Percutaneous Treatment of Delayed Post-Atherectomy Superficial Femoral Artery Pseudoaneurysm
ABSTRACT: SilverHawk atherectomy is commonly used in lower extremity percutaneous interventions. Minor perforations during SilverHawk atherectomy procedures are reported at a range of 0.8%. There are few reported cases in the literature about very late pseuodoaneursym formation after SilverHawk atherectomy. Herein we report a very unusual, late, concealed, acute rupture of superficial femoral artery with a large, painful pseuodoaneursym formation, 1 week after SilverHawk atherectomy and its treatment with Viabahn stent graft (W.L. Gore & Associates).
J INVASIVE CARDIOL 2012;24(10):E212–E214
Key words: SilverHawk atherectomy,pseudoaneurysm, Viabahn
________________________________________________
SilverHawk atherectomy (ev3 Endovascular) is commonly used in lower extremity percutaneous interventions. Although perforations, dissections, and embolism are among the known complications of revascularization with SilverHawk atherectomy,1 pseudoaneurysm formation of the superficial femoral artery (SFA) after atherectomy is a rare complication.2,3 The exact etiology of aneurysm formation following atherectomy has not been ascertained, but current theories identify mechanical factors including an oversized atherectomy device, tortuous nature of the vessel, and location of the lesion near side branches.3 We report a case of a patient who developed a fusiform aneurysm in the proximal SFA after SilverHawk antherectomy, which was successfully treated with a Viabahn stent graft.
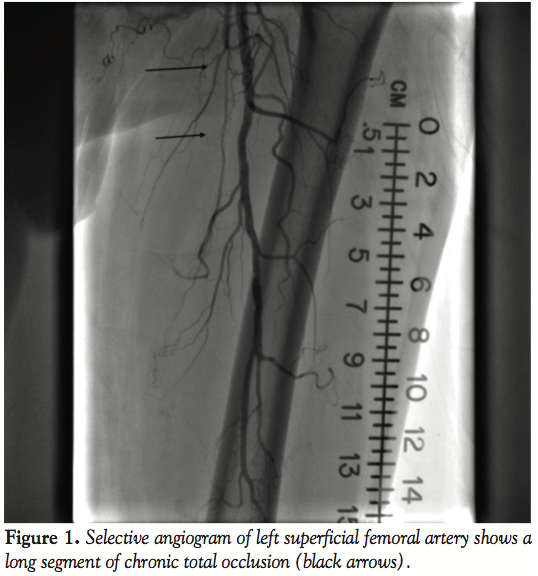 Case Report. A 70-year-old white male with history of hypertension, hyperlipidemia, coronary artery disease, prior bypass surgery, tobacco abuse, and severe peripheral vascular disease was seen in-clinic for class IV claudication with ischemic rest pain. Patient had been on appropriate medical management including an exercise regimen for approximately 9 months with no improvement in symptoms. He underwent a peripheral angiogram that showed chronic total occlusion (CTO) of the right and SFA (Figure 1). Since the left SFA
Case Report. A 70-year-old white male with history of hypertension, hyperlipidemia, coronary artery disease, prior bypass surgery, tobacco abuse, and severe peripheral vascular disease was seen in-clinic for class IV claudication with ischemic rest pain. Patient had been on appropriate medical management including an exercise regimen for approximately 9 months with no improvement in symptoms. He underwent a peripheral angiogram that showed chronic total occlusion (CTO) of the right and SFA (Figure 1). Since the left SFA  was more symptomatic, we proceeded with a left SFA intervention. After anticoagulation with bivalirudin, the lesion was crossed with a combination of a Terumo glidewire (Terumo Corporation) and a Confianza Pro wire (Abbott Vascular) with Trailblazer catheter (ev3 Endovascular) support. After confirmation of the distal end being in the true lumen by contrast injection through the Trailblazer catheter, atherectomy was performed with a TurboHawk LX-C device (ev3) followed by balloon angioplasty with a 5.0 mm x 120 mm EverCross balloon (ev3). There were no immediate complications and successful reduction of stenosis to <10% (Figure 2).
