

Percutaneous Coronary Intervention in Severely Calcified Unprotected Left Main Coronary Artery Disease: Initial Experience With Orbital Atherectomy
Abstract: Objective. We report the clinical outcomes of patients who underwent percutaneous coronary intervention (PCI) with orbital atherectomy for severely calcified unprotected left main coronary artery (ULMCA) disease. Background. Although surgical revascularization is the gold standard for patients with ULMCA disease, not all patients are candidates for this. PCI is increasingly used to treat complex coronary artery disease, including ULMCA disease. The presence of severely calcified lesions increases the complexity of PCI. Orbital atherectomy can be used to facilitate stent delivery and expansion in severely calcified lesions. The clinical outcomes of patients treated with orbital atherectomy for severely calcified ULMCA disease have not been reported. Methods. From May 2014 to July 2015, a total of 14 patients who underwent PCI with orbital atherectomy for ULMCA disease were retrospectively evaluated. The primary endpoint was major cardiac and cerebrovascular event (cardiac death, myocardial infarction, stroke, and target-lesion revascularization) at 30 days. Results. The mean age was 78.2 ± 5.8 years. The mean ejection fraction was 41.8 ± 19.8%. Distal bifurcation disease was present in 9 of 14 patients. Procedural success was achieved in all 14 patients. The 30-day major adverse cardiac and cerebrovascular event rate was 0%. One patient had coronary dissection that was successfully treated with stenting. No patient had perforation, slow flow, or thrombosis. Conclusions. Orbital atherectomy in patients with severely calcified ULMCA disease is feasible, even in high-risk patients who were considered poor surgical candidates. Randomized trials are needed to determine the role of orbital atherectomy in ULMCA disease.
J INVASIVE CARDIOL 2016;28(4):147-150
Key words: atherectomy, calcified lesions, ULMCA
________________________________________
Drug-eluting stents, which significantly reduce the rate of repeat revascularization, have led to expanded use of percutaneous coronary intervention (PCI) in patients with complex coronary anatomy. Although the gold standard for the treatment of unprotected left main coronary artery (ULMCA) disease is coronary artery bypass graft (CABG) surgery, PCI is a safe and effective treatment option when patients are carefully selected.1 In particular, patients who are most likely to benefit are patients with low-to-intermediate SYNTAX scores.2 The presence of heavy calcification increases the SYNTAX score. Severely calcified coronary artery lesions are associated with poor short-term and medium-term prognosis.3 Severe coronary calcification increases the complexity of PCI by decreasing vessel elasticity, and therefore, may prohibit the delivery of the stent to the lesion as well as optimal stent expansion and apposition, increasing the risk of death, myocardial infarction, stent thrombosis, and in-stent restenosis.4
Rotational atherectomy modifies severely calcified plaque, facilitating optimal stent expansion and apposition as well as improving procedural success.5 The American College of Cardiology Foundation/American Heart Association/Society for Cardiovascular Angiography and Interventions PCI guideline provides a class IIa recommendation for rotational atherectomy for fibrotic or heavily calcified lesions that might not be crossed by a balloon catheter or adequately dilated before stent implantation.1 The data on the clinical benefit of rotational atherectomy of the ULMCA are limited by small studies with short-term follow-up.6,7
Orbital atherectomy (Cardiovascular Systems, Inc) was approved by the United States Food and Drug Administration on October 21, 2013 for the treatment of severe coronary artery calcification given the excellent results at 30 days of the ORBIT II trial.8 The 1-year and 2-year data also reported excellent outcomes.9,10 However, the safety and efficacy of orbital atherectomy for the treatment of severely calcified ULMCA disease are unknown, as these trials did not include patients with ULMCA. We report the first clinical outcomes in patients with severely calcified ULMCA disease treated with orbital atherectomy.
