

Percutaneous Repair of Anterior Mitral Leaflet Perforation
Abstract: A 59-year-old male underwent coronary artery bypass grafting and mitral ring annuloplasty 4 years ago. The procedure was complicated by sternal wound infection. Recently, he presented with multiple admissions for decompensated heart failure with volume overload and pulmonary edema. He was found to have severe mitral regurgitation (MR) and transesophageal echocardiography (TEE) demonstrated severe MR through an anterior mitral leaflet perforation. Due to high surgical risk, he was referred for transcatheter repair of his mitral valve. This case illustrates the first reported use of an Amplatzer atrial septal occluder device for percutaneous mitral leaflet repair using three-dimensional TEE guidance after prior surgical mitral ring annuloplasty repair.
J INVASIVE CARDIOL 2012;24:134–137
Key words: mitral leaflet perforation, mitral regurgitation, catheter-based interventions
_______________________________________________
Mitral leaflet perforation and mitral ring annuloplasty dehiscence occur rarely after surgical mitral valve repair, and are related to technical factors, suture failure, tissue quality, and endocarditis.1-3 For patients with clinical symptoms, surgical reintervention is generally warranted. However, reoperation after mitral valve repair or replacement is associated with a mortality rate that approaches 12%.2,4 Numerous case series and reports have described percutaneous approaches to the management of mechanical or bioprosthetic mitral paravalvular leaks.5,6 Although there has been one reported case of an anterior leaflet perforation treated with an Amplatzer septal occluder after aortic valve replacement, there have been no prior reports describing percutaneous repair of mitral leaflet perforation after surgical mitral valve annuloplasty repair.7 We describe a case of successful percutaneous repair of an anterior mitral leaflet perforation in a high-risk patient who had previously undergone mitral ring annuloplasty.
Case Description
 A 59-year-old man was referred to our institution for potential MitraClip (Abbott Vascular) therapy after he was found to have severe mitral regurgitation (MR) seen on transthoracic echocardiography. He had a history of coronary artery disease and functional MR, and underwent coronary artery bypass grafting and mitral annuloplasty (28 mm CG Future; Medtronic Inc.) 4 years prior at an outside institution. A permanent pacemaker was also implanted for advanced atrioventricular block. The procedure was complicated by a methicillin-resistant
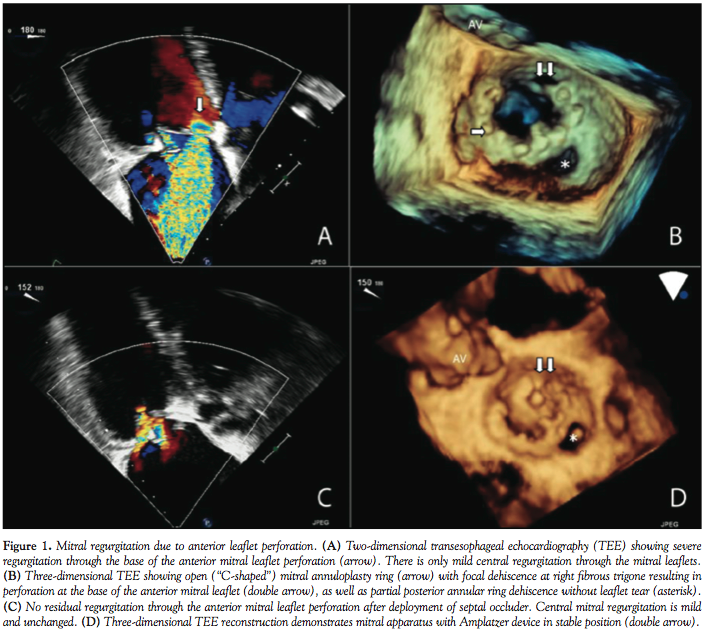
A 59-year-old man was referred to our institution for potential MitraClip (Abbott Vascular) therapy after he was found to have severe mitral regurgitation (MR) seen on transthoracic echocardiography. He had a history of coronary artery disease and functional MR, and underwent coronary artery bypass grafting and mitral annuloplasty (28 mm CG Future; Medtronic Inc.) 4 years prior at an outside institution. A permanent pacemaker was also implanted for advanced atrioventricular block. The procedure was complicated by a methicillin-resistant  staph aureus sternal wound infection requiring multiple debridements and wound vacuum drainage for 1 year. There was no documented bacteremia at that time. Three years later, he had several admissions for decompensated heart failure, volume overload, and pulmonary edema without angina pectoris. Transthoracic echocardiogram revealed left ventricular (LV) ejection fraction of 55%, severe MR with 2 distinct regurgitant jets, and an estimated right ventricular pulmonary systolic pressure of 60 mm Hg. Subsequent transesophageal echocardiography (TEE) demonstrated a dilated mitral annulus with the septal-lateral dimension measuring 36 mm. There was significant dehiscence of the annuloplasty ring from the posterior annulus and focal dehiscence at the right fibrous trigone, with a resultant 6 x 8 mm perforation at the base of the anterior mitral leaflet (Figure 1). There was 4+ MR through the mitral leaflet perforation and 1+ central MR. There was trivial regurgitation through the posterior dehiscence (Figure 2). After referral to our center, 3.5 years after the original operation, several blood cultures drawn on different days were negative and an erythrocyte sedimentation rate was normal. Angiography demonstrated occluded vein grafts to the left circumflex and right coronary arteries with severe native diffuse disease not amenable to percutaneous or surgical revascularization. The left internal mammary artery graft to left anterior descending artery was patent. In view of his related comorbidities and prior sternal wound infection, percutaneous repair of the anterior mitral leaflet perforation was performed.