was more symptomatic, we proceeded with a left SFA intervention. After anticoagulation with bivalirudin, the lesion was crossed with a combination of a Terumo glidewire (Terumo Corporation) and a Confianza Pro wire (Abbott Vascular) with Trailblazer catheter (ev3 Endovascular) support. After confirmation of the distal end being in the true lumen by contrast injection through the Trailblazer catheter, atherectomy was performed with a TurboHawk LX-C device (ev3) followed by balloon angioplasty with a 5.0 mm x 120 mm EverCross balloon (ev3). There were no immediate complications and successful reduction of stenosis to <10% (Figure 2).
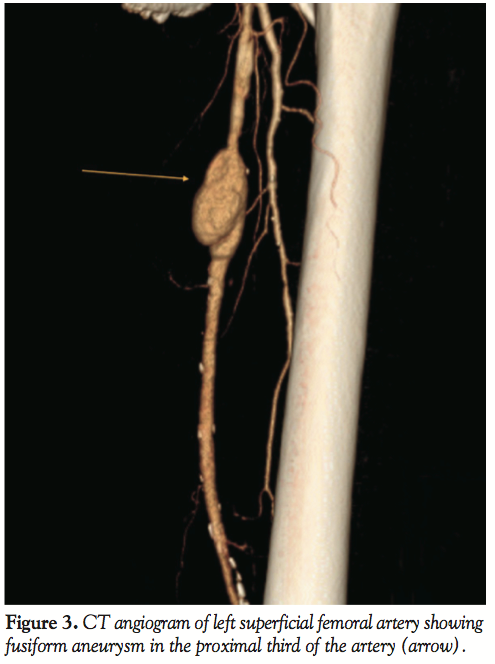 The patient was discharged home the following day without complications. A week later, the patient presented to the hospital with acute onset and worsening pain in his left thigh over the last 3 days and it was associated with ecchymosis and swelling. A CT angiography was performed and showed a fusiform aneurysm 4 cm x 27 mm diameter in the proximal third of the left SFA (Figure 3). Repeat angiogram confirmed the findings (Figure 4). Over a 0.014 ironman wire (Abbott Vascular), a 6.0 mm x 10 cm Viabahn endoprosthesis (W. L. Gore
The patient was discharged home the following day without complications. A week later, the patient presented to the hospital with acute onset and worsening pain in his left thigh over the last 3 days and it was associated with ecchymosis and swelling. A CT angiography was performed and showed a fusiform aneurysm 4 cm x 27 mm diameter in the proximal third of the left SFA (Figure 3). Repeat angiogram confirmed the findings (Figure 4). Over a 0.014 ironman wire (Abbott Vascular), a 6.0 mm x 10 cm Viabahn endoprosthesis (W. L. Gore 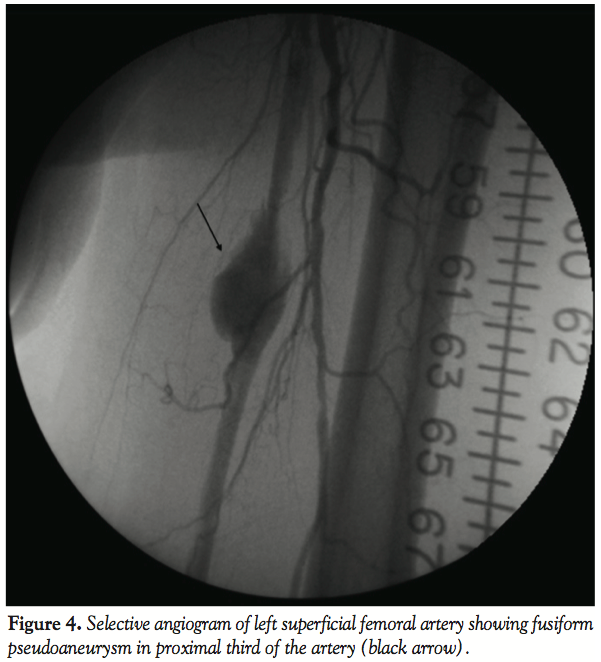 & Associates) was deployed and postdilated by a 6.0 mm x 40 cm balloon at nominal pressure at 9 atm. There was a persistent leak at the distal part of the aneurysm, so another 7.0 mm x 5 cm Viabahn stent was placed and again postdilated by a 6.0 mm x 40 mm compliant balloon at nominal pressure. Final angiogram showed successful exclusion of the pseudoaneurysm (Figure 5) and the patient tolerated the procedure well with no complications. One week later, the patient again presented to the hospital for worsening pain in his left thigh. Repeat CT angiography showed patent stent grafts with resolution of pseudoaneurysm. The patient’s symptoms improved by using a lidocaine patch and ibuprofen with no new symptoms in the 6 months follow-up.