Methods
Study population. Between May 2014 and July 2015, the data on 14 patients with severely calcified ULMCA disease who underwent PCI with orbital atherectomy were retrospectively analyzed. The patients included 14 patients who were treated from three centers (UCLA Medical Center, Los Angeles, California [2 patients], St. Francis Hospital, Roslyn, New York [4 patients], and North Shore University Hospital, Manhasset, New York [8 patients]). During the same period of this study, 7 patients underwent rotational atherectomy for calcified ULMCA disease (UCLA Medical Center [3 patients], St. Francis Hospital [0 patients], and North Shore University Hospital [4 patients]). Severely calcified vessels were defined by the presence of radioopacities on fluoroscopy involving both sides of the arterial wall. The decision to perform PCI with orbital atherectomy rather than CABG was left to the discretion of the treating physician. Patients underwent ULMCA-PCI if the cardiac surgeon felt the patient was too high a surgical risk, or due to the preference of the patient or referring physician. Patients were excluded if they presented with ST-elevation myocardial infarction within 72 hours prior to the intended PCI. The institutional review board at each site approved the review of the data. None of the patients in this registry were a part of the ORBIT II trial, which excluded patients with ULMCA disease.
Procedures and medical treatment. The coronary orbital atherectomy device has been previously described.8 The mechanism of action is differential sanding, whereby the eccentrically mounted, diamond-coated crown rotates over the Viper wire (Cardiovascular Systems, Inc) and laterally expands due to centrifugal force. The crown rotates at 80,000 rpm at low speed and 120,000 rpm at high speed.
Orbital atherectomy followed by stenting was performed via the transfemoral or transradial approach with standard techniques. Intravenous heparin to maintain the activated clotting time >250 seconds or bivalirudin was administered. The decisions to insert a temporary transvenous pacemaker, use intravascular ultrasound (IVUS), administer preprocedural intracoronary nitroglycerin, and implant drug-eluting vs bare-metal stent were at the discretion of the operator. The recommended duration of each pass was 20 seconds or less.
Dual-antiplatelet therapy was continued for at least 1 month for bare-metal stent and 1 year for drug-eluting stent. Optimal medical therapy, including beta-blockers, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, and statins, was given to patients unless contraindicated.
Study endpoints and clinical follow-up. The primary endpoint was a composite of major adverse cardiac and cerebrovascular events (cardiac death, myocardial infarction, stroke, and target-lesion revascularization) at 30 days. Death was considered cardiac in origin unless a non-cardiac origin was documented. Myocardial infarction was defined as recurrent symptoms with new ST-segment elevation or re-elevation of cardiac markers to at least twice the upper limit of normal. Target-lesion revascularization was defined as a repeat revascularization of the target lesion because of restenosis within the stent or in the 5 mm distal or proximal segments. Stent thrombosis was defined according to the Academic Research Consortium definition.11 Procedural success was defined as residual stenosis ≤30% and TIMI flow grade 3 without death, CABG, and/or PCI during the first 24 hours. Patient data were collected from medical records, and adverse clinical events were recorded in a dedicated PCI database.
Statistical analysis. Continuous variables are presented as mean ± standard deviation, and categorical variables are presented as numbers. Statistical analysis was performed with SAS software system (SAS Institute, Inc).
