

Orbital Atherectomy in Women 2.0 – Another Brick in the Wall
The impact of gender on percutaneous coronary intervention (PCI) outcomes has been the topic of intense research since the very beginning of percutaneous techniques and many hypotheses and explanations have been proposed. Our understanding of the impact of gender differences in PCI has significantly advanced in the last decade. Various components of gender-specific PCI outcomes have been the focus of multiple investigations. In this issue of the Journal of Invasive Cardiology, Lee et al1 focus on device-specific outcomes and report similar angiographic and clinical outcomes between females and males undergoing orbital atherectomy (OA) for plaque modification.
Devices addressing coronary calcification are greatly needed given the increasing complexity of patients presenting to cardiac catheterization laboratories worldwide. Three decades after the appearance of rotational atherectomy (RA), OA has emerged as a new technique specifically designed to address calcified coronary artery lesions. Safety and feasibility of the OA system for de novo calcified lesions were shown in the pivotal ORBIT I and II trials.2,3 When gender-specific outcomes were analyzed in a subsequent publication, procedural success was similar between women and men (89.7% vs 88.4%, respectively; P=.75); however, there were fewer perforations in men vs women (1.3% vs 2.1%, respectively; P=.72) and significantly more severe dissections in women (6.4% vs 1.7%; P=.01).4
The work by Lee et al confirms previous observations addressing gender-specific OA outcomes from the ORBIT II trial.1 Using data from 458 consecutive real-world patients from three centers (31% women) they report a primary endpoint of major adverse cardiac and cerebrovascular events of 0.7% for women and 2.9% for men (P=.14). Individual endpoints of death (0.7% vs 1.6%; P=.43), myocardial infarction (0.7% vs 1.3%; P=.58), target-vessel revascularization (0% vs 0%; P>.99), and stroke (0.0% vs 0.3%; P=.50) were low and did not differ in both groups. Periprocedural complications were also low, with perforation rate of 0.8% vs 0.7% (P>.90), dissection rate of 0.8% vs 1.1% (P=.80), and no-reflow rate of 0.8% vs 0.7% (P>.90). Although this was not a randomized trial, sex-based outcomes were in accordance with those reported in the ORBIT II study. Interestingly, female dissection rates in the present study were similar between the two sexes, differentiating it from a previous study (443 patients; 35% women) that reported a much higher adjusted risk of severe dissections in women.4
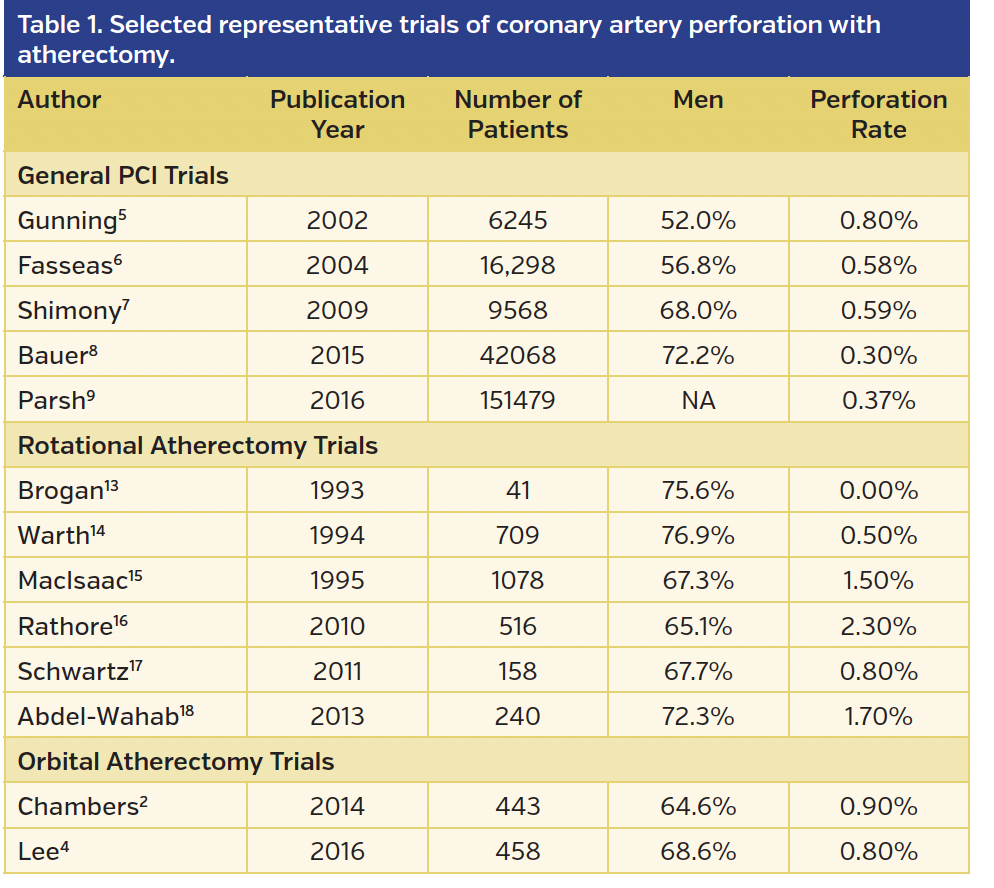
Probably one of the most dreaded complications for every interventional cardiologist is coronary perforation during PCI. Reported rates in large series range between 0.4%-0.6%.5-9 Perforations have been reported over the years in several trials involving both RA and OA, with atherectomy-associated rates generally higher than in all-comer registries (Table 1). Perforations are frequently associated with serious adverse outcomes and based on recent data appear to be more lethal in women. In a contemporary analysis of 151,459 all-comer PCIs, perforations were observed in 0.37% of patients. While in multivariate analysis women were not at a higher risk for perforations, mortality in women with coronary perforation was more than twice as high as in men (4.9% vs 2.4%).9
It is important to view the current literature on OA in view of the aforementioned statistics and complication rates. This is why the paper by Lee et al is important in furthering our understanding of this new device available to us in the cardiac catheterization laboratory. Small series are hypothesis generating and allow us to attempt to answer important safety questions on a larger scale. The Food and Drug Administration post-marketing device surveillance is truly a unique, essential process that allows us to collect data nationwide in daily clinical practice.10 Similarly, the National Cardiovascular Data Registry is an exceedingly important tool for us to understand how new devices and procedures perform when widely used in diverse populations.11,12 It is unlikely that a large randomized trial addressing the issue of gender and treatment of calcified lesions will ever be performed – we continue to learn in an iterative process to take better care of our increasingly more complex patients. The study by Lee et al is another brick in the wall of our knowledge.
