

Percutaneous Closure of Paravalvular Leaks After Transcatheter Aortic Valve Implantation With Edwards SAPIEN Prosthesis: A Report of Two Cases
Download a PDF of this article.
Abstract: Significant periprosthetic aortic regurgitation after transcatheter aortic valve implantation with Edwards SAPIEN prosthesis has become a major concern of this technique given its association with impaired survival. We report the successful closure of such defects using vascular occlusion devices with significant improvement in clinical status of patients.
J INVASIVE CARDIOL 2013;25(2):92-95
Key words: transcatheter aortic valve implantation
___________________________________________________
Aortic stenosis is the symptomatic valvulopathy with a higher prevalence in Western countries.1 When this condition is associated with cardiovascular symptoms, such as angina, heart failure, or syncope of unknown etiology, valve replacement is considered the first-line treatment.2 It occurs predominantly in elderly patients in association with other comorbidities3 who, due to the higher surgical risk,4 are not good candidates for surgical valve replacement. In the last years, transcatheter aortic valve implantation (TAVI) has emerged as a safe and efficient alternative in patients not suitable for cardiac surgery. Several patient series have been recently published showing acceptable results at the short and long term with any of the two devices approved to date: Edwards SAPIEN aortic valve prosthesis (Edwards Lifesciences) and CoreValve Revalving System (Medtronic).5-8 Moreover, it has been proven that, in this group of high-risk patients, the use of the Edwards prosthesis is not inferior to conventional surgery.9
However, it has been recently demonstrated that periprosthetic aortic regurgitation (PAR) is not an uncommon finding after TAVI and this is linked to an impaired prognosis10 in a recent large registry. Likewise, it is still a matter of controversy how to deal with this frequent complication. We report two cases of patients with severe PAR after TAVI procedure successfully treated by percutaneous closure with vascular plugs.
Case Presentations
Case 1. An 85-year-old male was admitted to our institution due to shortness of breath and progressive exertional chest pain. He reported a previous smoking habit and hypertension as cardiovascular risk factors. His previous cardiovascular history comprised several episodes of paroximal atrial fibrillation and peripheral vascular disease with intermittent claudication of lower limbs. Other comormidities were mild chronic kidney disease and a bladder neoplasm treated 6 years before, without evidence of recurrence. During diagnostic work-up, a transthoracic echocardiogram showed a non-dilated moderately hypertrophic left ventricle (LV) with preserved function and a severe calcified aortic stenosis (mean gradient, 47.6 mm Hg; aortic valve area [AVA], 0.78 cm2). Aortic annulus measurement was 24 mm. The angiographic study demonstrated a significant proximal right coronary artery (RCA) stenosis and severe concentric calcification and tortuosity of both aorto-iliac systems. After a joint heart team meeting, the patient was rejected for conventional aortic valve replacement due to high comorbidities (Logistic EuroScore, 17.7%; STS score, 7.5%) and frailty, and he was scheduled for TAVI via transapical route, because of his severe vascular disease. Prior to implantation, a bare-metal stent was placed in the proximal RCA. The patient underwent 26 mm Edwards SAPIEN TAVI (after confirmation of aortic annulus diameter by transesophageal echo) without complications (final aortic stent diameter, 26.25 mm) and discharge echo showed a preserved prosthetic valve function with a mild periprosthetic regurgitation jet located in the posterior part of the annulus.
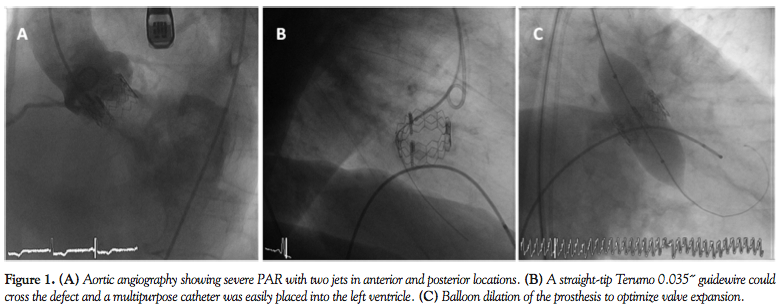 A month after discharge, the patient started complaining again of progressive shortness of breath; 5 weeks after the procedure, he was re-admitted to our hospital due to signs and symptoms of heart failure. A new echo showed preserved LV ejection fraction and normal function of the aortic valve with the same degree of periprosthetic regurgitation. However, the angiographic study was repeated and an aortogram showed a severe PAR with two jets, one in a posterior location and the other in an anterior position (Figure 1A). A straight-tip Terumo 0.035˝ guidewire could cross the defect and a multipurpose catheter was easily placed into the LV (Figure 1B). Several dilations of the prosthesis with an oversized balloon (25 mm Cristal balloon; Balt extrusion, inflated mechanically up to 6 atm) were carried out to optimize the expansion of the valve stent (Figure 1C), but the degree of angiographic insufficiency did not diminish.