Results
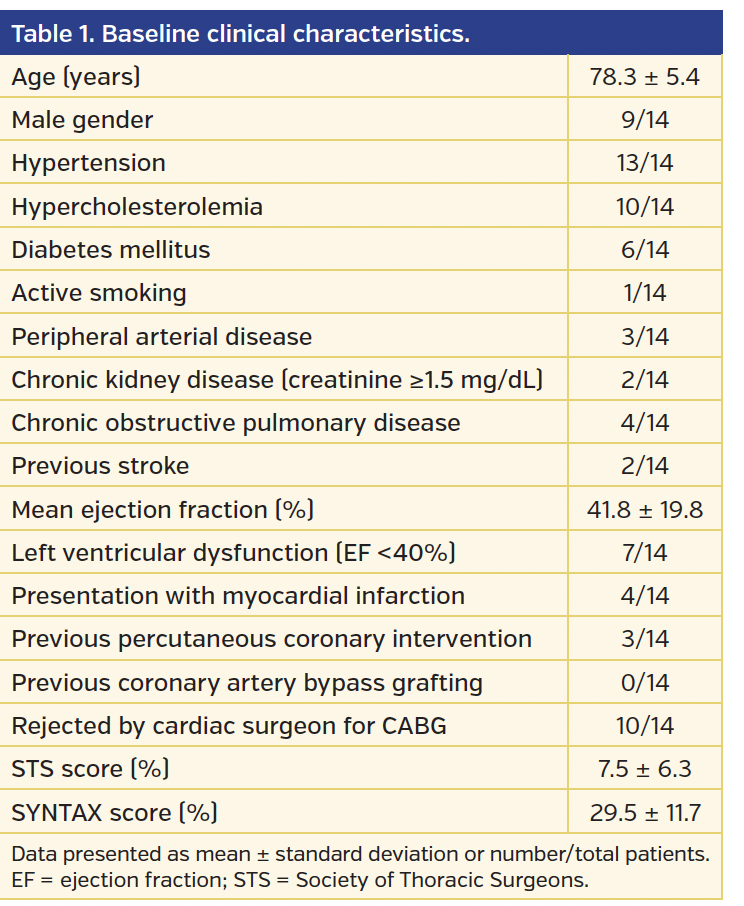
Baseline characteristics. The mean age was 78.3 ± 5.4 years and the majority of patients were male (Table 1). The mean ejection fraction was 41.8 ± 19.8%. The mean STS and SYNTAX scores were 7.5 ± 6.3 and 29.5 ± 11.7, respectively.
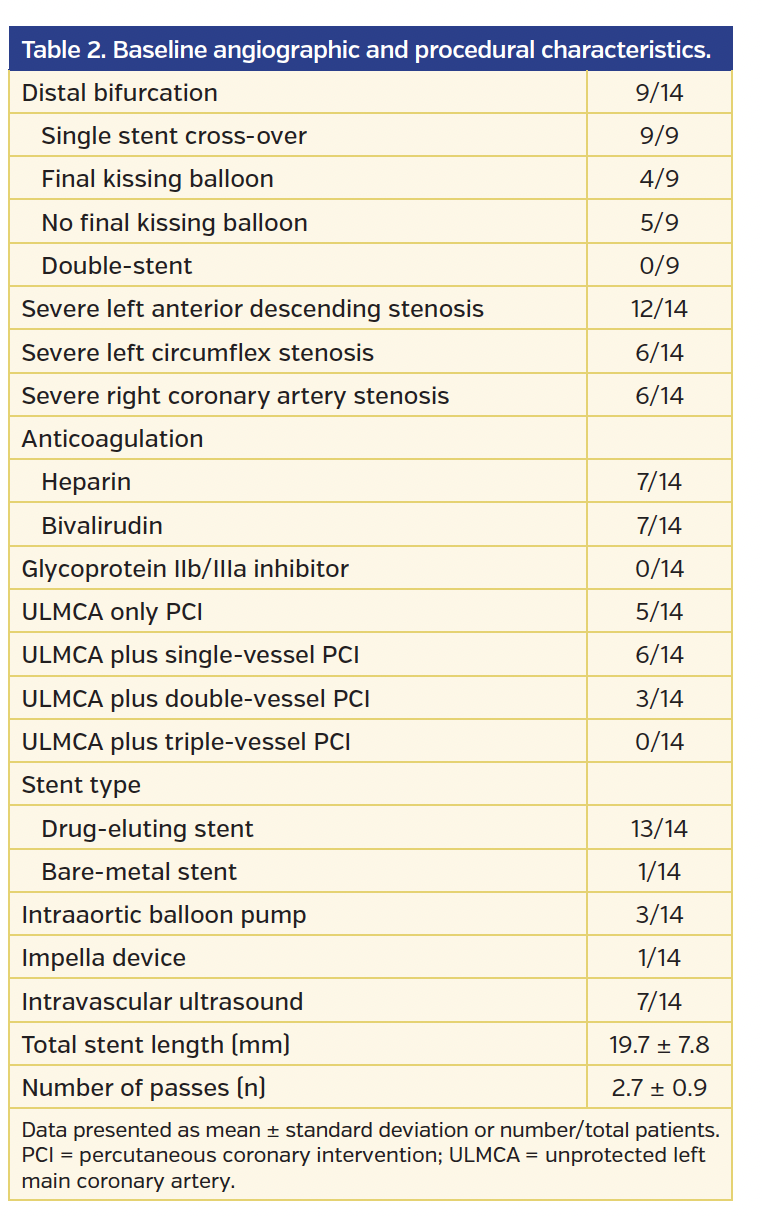
Distal bifurcation involvement was present in 9 of 14 patients (Table 2). Single stent cross-over technique was used in all 9 patients with distal bifurcation involvement, with 4 undergoing final simultaneous kissing-balloon inflation. Drug-eluting stents were used in all but 1 patient. The mean number of passes was 2.8 ± 0.8 per case.
