 µSv/Gy•cm2 [IQR, 0.11-0.81 µSv/Gy•cm2]; P<.001). There were no significant differences comparing operator pelvic radiation dose in radial (40 µSv [IQR, 23.5-85.7 µSv]) or femoral access (40 µSv [IQR, 13-70 µSv]; P=.56) even when radial procedures were analyzed separately for right radial (42.1 µSv [IQR, 31.7-82.5 µSv]) or left radial access (39 µSv [IQR, 18.6-90.1 µSv]; P=.43).
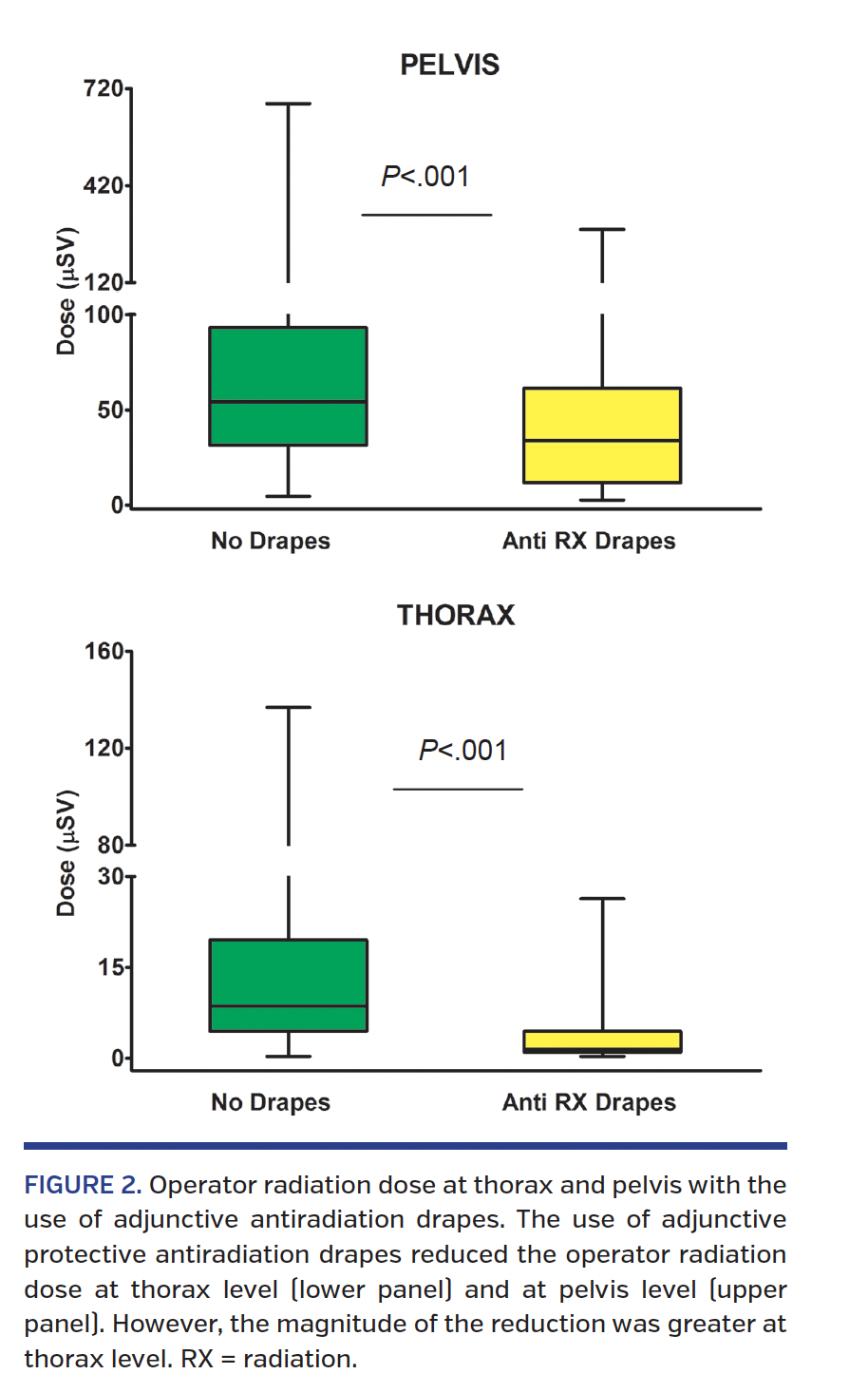
Use of adjunctive protective devices. The use of adjunctive protective antiradiation drapes placed on the patient’s pelvic region was associated with a significant reduction in operator radiation exposure at thorax level (8.6 µSv [IQR, 4.5-19.5 µSv] without drapes vs 1.6 µSv [IQR, 1.1-4.4 µSv] with drapes; P<.001) as well as at pelvic level (54.5 µSv [IQR, 31.4-93.2 µSv] without drapes vs 33.9 µSv [IQR, 11.7-61.4 µSv] with drapes; P<.001) (Figure 2). However, the percent reduction in radiation exposure using the adjunctive protective drapes was less at pelvic level than at thorax level (38% vs 80%, respectively).