A month after discharge, the patient started complaining again of progressive shortness of breath; 5 weeks after the procedure, he was re-admitted to our hospital due to signs and symptoms of heart failure. A new echo showed preserved LV ejection fraction and normal function of the aortic valve with the same degree of periprosthetic regurgitation. However, the angiographic study was repeated and an aortogram showed a severe PAR with two jets, one in a posterior location and the other in an anterior position (Figure 1A). A straight-tip Terumo 0.035˝ guidewire could cross the defect and a multipurpose catheter was easily placed into the LV (Figure 1B). Several dilations of the prosthesis with an oversized balloon (25 mm Cristal balloon; Balt extrusion, inflated mechanically up to 6 atm) were carried out to optimize the expansion of the valve stent (Figure 1C), but the degree of angiographic insufficiency did not diminish.
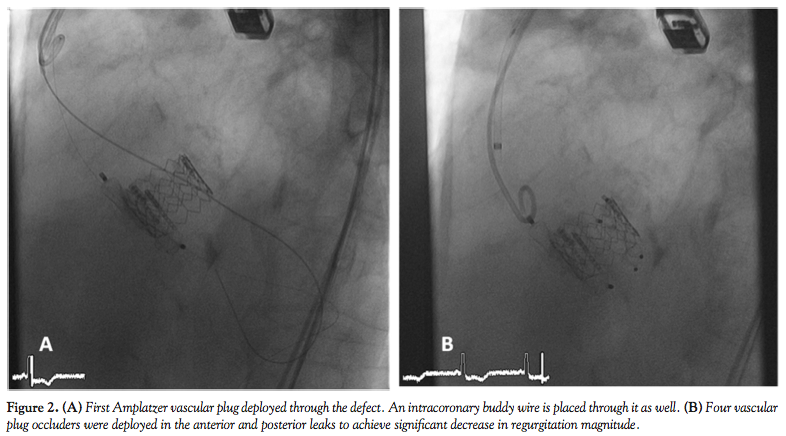 In this situation, we therefore scheduled the patient to make an attempt to close the paravalvular leak by percutaneous route using vascular plug occluders, under general anesthesia and with transesophageal echo (TEE) guidance. Using an 8 Fr right femoral approach, a straight-tip Terumo 0.035˝ guidewire was placed first through the anterior leak and a 5 Fr Terumo Vertebral Glidecath (Terumo Europe) was passed to the LV. The Terumo wire was retrieved and exchanged by an Amplatz Extra Stiff guidewire (Cook Medical). Through this guidewire, an AGA Amplatzer TorqVue 45° 8 Fr sheath (AGA Medical Corporation) was placed in the LV through the defect. Subsequently, the Amplatz wire was retrieved and a 14 x 5 mm Vascular Plug III (AGA Medical Corporation) was deployed (Figure 2A). Due to residual shunt, another Vascular Plug III (10 x 5 mm) was placed in the same defect after
In this situation, we therefore scheduled the patient to make an attempt to close the paravalvular leak by percutaneous route using vascular plug occluders, under general anesthesia and with transesophageal echo (TEE) guidance. Using an 8 Fr right femoral approach, a straight-tip Terumo 0.035˝ guidewire was placed first through the anterior leak and a 5 Fr Terumo Vertebral Glidecath (Terumo Europe) was passed to the LV. The Terumo wire was retrieved and exchanged by an Amplatz Extra Stiff guidewire (Cook Medical). Through this guidewire, an AGA Amplatzer TorqVue 45° 8 Fr sheath (AGA Medical Corporation) was placed in the LV through the defect. Subsequently, the Amplatz wire was retrieved and a 14 x 5 mm Vascular Plug III (AGA Medical Corporation) was deployed (Figure 2A). Due to residual shunt, another Vascular Plug III (10 x 5 mm) was placed in the same defect after  re-crossing the defect, with a significant decrease in insufficiency magnitude. The delivery cable of the first device was not released until the second device was placed through the defect to avoid the possibility of dislodgment. During the positioning and deployment of the occluders, a 0.014˝ intracoronary buddy-wire was kept in the defect to maintain the position if further intervention was requested. The same maneuvers were carried out with the posterior leak, and again two Vascular Plug III occluders of the same dimension were placed through the defect (Figure 2B). A control angiogram showed that, after treatment, the global degree of angiographic regurgitation was now mild and with a significant decrease from the initial angio (Figure 3A). An excellent result was also ascertained from the TEE monitoring (Figure 3B).