staph aureus sternal wound infection requiring multiple debridements and wound vacuum drainage for 1 year. There was no documented bacteremia at that time. Three years later, he had several admissions for decompensated heart failure, volume overload, and pulmonary edema without angina pectoris. Transthoracic echocardiogram revealed left ventricular (LV) ejection fraction of 55%, severe MR with 2 distinct regurgitant jets, and an estimated right ventricular pulmonary systolic pressure of 60 mm Hg. Subsequent transesophageal echocardiography (TEE) demonstrated a dilated mitral annulus with the septal-lateral dimension measuring 36 mm. There was significant dehiscence of the annuloplasty ring from the posterior annulus and focal dehiscence at the right fibrous trigone, with a resultant 6 x 8 mm perforation at the base of the anterior mitral leaflet (Figure 1). There was 4+ MR through the mitral leaflet perforation and 1+ central MR. There was trivial regurgitation through the posterior dehiscence (Figure 2). After referral to our center, 3.5 years after the original operation, several blood cultures drawn on different days were negative and an erythrocyte sedimentation rate was normal. Angiography demonstrated occluded vein grafts to the left circumflex and right coronary arteries with severe native diffuse disease not amenable to percutaneous or surgical revascularization. The left internal mammary artery graft to left anterior descending artery was patent. In view of his related comorbidities and prior sternal wound infection, percutaneous repair of the anterior mitral leaflet perforation was performed.
 The procedure was performed under general anesthesia with three-dimensional TEE guidance, and periprocedural prophylactic antibiotics were given. The anterior mitral leaflet perforation measured 6 x 8 mm (area, 0.37 cm2), and the anterior mitral leaflet length was measured at 22 mm. As the left atrial (left ventricular, for this case) disc for a 5 mm Amplatzer septal occluder (St. Jude Medical) was 17 mm, it was felt that the device would not restrict the motion of the leaflet and still adequately seal the perforation.
The procedure was performed under general anesthesia with three-dimensional TEE guidance, and periprocedural prophylactic antibiotics were given. The anterior mitral leaflet perforation measured 6 x 8 mm (area, 0.37 cm2), and the anterior mitral leaflet length was measured at 22 mm. As the left atrial (left ventricular, for this case) disc for a 5 mm Amplatzer septal occluder (St. Jude Medical) was 17 mm, it was felt that the device would not restrict the motion of the leaflet and still adequately seal the perforation.