& Associates) was deployed and postdilated by a 6.0 mm x 40 cm balloon at nominal pressure at 9 atm. There was a persistent leak at the distal part of the aneurysm, so another 7.0 mm x 5 cm Viabahn stent was placed and again postdilated by a 6.0 mm x 40 mm compliant balloon at nominal pressure. Final angiogram showed successful exclusion of the pseudoaneurysm (Figure 5) and the patient tolerated the procedure well with no complications. One week later, the patient again presented to the hospital for worsening pain in his left thigh. Repeat CT angiography showed patent stent grafts with resolution of pseudoaneurysm. The patient’s symptoms improved by using a lidocaine patch and ibuprofen with no new symptoms in the 6 months follow-up.
 Discussion. SilverHawk atherectomy (ev3) is an effective treatment in peripheral vascular disease with plaque excision and a gradual and progressive increase in lumen size. As the device is advanced through the lesion, plaque is excised and packed in the nosecone. Different planes of excision are achieved by rotation of the device. It can be used as stand-alone therapy or with balloon angioplasty/stenting. There are potential complications with atherectomy such as distal embolization, no flow, and ischemia.1 In the Treating Peripherals with SilverHawk: Outcomes Collection (TALON) Registry,1 perforation rate was 0.8%, ≥ grade C dissection 0.8%; 30-day occlusion and thrombosis rate was 0.1%. Directional atherectomy in coronary arteries has been associated with perforations4 and aneurysm formation in up to 10% of patients.5 However, after atherectomy there are only few reported cases of popliteal artery and SFA pseudoaneurysm formation in the literature.2,6 These interventions were done for complex plaque in both vessels without CTO and their presentations are not as dramatic as our patient. Our patient had acute onset of pain associated with ecchymosis and swelling after being ambulatory for several days, suggestive of late rupture of the SFA with pseudoaneursym formation. Atherectomy samples from peripheral arteries had 21% medial and 1% adventitial component of the arterial wall, which is much lower compared to coronary samples at 67% and 27%, respectively.7 Having a CTO and wire bias might have resulted in deeper cuts in our patient with weakening of the arterial wall and subsequent rupture as a result of increased mechanical stress associated with ambulation and arterial pressure.