re-crossing the defect, with a significant decrease in insufficiency magnitude. The delivery cable of the first device was not released until the second device was placed through the defect to avoid the possibility of dislodgment. During the positioning and deployment of the occluders, a 0.014˝ intracoronary buddy-wire was kept in the defect to maintain the position if further intervention was requested. The same maneuvers were carried out with the posterior leak, and again two Vascular Plug III occluders of the same dimension were placed through the defect (Figure 2B). A control angiogram showed that, after treatment, the global degree of angiographic regurgitation was now mild and with a significant decrease from the initial angio (Figure 3A). An excellent result was also ascertained from the TEE monitoring (Figure 3B).
Three days after the procedure, the patient was discharged with no further complications and he is doing well at 1-year follow-up.
Case 2. An 84-year-old male was sent to our institution to evaluate the possibility of TAVI due to severe calcified aortic stenosis and New York Heart Association class III heart failure. Relevant background showed dyslipidemia as a cardiovascular risk factor and coronary artery bypass graft surgery in 2000 due to left main and three-vessel disease. Echo study revealed an LV with moderately impaired function (LV ejection fraction, 42%) due to inferior and apical akinesia, moderate concentric hypertrophy, and severe aortic stenosis (mean gradient, 63.2 mm Hg; AVA, 0.50 cm2). Angiographic assessment pre-TAVI showed severe diffuse 3-vessel coronary disease, patent grafts, and mild calcification without significant disease of aorto-iliac arteries. The Logistic EuroScore was 19.9% and STS score was 8.9%.
Hence, the TAVI procedure was accomplished via femoral route and a 23 mm Edwards SAPIEN valve was successfully implanted (final aortic stent diameter, 22.98 mm). In the control angiography after device deployment, a significant residual regurgitation in anterior periprosthetic location was observed. To overcome this drawback, several inflations with an oversized balloon were performed (Cristal balloon 25 mm; Balt extrusion, inflated mechanically up to 4 atm) and a reduction in the degree of insufficiency was achieved, considering the result as acceptable, with mild angiographic residual shunt. The patient was discharged uneventfully 3 days after the procedure.
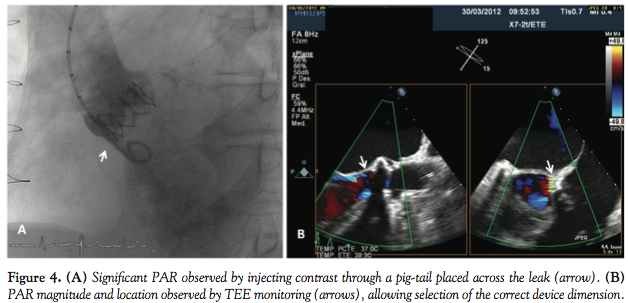 Two weeks after implantation, the patient was admitted to another hospital because of several episodes of typical chest pain at rest and symptoms of heart failure. The patient was re-transferred to our center for a new angiographic evaluation of coronary disease, grafts, and residual regurgitation. Echo study before catheterization showed a normal prosthetic function with mild anterior periprosthetic regurgitation. Angiographic evaluation confirmed no changes in coronary disease or patency of grafts and severe aortic insufficiency due to an anterior paravalvular leak (Figure 4A). TEE study confirmed the location and magnitude of the residual defect (Figure 4B).
Two weeks after implantation, the patient was admitted to another hospital because of several episodes of typical chest pain at rest and symptoms of heart failure. The patient was re-transferred to our center for a new angiographic evaluation of coronary disease, grafts, and residual regurgitation. Echo study before catheterization showed a normal prosthetic function with mild anterior periprosthetic regurgitation. Angiographic evaluation confirmed no changes in coronary disease or patency of grafts and severe aortic insufficiency due to an anterior paravalvular leak (Figure 4A). TEE study confirmed the location and magnitude of the residual defect (Figure 4B).