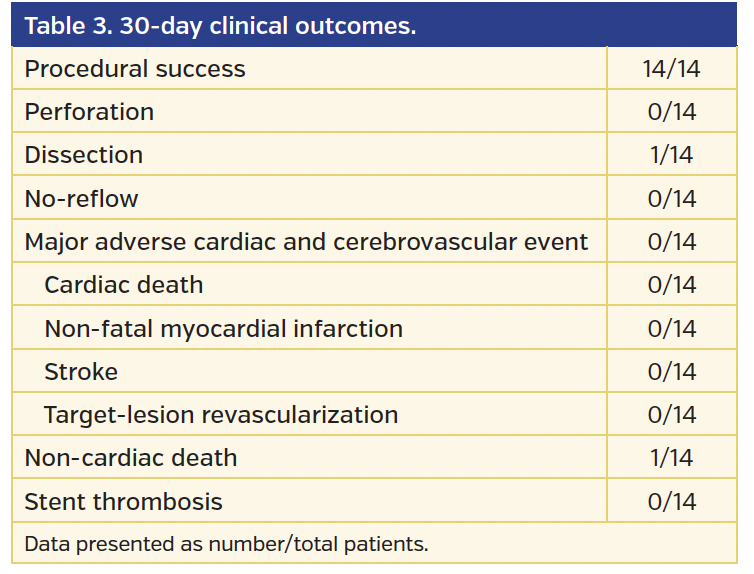
30-day clinical outcomes. Procedural success was achieved in all 14 patients (Table 3). One patient had periprocedural coronary artery dissection that was successfully treated with stenting. There was no stent thrombosis, perforation, spasm, or no-reflow. No patient experienced a major adverse cardiac and cerebrovascular event.
Discussion
Severely calcified ULMCA disease represents a highly complex lesion. Orbital atherectomy in patients with severely calcified ULMCA disease is feasible, even in high-risk patients who were considered poor surgical candidates.