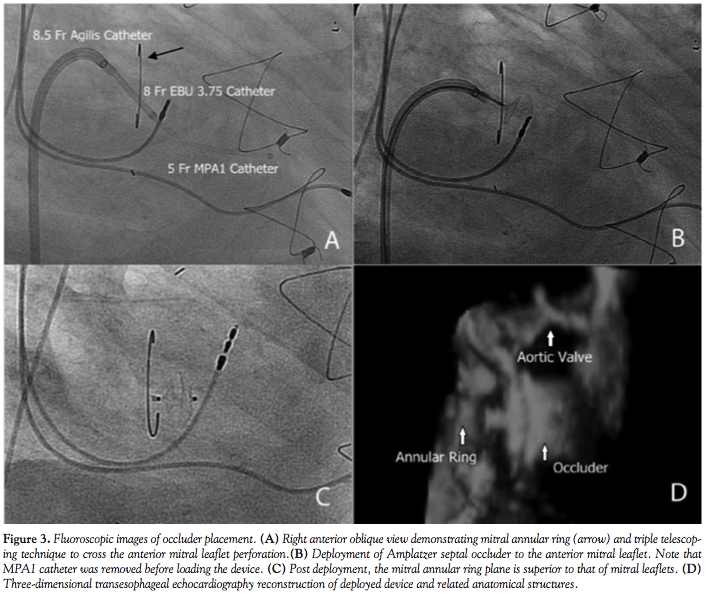
 Initially, right heart catheterization was performed that demonstrated pulmonary arterial pressure of 40/20 with mean pulmonary capillary wedge pressure of 18 mm Hg and V waves up to 22 mm Hg. Simultaneously, left heart catheterization revealed LV end diastolic pressure of 17 mm Hg, ruling out mitral stenosis. A BRK needle (St. Jude Medical) was used to perform transseptal puncture under echocardiographic guidance and a Mullins transseptal sheath (Medtronic Inc.) was advanced through the interatrial septum in a superior location within the fossa ovalis. Intravenous heparin was given at this point. Mean left atrial pressure was recorded at 18 mm Hg with prominent V waves up to 40 mm Hg. The Mullins sheath was then removed and a medium curl Agilis NxT catheter (11.5 Fr outer diameter, 8.5 Fr inner diameter, St. Jude Medical) was advanced into the left atrium and directed toward the base of the anterior mitral leaflet. Through the Agilis catheter, an 8 Fr EBU 3.75 guiding catheter (Medtronic Inc.) was then advanced to its tip. Another multipurpose catheter was then nested through the guiding catheter using a triple telescoping “mother and child” approach. An exchange-length 0.035˝ angled Glidewire (Terumo Medical Corporation) was then advanced through the leaflet perforation using three-dimensional TEE guidance in an antegrade fashion. Over the Glidewire, the multipurpose catheter was passed through the defect into the LV apex. The Glidewire was then exchanged for an Amplatz Superstiff wire (Boston Scientific), over which the EBU guiding catheter was advanced in the LV cavity (Figure 2). Once the guiding catheter was appropriately positioned in the LV midcavity, the multipurpose catheter as well as the stiff wire were removed. Then, a 5 mm Amplatzer atrial septal occluder was loaded into the guiding catheter and deployed successfully to the anterior mitral leaflet perforation under TEE guidance (Figure 3). On color Doppler, there was no residual MR through the leaflet perforation and only 1+ functional (central) MR with excellent device stability (Figures 1 and 4). The anterior mitral leaflet had preserved mobility and there was no obstruction of the LVOT (Figure 4). Mean left atrial pressure after the repair was 15 mm Hg with diminished V waves. Final transmitral gradient was 4 mm Hg with mitral valve area of 2.5 cm2. Procedural fluoroscopy time was 27 minutes. The postprocedure course was uneventful and the patient was discharged on aspirin and clopidogrel on postprocedure day 1. At 1-month follow-up, he was in New York Heart Association functional class I. He developed transient mild hemolytic anemia, which did not require transfusion. On follow-up echocardiogram, there was no residual MR through the defect and only 1+ central MR.
Initially, right heart catheterization was performed that demonstrated pulmonary arterial pressure of 40/20 with mean pulmonary capillary wedge pressure of 18 mm Hg and V waves up to 22 mm Hg. Simultaneously, left heart catheterization revealed LV end diastolic pressure of 17 mm Hg, ruling out mitral stenosis. A BRK needle (St. Jude Medical) was used to perform transseptal puncture under echocardiographic guidance and a Mullins transseptal sheath (Medtronic Inc.) was advanced through the interatrial septum in a superior location within the fossa ovalis. Intravenous heparin was given at this point. Mean left atrial pressure was recorded at 18 mm Hg with prominent V waves up to 40 mm Hg. The Mullins sheath was then removed and a medium curl Agilis NxT catheter (11.5 Fr outer diameter, 8.5 Fr inner diameter, St. Jude Medical) was advanced into the left atrium and directed toward the base of the anterior mitral leaflet. Through the Agilis catheter, an 8 Fr EBU 3.75 guiding catheter (Medtronic Inc.) was then advanced to its tip. Another multipurpose catheter was then nested through the guiding catheter using a triple telescoping “mother and child” approach. An exchange-length 0.035˝ angled Glidewire (Terumo Medical Corporation) was then advanced through the leaflet perforation using three-dimensional TEE guidance in an antegrade fashion. Over the Glidewire, the multipurpose catheter was passed through the defect into the LV apex. The Glidewire was then exchanged for an Amplatz Superstiff wire (Boston Scientific), over which the EBU guiding catheter was advanced in the LV cavity (Figure 2). Once the guiding catheter was appropriately positioned in the LV midcavity, the multipurpose catheter as well as the stiff wire were removed. Then, a 5 mm Amplatzer atrial septal occluder was loaded into the guiding catheter and deployed successfully to the anterior mitral leaflet perforation under TEE guidance (Figure 3). On color Doppler, there was no residual MR through the leaflet perforation and only 1+ functional (central) MR with excellent device stability (Figures 1 and 4). The anterior mitral leaflet had preserved mobility and there was no obstruction of the LVOT (Figure 4). Mean left atrial pressure after the repair was 15 mm Hg with diminished V waves. Final transmitral gradient was 4 mm Hg with mitral valve area of 2.5 cm2. Procedural fluoroscopy time was 27 minutes. The postprocedure course was uneventful and the patient was discharged on aspirin and clopidogrel on postprocedure day 1. At 1-month follow-up, he was in New York Heart Association functional class I. He developed transient mild hemolytic anemia, which did not require transfusion. On follow-up echocardiogram, there was no residual MR through the defect and only 1+ central MR.