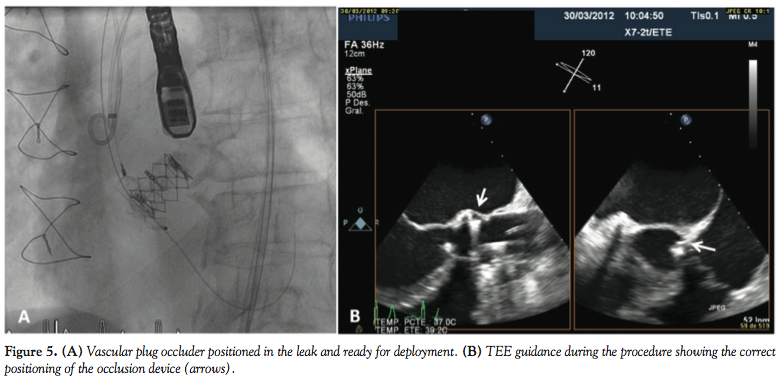 Four days after diagnosis, under general anesthesia and TEE monitoring, percutaneous closure was attempted. Using an 8 Fr sheath through the right femoral approach, we were able to advance a straight-tip 0.035˝ Terumo guidewire, probing the defect. Subsequently, a 4 Fr multipurpose catheter (Cordis) was advanced into the LV and the wire was exchanged by an Amplatz Extra-Stiff guidewire in order to advance the plug delivery system. An 8 Fr Amplatzer TorqVue sheath was placed through the defect in the LV and a 12 x 5 mm Vascular Plug III was delivered in the defect (Figure 5A) with practically total disappearance of regurgitation. TEE monitoring confirmed the correct positioning of the occluder device (Figure 5B).
Four days after diagnosis, under general anesthesia and TEE monitoring, percutaneous closure was attempted. Using an 8 Fr sheath through the right femoral approach, we were able to advance a straight-tip 0.035˝ Terumo guidewire, probing the defect. Subsequently, a 4 Fr multipurpose catheter (Cordis) was advanced into the LV and the wire was exchanged by an Amplatz Extra-Stiff guidewire in order to advance the plug delivery system. An 8 Fr Amplatzer TorqVue sheath was placed through the defect in the LV and a 12 x 5 mm Vascular Plug III was delivered in the defect (Figure 5A) with practically total disappearance of regurgitation. TEE monitoring confirmed the correct positioning of the occluder device (Figure 5B).
The patient was discharged 2 days later with no further complications and he is symptom free 2 months after closure.
Discussion
PAR has become a main concern after TAVI. It has been reported that nearly all patients undergoing this procedure have some degree of PAR, most of them mild (<2/4). However, around 14%-20% may have significant (≥2/4) AR,10,12 which has been recently linked to an increasing mortality rate.10,12,13 The association between significant PAR and worse prognosis is easily understandable given the effect of an early acute valvular insufficiency in patients with hypertrophic low-compliant ventricles.14 Factors associated with this condition, such as severe asymmetric calcification of the native aortic valve,15 incomplete expansion of the device, incorrect positioning, team experience, or inappropriate prosthesis size have been previously reported.11,16 Although conventional criteria should be used to assess the severity of the PAR, sometimes transthoracic echocardiography may have limitations, such as poor acoustic window and difficulties in the evaluation of jet magnitude, due to the morphology of such regurgitating jets (usually very eccentric). As an example, in our two cases, expert echocardiographers graded the PAR as mild (<2/4) in both patients, while angiography or TEE demonstrated the severity. Therefore, we encourage clinicians to continue with diagnostic work-up either by TEE or invasive angiography if there is any incongruence between clinical status and the results of TTE.
The management of paravalvular leaks after TAVI is still a matter of controversy. Mild degrees of paravalvular regurgitation (<2/4) might be clinically followed as they are thought to be benign and not progressive in the majority of patients.17 However, more severe degrees of AR may be clinically relevant and need intervention. Usually, balloon postdilatation is the first option for paravalvular leaks following TAVI, using a slightly oversized balloon. Nonetheless, the use of postdilatation is limited by valve leaflet damage or the possibility of aortic annulus rupture. In both our cases, balloon dilatation was the first-line intervention, but failed to solve the paravalvular regurgitation, although no complications were observed after the use of an oversized balloon. The possibility of implanting a valve-in-valve to treat this complication has also been described,18 with an excellent result. However, this strategy may be limited due to few available access routes in some patients and may not be useful, as well, if the leak is produced by the presence of bulky calcification of the annulus. And finally, the use of occlusion devices may be an appropriate technique to deal with such paravalvular leaks. There have been reports of previous successful experiences of closing leaks after surgically replaced valves,19 which may offer potential advantages. Given the low profile of sheaths to deliver the devices, its use might be extended to patients with vascular disease who are unsuitable for transfemoral TAVI, allowing treatment of several leaks in a single procedure. Notwithstanding, although not observed in our series, there are potential risks of the technique such as valve dislodgment during device delivery, entrapment of a wire in the stent struts while crossing the defect, stroke, or closure device embolization, and extreme caution should be taken to avoid them.