Detection of the presence of severe coronary artery calcification is vital to successful PCI. Failure to recognize its presence prior to PCI can increase morbidity and mortality. Severely calcified lesions can increase the complexity of PCI due to the inability to fully dilate the lesion and expand the stent, increasing the risk of in-stent restenosis and stent thrombosis. The rationale for atherectomy in severely calcified lesions is plaque modification, leading to plaque reduction and enhancing the likelihood of full stent dilation. Balloon angioplasty of severely calcified lesions may require high-pressure inflation to “crack” the lesion, possibly leading to a dissection at the junction of calcified and non-calcified tissues.12
Data are limited in patients with severely calcified lesions, as they are often excluded from randomized trials. Severe coronary artery calcification can be underdiagnosed. Imaging modalities to accurately assess the presence and severity of coronary artery calcification include IVUS and optical coherence tomography. IVUS can also be helpful to optimize results by assessing for stent expansion and apposition. A subgroup analysis of the MAIN-COMPARE registry demonstrated that IVUS-guided PCI was associated with a lower mortality at 3 years compared with conventional angiography-guided PCI after adjustment with propensity-score matching (6.3% vs 13.6%; log-rank P=.06; hazard ratio, 0.54; 95% confidence interval, 0.28-1.03).13
Although orbital atherectomy of severely calcified lesions adds to the procedure length and cost of the PCI, it may potentially decrease procedural time when one takes into consideration the added time of using multiple balloons to predilate the lesion to facilitate stent delivery and postdilate the stent if underexpanded. Therefore, it may reduce the length of stay in the hospital, readmission rates, and long-term complications. The rate of target-lesion revascularization in the ORBIT II trial was 6.2% at 2-year follow-up.10
A potential advantage of orbital atherectomy is that PCI can be performed faster than with rotational atherectomy. Typically, the set-up time for orbital atherectomy is approximately 2 minutes. The set-up time for rotational atherectomy is longer given that there are more components, such as the nitrogen tank and a pedal to activate the burr. It also requires calibration to test the speed of the burr. Unlike rotational atherectomy, which requires a change to different burrs to achieve a larger lumen size, orbital atherectomy has only one crown that can provide more atherectomy at higher rotational speeds. Obviating the need to upsize to a larger crown leads to shorter procedural and fluoroscopy times. The left main coronary artery is a large-diameter vessel (approximately 4 mm in diameter). Another advantage of orbital atherectomy is that the particles liberated are <2 µm, while the particle size created by rotational atherectomy is 5-10 µm; this potentially lowers the risk of distal embolization and slow or no-reflow, maintaining coronary perfusion.14,15 Another factor behind the lower likelihood of slow or no-reflow is that the crown orbits elliptically. This may allow blood and microparticles to flow around the crown, minimizing the risk of thermal injury. In contrast, rotational atherectomy utilizes a concentric burr that does not allow blood and microparticles to flow past the burr. Slow or no-reflow during ULMCA-PCI may be particularly catastrophic and lead to hemodynamic and electrical instability given that the ULMCA subtends a large area of myocardium.
Data on ULMCA-PCI with rotational atherectomy are limited. Yabushita et al reported a 30-day mortality rate of 3.1% in 64 patients who underwent ULMCA-PCI with rotational atherectomy.6 The 30-day mortality in patients who underwent CABG in the SYNTAX trial was 2.0%.2
Patients with severe left ventricular dysfunction may be at higher risk for slow or no-reflow. Our study included 8 high-risk patients (61.5%) who received consultation from cardiac surgery and were not considered to be candidates for surgical revascularization. Six patients (46.2%) had severe left ventricular dysfunction and underwent orbital atherectomy with hemodynamic support device including intraaortic balloon pump (23.1%) or Impella left ventricular assist device (7.7%). No patients developed slow or no-reflow.
Study limitations. This was a small, non-randomized, retrospective analysis with short-term follow-up. Comparison with surgical revascularization, the gold standard for the treatment of ULMCA disease, was not performed. Furthermore, neither comparison with rotational atherectomy nor PCI without atherectomy was performed. Risk stratification with SYNTAX, STS, and Parsonnet scores was not calculated. Quantitative coronary angiography was not performed. The determination of the severity of calcification was not standardized or performed by an angiographic core laboratory. Rather, angiographic calcification was determined by the individual investigator. Therefore, outcomes with patients with extremely calcified and longer lesions may be more complex and have worse outcomes compared with patients who have short calcified lesions. Periprocedural cardiac biomarkers were not obtained for all patients. Therefore, the incidence of myocardial infarction could have been underdiagnosed.
Conclusion
High-risk PCI can be performed safely and effectively with orbital atherectomy in patients with severely calcified ULMCA disease, many of whom have significant comorbidities that render them poor surgical candidates. Plaque modification with orbital atherectomy facilitates stent delivery and optimal stent expansion. A large, prospective, randomized trial is needed to determine the optimal treatment strategy for high-risk patients within this complex lesion subset.