Discussion
MR is one of the most commonly encountered valvular lesions in clinical practice, with 6.4% of the general population ≥65 years having at least moderate MR.8 Moderate-severe MR is present in 15-30% of patients with congestive heart failure and up to 12% of patients within 1 month after myocardial infarction. Since MR severity has been positively correlated with the subsequent development of heart failure and death, patients are often referred for surgical or percutaneous repair.9-12 The patient we have presented had functional MR (FMR), which is a consequence of underlying LV dysfunction or annular dilation. These derangements in the mitral apparatus impair the coaptation of leaflets which are otherwise structurally normal. Surgical correction of FMR with mitral annuloplasty rings has been shown to improve functional class and LV remodeling, but a survival benefit has yet to be proven.13,14 Additionally, even with current surgical annuloplasty techniques, up to 35% of treated patients have moderate or greater MR recur within 1 year of surgery.15-17
Because of the technical complexity of mitral valve repair, these remain challenging procedures for the cardiovascular surgeon. Mechanisms of late mitral repair failure include progression of degenerative changes of the leaflets and chordae tendineae, suture dehiscence, and endocarditis.1,18 As endocarditis is often associated with cardiac valve leaflet perforation and erosion, infection must be excluded in all patients with leaflet perforation, suture dehiscence, or paravalvular leak. In the reported case, multiple blood cultures drawn over several weeks after referral to our center were negative, and no vegetations were seen on TEE. The perforation in this case could have been the result of excessive suture tension, or from prior endocarditis following the original surgery complicated by severe sternal infection. Surgical intervention for leaflet perforation remains the treatment of choice in most patients. Sareyyupoglu and colleagues reported a series of 26 subjects with anterior mitral leaflet perforation who underwent surgical repair.19 Ninety-two percent of these patients had a history of endocarditis. Surgical repair with primary suture closure (n = 15) or patch repair (n = 11) was decided by measuring the area of the defect. Larger perforations (>1.5 cm2) were more likely to be repaired with a patch than primary suture closure. Both surgical techniques demonstrated excellent durability and procedural safety. In the absence of active infection, smaller perforations, as in our reported case, might be effectively repaired with percutaneous approach as smaller devices are less likely to restrict normal leaflet excursion or cause LVOT obstruction.
For percutaneous leaflet repair, high-quality two-and three-dimensional TEE are essential to delineate defect dimensions and motion of the anterior mitral leaflet in relation to the left ventricular outflow tract (LVOT). We utilized real-time three-dimensional TEE of the mitral valve as well as fluoroscopy to direct the guiding catheter and deploy the device. A triple-telescoping catheter technique that has been previously described was used to cross the very medial and somewhat posterior defect.20 For device selection, it is important to consider the diameters of the waist and two retention discs. We chose an Amplatzer septal occluder due to the very low profile and small disc diameters, which minimized the potential of restricting leaflet motion or obstructing the LVOT. Although use of an Amplatzer vascular plug has been described for a mitral leaflet perforation as a complication of mechanical aortic valve replacement, this device has substantial height and may not be the ideal choice for patching a leaflet perforation.7
In summary, percutaneous repair of mitral leaflet perforation is feasible and has acute safety in appropriately selected patients at high risk for surgery. Further investigation is required to establish mid- and longer-term durability of this approach.
References
- Gillinov AM, Cosgrove DM, Lytle BW, et al. Reoperation for failure of mitral valve repair. J Thorac Cardiovasc Surg. 1997;113(3):467-473; discussion 473-475.