Conclusions
Significant PAR after TAVI is not uncommon and may result in clinical deterioration of patients. Device closure of these defects is a safe and feasible strategy to solve them. We believe that this technique should stay at the frontline of management of significant paravalvular leaks after TAVI.
References
- Lung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24(13):1231-1243.
- Vahanian A, Baumgartner H, Bax J, et al. [Guidelines on the management of valvular heart disease]. Rev Esp Cardiol. 2007;60(6):1e-50e.
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005-1011.
- Lung B, Cachier A, Baron G, et al. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur Heart J. 2005;26(24):2714-2720.
- Webb JG, Altwegg L, Boone RH, et al. Transcatheter aortic valve implantation: impact on clinical and valve-related outcomes. Circulation. 2009;119(23):3009-3016.
- Rodés-Cabau J, Webb JG, Cheung A, et al. Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgical risk: acute and late outcomes of the multicenter Canadian experience. J Am Coll Cardiol. 2010;55(11):1080-1090.
- Piazza N, Grube E, Gerckens U, et al. Procedural and 30-day outcomes following transcatheter aortic valve implantation using the third generation (18 Fr) CoreValve revalving system: results from the multicentre, expanded evaluation registry 1-year following CE mark approval. EuroIntervention. 2008;4(2):242-249.
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198.
- Gilard M, Eltchaninoff H, Iung B, et al. Registry of transcatheter aortic-valve implantation in high-risk patients. N Engl J Med. 2012;366(18):1705-1715.
- Detaint D, Lepage L, Himbert D, et al. Determinants of significant paravalvular regurgitation after transcatheter aortic valve: implantation impact of device and annulus discongruence. JACC Cardiovasc Interv. 2009;2(9):821-827.
- Tamburino C, Capodanno D, Ramondo A, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation. 2011;123(3):299-308.
- Kodali SK, Williams MR, Smith CR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366(18):1686-1695.
- Stout KK, Verrier ED. Acute valvular regurgitation. Circulation. 2009;119(25):3232-3241.
- Zegdi R, Ciobotaru V, Noghin M, et al. Is it reasonable to treat all calcified stenotic aortic valves with a valved stent? Results from a human anatomic study in adults. J Am Coll Cardiol. 2008;51(5):579-584.
- Goncalves A, Marcos-Alberca P, Zamorano JL. Echocardiography: guidance during valve implantation. EuroIntervention. 2010;6(Suppl G):G14-G19.
- Rallidis LS, Moyssakis IE, Ikonomidis I, Nihoyannopoulos P. Natural history of early aortic paraprosthetic regurgitation: a five-year follow-up. Am Heart J. 1999;138(2 Pt 1):351-357.
- Rodes-Cabau J, Dumont E, Doyle D. “Valve-in-valve” for the treatment of paravalvular leaks following transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2009;74(7):1116-1119.
- Latson LA. Transcatheter closure of paraprosthetic valve leaks after surgical mitral and aortic valve replacements. Expert Rev Cardiovasc Ther. 2009;7(5):507-514.
__________________________________________________
From the Interventional Cardiology Unit, Division of Cardiology, Complejo Hospitalario Universitario A Coruña, La Coruña, Spain.
Funding: Dr. Rodrigo Estévez-Loureiro is supported by a Rio Hortega grant from the Instituto Carlos III, Ministerio de Ciencia e Innovación.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted July 6, 2012, provisional acceptance given July 13, 2012, final version accepted August 20, 2012.
Address for correspondence: Rodrigo Estévez-Loureiro, MD, Interventional Cardiology Unit, Division of Cardiology. Complejo Hospitalario Universitario A Coruña, Xubias de Arriba 84, 15006 A Coruña, La Coruña, Spain. Email: rodrigo.estevez.loureiro@sergas.es