Discussion
The present study is the first to investigate operator pelvic radiation exposure during percutaneous coronary procedures. We observed a significant, 9-fold higher operator radiation dose at pelvic level compared to thorax level. Moreover, the use of adjunctive devices to reduce radiation exposure was less effective at pelvic level compared to thorax level.
Radiation safety should be a key element in the cardiac catheterization laboratory considering the possible radiation-related risks to both the patient and the operator.1,2,13 In particular, the observation of a significantly higher incidence of left-side brain tumors in interventional cardiologists increased some concerns among physicians.2 Recently, these concerns have been confirmed in a large European survey showing that radiation exposure is a main factor that prevents physicians (particularly women) from pursuing a career in interventional cardiology. At the same time, the American College of Cardiology Committee Survey on Women in Cardiology showed that almost 24% of women choose a career with minimal radiation exposure.14 A further unique concern related to radiation exposure in young women is radiation exposure to gonads due to a possible pregnancy. To date, operator radiation exposure has been evaluated at thorax, eye, or left-arm level, whereas there are no data on operator pelvic dose that are correlated with pelvic exposure.
In the present study, we observed that the radiation dose to pelvic region was significantly higher compared to thorax; the possible explanation is the closer position of the pelvis to the radiation source and to the patient. Indeed, there is an inverse correlation between distance to the radiation source and radiation exposure.11 Another important point is that for the first time, we observed the magnitude of this higher pelvic exposure (9-fold compared to thorax level).
In recent years, different studies showed a possible vascular access effect to determine the operator radiation dose. In particular, radial access is associated with a higher radiation exposure when compared to femoral access,10 and right radial access exposes the operator to a higher thorax dose than left radial access.15 In this study, the operator pelvic exposure did not show significant differences among the three vascular access sites (femoral, right radial, or left radial) and in all cases, the radiation dose was significantly higher compared to thorax level.
Different measures to reduce operator radiation exposure have been utilized such as reduction in x-ray pulse rate,8 the use of fluoro rather than cine mode acquisition,16 and the use of adjunctive protective drapes.17 In the present study, the use of antiradiation drapes placed on the patient abdomen reduced the radiation dose at thorax level as well as pelvic level. However, the reduction of the radiation dose at pelvic level, even if significant, was small compared to the reduction obtained at thorax level, indicating that these devices are less effective at controlling operator pelvic exposure.
An important way to reduce operator radiation exposure is the correct use of structural shields, such as the upper mobile leaded glass and the below-table leaded curtain. In particular, the upper body shield should be located relatively far from the scatter source and close to the physician. Moreover, the upper shield should be brought down and approximate the table-attached shielding to maximize operator protection.18
Study limitations. The present study is observational rather than a randomized trial, and it is possible that there were some confounders that biased our results. This is also a single-center experience; consequently, a different arrangement of the cath lab or a different use of protective shields could give different results. Another limitation is that only one operator was equipped with the pelvic dosimeter, and we do not know if our results could be extended to operators of different heights, as operator height is an important determinant of radiation exposure;19 for instance, shorter operators have great exposure to radiation, but could have a significantly lower pelvic exposure due to better protection obtained by the below-table leaded shield. Finally, we did not use dosimeters placed under the operator lead apron, which would have evaluated the actual radiation dose absorbed by the operators.
Conclusion
Operator radiation exposure to the pelvic region during percutaneous coronary procedures is significantly higher compared to thorax radiation dose; this increase is independent of the vascular access site employed. The use of adjunctive protective drapes placed on the patient reduce only partially the operator pelvic dose, and different radioprotective devices should be considered to reduce operator pelvic radiation exposure.
References
1. Ciraj-Bjelac O, Rehani M, Minamoto A, Sim KH, Liew HB, Vaño E. Radiation-induced eye lens changes and risk for cataract in interventional cardiology. Cardiology. 2012;123:168-171.
2. Roguin A, Goldstein J, Bar O, Goldstein JA. Brain and neck tumors among physicians performing interventional procedures. Am J Cardiol. 2013;111:1368-1372.
3. Andreassi MG, Cioppa A, Botto N, et al. Somatic DNA damage in interventional cardiologists: a case control study. FASEB J. 2005;19:998-999.