Discussion. SilverHawk atherectomy (ev3) is an effective treatment in peripheral vascular disease with plaque excision and a gradual and progressive increase in lumen size. As the device is advanced through the lesion, plaque is excised and packed in the nosecone. Different planes of excision are achieved by rotation of the device. It can be used as stand-alone therapy or with balloon angioplasty/stenting. There are potential complications with atherectomy such as distal embolization, no flow, and ischemia.1 In the Treating Peripherals with SilverHawk: Outcomes Collection (TALON) Registry,1 perforation rate was 0.8%, ≥ grade C dissection 0.8%; 30-day occlusion and thrombosis rate was 0.1%. Directional atherectomy in coronary arteries has been associated with perforations4 and aneurysm formation in up to 10% of patients.5 However, after atherectomy there are only few reported cases of popliteal artery and SFA pseudoaneurysm formation in the literature.2,6 These interventions were done for complex plaque in both vessels without CTO and their presentations are not as dramatic as our patient. Our patient had acute onset of pain associated with ecchymosis and swelling after being ambulatory for several days, suggestive of late rupture of the SFA with pseudoaneursym formation. Atherectomy samples from peripheral arteries had 21% medial and 1% adventitial component of the arterial wall, which is much lower compared to coronary samples at 67% and 27%, respectively.7 Having a CTO and wire bias might have resulted in deeper cuts in our patient with weakening of the arterial wall and subsequent rupture as a result of increased mechanical stress associated with ambulation and arterial pressure.
A Viabahn covered stent was used to successfully treat the pseudoaneurysm in our patient. The Viabahn endoprosthesis is constructed of nitinol and expanded polytetrafluoroethylene (ePTFE) lining and has a proprietary heparin bioactive surface. It has been shown in observational studies and randomized trials to be an effective and safe treatment strategy compared to bare self-expanding stents and surgical prosthetic bypass grafts.8 A randomized prospective study showed comparable 1-year patency self-expanding ePTFE/nitinol stent graft vs surgical femoral-to-above knee popliteal artery bypass with synthetic graft material (73.4% vs 74.2%) in treating SFA occlusive disease.9 When Viabahn stent grafts were placed into 87 limbs in 76 patients for the treatment of atherosclerotic occlusive disease of the femoropopliteal obstruction with a mean lesion length of 14.2 cm, primary patency rates were 76% at 1 year and 55% at 4 years. Primary patency was independent of lesion length and type but dependent on device diameter (P=.001) with a 4-year, 82% patency rate in devices of at least 7 mm.10
The Viabahn stent has been used for treatment of pseudoaneurysms in the popliteal artery. In a single center study, 18 patients underwent endothelialization of popliteal pseudoaneurysms with the Viabahn endograft with patency and exclusion of aneurysm rate of 86% in 6 months.11 It has also been successfully used in to treat iatrogenic post-pacemaker axillary artery pseudoaneurysms12 and carotid artery pseudoaneurysms after carotid surgery or radical neck dissection.13-15 In animal studies, complete endothelialization inside ePTFE nitinol stents may take up to 6 months.16 Re-occlusions mostly occurred in the first year after Hemobahn/Viabahn endoprosthesis placement and 21% were in the first 30 days,17 which emphasizes the importance of antiplatelet therapy in these patients. Progression of other SFA lesions outside the Hemobahn/Viabahn endoprosthesis also increases the possibility of re-occlusion.17 Due to this, routine ABI/duplex ultrasound screening should be considered in follow-up.
Conclusion
As seen in our case, delayed perforations at the SilverHawk atherectomy site can occur after ambulation with associated symptoms of ecchymosis, pain, and swelling. Patients with such symptoms will require prompt evaluation of the atherectomy site. The Viabahn stent can be used as a treatment option for treatment of pseudoaneurysms in the SFA.
References
- Ramaiah V, Gammon R, Kiesz S, et al; for the TALON Registry. Midterm outcomes from the TALON Registry: treating peripherals with SilverHawk: outcomes collection. J Endovasc Ther. 2006;13(5):592-602.
- Nikam SD, Morgan JH, Zakhary EM, Galt SW, Elmore JR, Franklin DP. Native superficial femoral artery peripheral atherectomy site pseudoaneurysm: a case report. J Vasc Surg. 2007;46(3):565-568.
- Matsumoto AH, Selby JB Jr, Ladika JE Jr, Tegtmeyer CJ. Pseudoaneurysm formation following directional atherectomy. J Vasc Interv Radiol. 1993;4(2):283-286.