- Cerfolio RJ, Orzulak TA, Pluth JR, Harmsen WS, Schaff HV. Reoperation after valve repair for mitral regurgitation: early and intermediate results. J Thorac Cardiovasc Surg. 1996;111(6):1177-1183; discussion 1183-1184.
- DiBardino DJ, ElBardissi AW, McClure RS, Razo-Vasquez OA, Kelly NE, Cohn LH. Four decades of experience with mitral valve repair: analysis of differential indications, technical evolution, and long-term outcome. J Thorac Cardiovasc Surg. 2010;139(1):76-83; discussion 83-84.
- Echevarria JR, Bernal JM, Rabasa JM, Morales D, Revilla Y, Revuelta JM. Reoperation for bioprosthetic valve dysfunction. A decade of clinical experience. Eur J Cardiothorac Surg. 1991;5(10):523-526; discussion 527.
- Kim MS, Casserly IP, Garcia JA, Klein AJ, Salcedo EE, Carroll JD. Percutaneous transcatheter closure of prosthetic mitral paravalvular leaks: are we there yet? JACC Cardiovasc Interv. 2009;2(2):81-90.
- Sorajja P, Cabalka AK, Hagler DJ, et al. Successful percutaneous repair of perivalvular prosthetic regurgitation. Catheter Cardiovasc Interv. 2007;70(6):815-823.
- Velasco S, Larman M, Eneriz M. Percutaneous closure of a native mitral valve perforation. Rev Esp Cardiol. 2010;63(5):597.
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005-1011.
- Bursi F, Enriquez-Sarano M, Nkomo VT, et al. Heart failure and death after myocardial infarction in the community: the emerging role of mitral regurgitation. Circulation. 2005;111(3):295-301.
- Robbins JD, Maniar PB, Cotts W, Parker MA, Bonow RO, Gheorghiade M. Prevalence and severity of mitral regurgitation in chronic systolic heart failure. Am J Cardiol. 2003;91(3):360-362.
- Trichon BH, Felker GM, Shaw LK, Cabell CH, O’Connor CM. Relation of frequency and severity of mitral regurgitation to survival among patients with left ventricular systolic dysfunction and heart failure. Am J Cardiol. 2003;91(5):538-543.
- Feldman T, Foster E, Glower DG, et al. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med. 2011;364:1395-1406.
- Bax JJ, Braun J, Somer ST, et al. Restrictive annuloplasty and coronary revascularization in ischemic mitral regurgitation results in reverse left ventricular remodeling. Circulation. 2004;110(11 Suppl 1):II103-II108.
- Wu AH, Aaronson KD, Bolling SF, Pagani FD, Welch K, Koelling TM. Impact of mitral valve annuloplasty on mortality risk in patients with mitral regurgitation and left ventricular systolic dysfunction. J Am Coll Cardiol. 2005;45(3):381-387.
- Hung J, Papakostas L, Tahta SA, et al. Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: continued LV remodeling as a moving target. Circulation. 2004;110(11 Suppl 1):II85-II90.
- Marwick TH. Restrictive annuloplasty for ischemic mitral regurgitation: too little or too much? J Am Coll Cardiol. 2008;51(17):1702-1703.
- McGee EC, Gillinov AM, Blackstone EH, et al. Recurrent mitral regurgitation after annuloplasty for functional ischemic mitral regurgitation. J Thorac Cardiovasc Surg. 2004;128(6):916-924.
- Marwick TH, Stewart WJ, Currie PJ, Cosgrove DM. Mechanisms of failure of mitral valve repair: an echocardiographic study. Am Heart J. 1991;122(1 Pt 1):149-156.
- Sareyyupoglu B, Schaff HV, Suri RM, Connolly HM, Daly RC, Orszulak TA. Safety and durability of mitral valve repair for anterior leaflet perforation. J Thorac Cardiovasc Surg. 2010;139(6):1488-1493.
- Yuksel UC, Tuzcu EM, Kapadia SR. Percutaneous closure of a postero-medial mitral paravalvular leak: the triple telescopic system. Catheter Cardiovasc Interv. 2011;77(2):281-285.
_______________________________________________
From the Division of Cardiovascular Medicine, University of California, Davis Medical Center, Sacramento, California.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. Rogers discloses that he is a consultant for St. Jude Medical. No other authors report disclosures regarding the content herein.
Manuscript submitted September 6, 2011, provisional acceptance given September 16, 2011, final version accepted October 19, 2011.
Address for correspondence: Jason H. Rogers, MD, 4860 Y Street, Suite 2820, Sacramento, CA 95817. Email: jason.rogers@ucdmc.ucdavis.edu