4. Tonacci A, Baldus G, Corda D, et al. Olfactory non-cancer effects of exposure to ionizing radiation in staff working in the cardiac catheterization laboratory. Int J Cardiol. 2014;171:461-463.
5. Andreassi MG, Piccaluga E, Gargani L, et al. Subclinical carotid atherosclerosis and early vascular aging from long-term low-dose ionizing radiation exposure: a genetic, telomere, and vascular ultrasound study in cardiac catheterization laboratory staff. JACC Cardiovasc Interv. 2015;8:616-627.
6. Capranzano P, Kunadian V, Mauri J, et al. Motivations for and barriers to choosing an interventional cardiology career path: results from the EAPCI Women Committee worldwide survey. EuroIntervention. 2016;12:53-59.
7. Agarwal S, Parashar A, Bajaj NS, et al. Relationship of beam angulation and radiation exposure in the cardiac catheterization laboratory. JACC Cardiovasc Interv. 2014;7:558-566.
8. Abdelaal E, Plourde G, Mac Haalany J, et al. Effectiveness of low rate fluoroscopy at reducing operator and patient radiation dose during transradial coronary angiography and interventions. JACC Cardiovasc Interv. 2014;7:567-574.
9. Sciahbasi A, Rigattieri S, Sarandrea A, et al. Determinants of operator radiation exposure during percutaneous coronary procedures. Am Heart J. 2017;187:10-18.
10. Sciahbasi A, Frigoli E, Sarandrea A, et al. Radiation exposure and vascular access in acute coronary syndromes: the RAD-Matrix trial. J Am Coll Cardiol. 2017;69:2530-2537.
11. Hirshfeld JW Jr, Balter S, Brinker JA, et al. ACCF/AHA/HRS/SCAI clinical competence statement on physician knowledge to optimize patient safety and image quality in fluoroscopically guided invasive cardiovascular procedures: a report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence and Training. Circulation. 2005;111:511-532.
12. Sciahbasi A, Rigattieri S, Sarandrea A, et al. Operator radiation exposure during right or left transradial coronary angiography: a phantom study. Cardiovasc Revasc Med. 2015;16:386-390.
13. Vañó E, Arranz L, Sastre JM, et al. Dosimetric and radiation protection considerations based on some cases of patient skin injuries in interventional cardiology. Br J Radiol. 1998;71:510-516.
14. Poppas A, Cummings J, Dorbala S, Douglas PS, Foster E, Limacher MC. Survey results: a decade of change in professional life in cardiology: a 2008 report of the ACC women in cardiology council. J Am Coll Cardiol. 2008;52:2215-2226.
15. Sciahbasi A, Romagnoli E, Trani C, et al. Operator radiation exposure during percutaneous coronary procedures through the left or right radial approach: the TALENT dosimetric substudy. Circ Cardiovasc Interv. 2011;4:226-231.
16. Olcay A, Guler E, Karaca IO, et al. Comparison of fluoro and cine coronary angiography: balancing acceptable outcomes with a reduction in radiation dose. J Invasive Cardiol. 2015;27:199-202.
17. Sciahbasi A, Rigattieri S, Sarandrea A, et al. Radiation dose absorbed by operators during transradial percutaneous coronary procedures comparing different protective drapes: the RADIATION study. EuroIntervention. 2017;12:e2253-e2261.
18. Fetterly KA, Magnuson DJ, Tannahill GM, Hindal MD, Mathew V. Effective use of radiation shields to minimize operator dose during invasive cardiology procedures. JACC Cardiovasc Interv. 2011;4:1133-1139.
19. Rigatelli G, Panin S, Fiorrevanti R, et al. Impact of operators’ height on individual radiation exposure measurements during catheter-based cardiovascular interventions. J Interv Cardiol. 2016;29:83-88.
From the 1Department of Interventional Cardiology, Sandro Pertini Hospital, Rome, Italy; 2Niguarda Hospital, Milan, Italy; 3HSE Management, Rome, Italy; 4Department of Cardiology, University of L’Aquila, Italy; and 5ASL RM2, Rome, Italy.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Sciabasi reports advisory board fees from Bayer Healthcare. Dr Rigattieri reports advisory board fees from Astra Zeneca. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted August 11, 2017, provisional acceptance given September 1, 2017, final version accepted October 13, 2017.
Address for correspondence: Alessandro Sciahbasi, Interventional Cardiology, Sandro Pertini Hospital, ASL Roma2, Rome, Italy. Email: alessandro.sciahbasi@fastwebnet.it