- Elliott JM, Berdan LG, Holmes DR, et al. One-year follow-up in the Coronary Angioplasty Versus Excisional Atherectomy Trial (CAVEAT I). Circulation. 1995;91(8):2158-2166.
- Oikawa Y, Yajima J, Angiolillo DJ, et al. Short- or long-term outcomes of coronary artery aneurysms occurring after directional coronary atherectomy. J Invasive Cardiol. 2008;20(4):159-160.
- Penugonda N, Duncan K, Schreiber T. Popliteal artery pseudoaneurysm following FoxHollow atherectomy: a rare complication. J Invasive Cardiol. 2008;20(9):477-478.
- Kaid KA, Gopinathapillai R, Qian F, Salvaji M, Wasty N, Cohen M. Analysis of particulate debris after superficial femoral artery atherectomy. J Invasive Cardiol. 2009;21(1):7-10.
- Kwa AT, Yeo KK, Laird JR. The role of stent-grafts for prevention and treatment of restenosis. J Cardiovasc Surg. 2010;51(4):579-589.
- Kedora J, Hohmann S, Garrett W, Munschaur C, Theune B, Gable D. Randomized comparison of percutaneous Viabahn stent grafts vs prosthetic femoral-popliteal bypass in the treatment of superficial femoral arterial occlusive disease. J Vasc Surg. 2007;45(1):10-16; discussion 16. Epub 2006 Nov 28.
- Saxon RR, Coffman JM, Gooding JM, Ponec DJ. Long-term patency and clinical outcome of the Viabahn stent-graft for femoropopliteal artery obstructions. J Vasc Interv Radiol. 2007;18(11):1341-1349; quiz 1350.
- Etezadi V, Fuller J, Wong S, et al. Endovascular treatment of popliteal artery aneurysms: a single-center experience. J Vasc Interv Radiol. 2010;21(6):817-823. Epub 2010 Apr 24.
- Weger N, Klaassen Z, Sturt C, Hertz S. Endovascular treatment of a pseudoaneurysm after an iatrogenic axillary artery injury. Ann Vasc Surg. 2010;24(6):826.e9-826.e12. Epub 2010 May 13.
- Elpiniki T, Salviato E, Rocca T, Braccini L, Galeotti R, Mascoli F. Heparin surface stent-graft for the treatment of a carotid pseudoaneurysm. Ann Vasc Surg. 2010;24(7):952.e9-952.e12. Epub 2010 Jul 6.
- Ahuja V, Tefera G. Successful covered stent-graft exclusion of carotid artery pseudo-aneurysm: two case reports and review of literature. Ann Vasc Surg. 2007;21(3):367-372.
- Golarz SR, Gable D. Use of a Viabahn stent for repair of a common carotid artery pseudoaneurysm and dissection. Ann Vasc Surg. 2010;24(4):550.e11-550.e13. Epub 2010 Feb 7.
- Virmani R, Kolodgie FD, Dake MD, et al. Histopathologic evaluation of an expanded polytetrafluoroethylene-nitinol stent endoprosthesis in canine iliofemoral arteries. J Vasc Interv Radiol. 1999;10(4):445-456.
- Fischer M, Schwabe C, Schulte KL. Value of the hemobahn/viabahn endoprosthesis in the treatment of long chronic lesions of the superficial femoral artery: 6 years of experience. J Endovasc Ther. 2006;13(3):281-290.
________________________________________________
From the LSU Health Sciences Center Shreveport, Division of Cardiovascular Diseases Shreveport, Louisiana.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted February 27, 2012, provisional acceptance given May 21, 2012, final version accepted May 30, 2012.
Address for correspondence: Nuri Ilker Akkus MD, FACC, LSU Health Sciences Center Shreveport, Division of Cardiovascular Diseases , 1501 Kings Highway, Shreveport, LA, 71103. Email:iakkus@hotmail.com