References
1. Levine GN, Bates ER, Blankenship JC, et al; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58:e44-e122.
2. Morice MC, Serruys PW, Kappetein AP, et al. Outcomes in patients with de novo left main disease treated with either percutaneous coronary intervention using paclitaxel-eluting stents or coronary artery bypass graft treatment in the synergy between percutaneous coronary intervention with TAXUS and cardiac surgery (SYNTAX) trial. Circulation. 2010;121:2645-2653.
3. Williams M, Shaw LJ, Raggi P, et al. Prognostic value of number and site of calcified coronary lesions compared with the total score. JACC Cardiovasc Imaging. 2008;1:61-69.
4. Bangalore S, Vlachos HA, Selzer F, et al. Percutaneous coronary intervention of moderate to severe calcified coronary lesions: insights from the National Heart, Lung, and Blood Institute Dynamic Registry. Catheter Cardiovasc Interv. 2011;77:22-28.
5. Abdel-Wahab M, Richardt G, Joachim Buttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2013;6:10-19.
6. Yabushita H, Takagi K, Tahara S, et al. Impact of rotational atherectomy on heavily calcified, unprotected left main disease. Circ J. 2014;78:1867-1872.
7. Garcia-Lara J, Pinar E, Valdesuso R, et al. Percutaneous coronary intervention with rotational atherectomy for severely calcified unprotected left main: immediate and two-years follow-up results. Catheter Cardiovasc Interv. 2012;80:215-220.
8. Chambers JW, Feldman RL, Himmelstein SI, et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv. 2014;7:510-518.
9. Généreux P, Lee AC, Kim CY, et al. Orbital atherectomy for treating de novo severely calcified coronary narrowing (1-Year results from the pivotal ORBIT II Trial). Am J Cardiol. 2015;115:1685-1690.
10. Chambers J. Orbital atherectomy treatment of severely calcified coronary lesions: two year results of the ORBIT II trial and long-term economic analysis. SCAI Scientific Sessions. May 7, 2015.
11. Cutlip DE, Windecker S, Mehran R, et al; Academic Research Consortium. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115:2344-2351.
12. Fitzgerald PJ, Ports TA, Yock PG. Contribution of localized calcium deposits to dissection after angioplasty: an observational study using intravascular ultrasound. Circulation. 1992;86:64-70.
13. Park SJ, Kim YH, Park DW, et al. Impact of intravascular ultrasound guidance on long-term mortality in stenting for unprotected left main coronary artery stenosis. Circ Cardiovasc Interv. 2009;2:167-177.
14. Kini A, Marmur JD, Duvvuri S, Dangas G, Choudhary S, Sharma SK. Rotational atherectomy: improved procedural outcome with evolution of technique and equipment. Single-center results of first 1,000 patients. Catheter Cardiovasc Interv. 1999;46:305-311.
15. Adams GL, Khanna PK, Staniloae CS, Abraham JP, Sparrow EM. Optimal techniques with the Diamondback 360° System achieve effective results for the treatment of peripheral arterial disease. J Cardiovasc Transl Res. 2011;4:220-229.
_______________________________________
From the ¹Division of Interventional Cardiology, UCLA Medical Center, Los Angeles, California; ²Division of Cardiology, North Shore University Hospital, Manhasset, New York; and ³Division of Cardiology, St. Francis Hospital, Roslyn, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Lee reports speaker’s bureau fees from CSI. Dr R. Shlofmitz reports consulting fees from CSI. Dr E. Shlofmitz reports stock ownership in CSI. Dr Kaplan reports no conflicts of interest regarding the content herein.
Manuscript submitted September 18, 2015, provisional acceptance given October 19, 2015, final version accepted November 18, 2015.
Address for correspondence: Dr Michael S. Lee, 100 Medical Plaza, Suite 630, Los Angeles, CA 90095. Email: mslee@mednet.ucla.edu