References
1. Lee M, Shlofmitz E, Mansourian P, Sethi S, Shlofmitz R. Gender-based differences in outcomes after orbital atherectomy for the treatment of de novo severely calcified coronary lesions. J Invasive Cardiol. 2016;28:440-443.
2. Parikh K, Chandra P, Choksi N, Khanna P, Chambers J. Safety and feasibility of orbital atherectomy for the treatment of calcified coronary lesions: the ORBIT I trial. Catheter Cardiovasc Interv. 2013;81:1134-1139.
3. Chambers JW, Feldman RL, Himmelstein SI, et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv. 2014;7:510-518.
4. Kim CY, Lee AC, Wiedenbeck TL, Lee MS, Chambers JW. Gender differences in acute and 30-day outcomes after orbital atherectomy treatment of de novo, severely calcified coronary lesions. Catheter Cardiovasc Interv. 2016;87:671-677.
5. Gunning MG, Williams IL, Jewitt DE, Shah AM, Wainwright RJ, Thomas MR. Coronary artery perforation during percutaneous intervention: incidence and outcome. Heart. 2002;88:495-498.
6. Fasseas P, Orford JL, Panetta CJ, et al. Incidence, correlates, management, and clinical outcome of coronary perforation: analysis of 16,298 procedures. Am Heart J. 2004;147:140-145.
7. Shimony A, Zahger D, Van Straten M, et al. Incidence, risk factors, management and outcomes of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2009;104:1674-1677.
8. Bauer T, Boeder N, Nef HM, et al. Fate of patients with coronary perforation complicating percutaneous coronary intervention (from the Euro Heart Survey Percutaneous Coronary Intervention Registry). Am J Cardiol. 2015;116:1363-1367.
9. Parsh J, Seth M, Green J, et al. The deadly impact of coronary perforation in women undergoing PCI: insights from BMC2. J Am Coll Cardiol. 2016;67:179.
10. Resnic FS, Normand S-LT. Postmarketing surveillance of medical devices — filling in the gaps. N Engl J Med. 2012;366:875-877.
11. Brilakis ES, Banerjee S, Karmpaliotis D, et al. Procedural outcomes of chronic total occlusion percutaneous coronary intervention: a report from the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc Interv. 2015;8:245-253.
12. Rumsfeld JS, Peterson ED. Achieving meaningful device surveillance: from reaction to proaction. JAMA. 2010;304:2065-2066.
13. Brogan WC 3rd, Popma JJ, Pichard AD, et al. Rotational coronary atherectomy after unsuccessful coronary balloon angioplasty. Am J Cardiol. 1993;71:794-798.
14. Warth DC, Leon MB, O’Neill W, et al. Rotational atherectomy multicenter registry: acute results, complications and 6-month angiographic follow-up in 709 patients. J Am Coll Cardiol. 1994;24:641-648.
15. MacIsaac AI, Bass TA, Buchbinder M, et al. High speed rotational atherectomy: outcome in calcified and noncalcified coronary artery lesions. J Am Coll Cardiol. 1995;26:731-736.
16. Rathore S, Matsuo H, Terashima M, et al. Rotational atherectomy for fibro-calcific coronary artery disease in drug eluting stent era: procedural outcomes and angiographic follow-up results. Catheter Cardiovasc Interv. 2010;75:919-927.
17. Schwartz BG, Mayeda GS, Economides C, Kloner RA, Shavelle DM, Burstein S. Rotational atherectomy in the drug-eluting stent era: a single-center experience. J Invasive Cardiol. 2011;23:133-139.
18. Abdel-Wahab M, Richardt G, Joachim Buttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6:10-19.
From the Department of Veterans Affairs, Jesse Brown VA Medical Center, Chicago, Illinois and Division of Cardiology, Department of Medicine, University of Illinois at Chicago, Chicago, Illinois.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Vidovich discloses consultant fees from CSI. Dr Voudris reports no conflicts of interest regarding the content herein.
Address for correspondence: Mladen I. Vidovich, MD, 840 S Wood Street, MC 715, Chicago, IL 60613. Email: miv@uic.edu









