

Pericardiocentesis in Contemporary Practice
ABSTRACT: Objective. Pericardiocentesis is a life-saving procedure associated with a small, but significant, risk of major complication. An apical or subcostal approach may be used, although the relative complication rates are not reported. In modern practice, an increasing proportion of pericardial effusions occur as a result of catheter-laboratory related complications. This study examines current practice and analyzes the complications of pericardial drainage according to the route of approach. Design. Historical cohort study. Setting. Four Oxfordshire hospitals, including the John Radcliffe Hospital, a tertiary referral center. Patients. Local databases were searched to identify percutaneous pericardiocenteses carried out between November 2002 and October 2009. Results. A total of 188 pericardiocenteses were performed in 163 patients. Malignancy (55; 33.7%) and catheter-based cardiac procedures (45; 23.9%) were the most common causes of pericardial effusions requiring drainage. 50.0% of all pericardiocenteses were performed in patients who had received anticoagulant or antiplatelet agents the same day. This rose to 93.7% in patients whose effusions occurred as a complication of a catheter-based procedure. Nine complications occurred during the study period, giving an overall complication rate of 4.8%. Six of the complications occurred via the subcostal route and all 4 complications requiring surgery occurred via the subcostal route. Conclusion. The numbers of iatrogenic pericardial effusions occurring as a complication of catheter-based procedures mean that a significant proportion of pericardiocenteses are being performed in anticoagulated patients. This may alter the risk profile. Although complication rates were low for both routes, all major complications requiring surgery occurred via the subcostal approach. These data suggest an apical approach may be preferable where practical.
J INVASIVE CARDIOL 2011;23:234–239
Key words: pericardiocentesis, pericardial effusions
____________________________________________
Pericardiocentesis is a life-saving procedure associated with a small, but significant, risk of major complication.1 Historically, malignancy and uremia are the most common causes of pericardial effusions requiring drainage;2 more recent studies indicate that effusions occurring as a complication of percutaneous catheter-based procedures are increasing.3 It is unknown if the characteristics of the population undergoing pericardiocentesis are changing as a result.
Pericardiocentesis can be performed via an apical or subcostal approach.4 Traditionally, a subcostal approach was preferred, largely because this is considered the safest route without image guidance.4,5 The complication rates according to the route of approach have not been previously reported.
This historical cohort study examines the etiology and clinical outcomes of pericardial effusions in patients undergoing pericardiocentesis in contemporary practice, with particular emphasis on those effusions occurring as a result of percutaneous catheter-based procedures. It also analyzes the complications according to the route of approach.
Methods
 Data collection. Local databases (including echocardiography reports and records from the catheter laboratory, coronary care units and other procedure areas) were searched to identify percutaneous pericardiocenteses carried out across four Oxfordshire hospitals between November 2002 and October 2009. Data were collected from individual patient records.
Data collection. Local databases (including echocardiography reports and records from the catheter laboratory, coronary care units and other procedure areas) were searched to identify percutaneous pericardiocenteses carried out across four Oxfordshire hospitals between November 2002 and October 2009. Data were collected from individual patient records.
The four hospitals comprised a large tertiary referral center (John Radcliffe Hospital, Oxford) and three surrounding district general hospitals (Royal Berkshire Hospital, High Wycombe General Hospital and Milton Keynes General Hospital); the average number of procedures performed per annum in each hospital is shown in Table 1.
For each pericardiocentesis, the following data were collected: clinical presentation, etiology of the effusion, use of anticoagulant therapy and clotting parameters on the day of the procedure, approach route used to drain the effusion, procedural monitoring, volume drained, complications related to the procedure, date of death (if applicable) and nature of consent prior to drainage. Mortality data were confirmed by searching the National Health Service spine. Eleven patients were identified who underwent pericardiocentesis during the study period, but whose complete records were not available. These cases were excluded from subsequent analyses.
Patients were followed for a median of 17.3 months (interquartile range: 5.7–36.2 months).
Procedures and techniques. Pericardiocentesis was performed using the Seldinger technique with a 7 cm, 18 gauge needle and typically either ultrasound or fluoroscopic guidance. There was no standardized protocol for pericardiocentesis procedures at the time of data collection, so the approach route and procedural monitoring were at the operator’s discretion.
Definitions. A diagnosis of tamponade was based on a combination of clinical and echocardiographic findings, as documented in the patient record. Echocardiographic features of tamponade included right atrial or ventricular diastolic collapse or respiratory swing in the mitral or tricuspid valve inflow.
Statistical analysis. Results are given as mean ± standard deviation for continuous variables. Survival data are given as median ± interquartile range and survival analysis was performed using the Kaplan-Meier method. Categorical variables were compared using the Chi-squared test.
Results
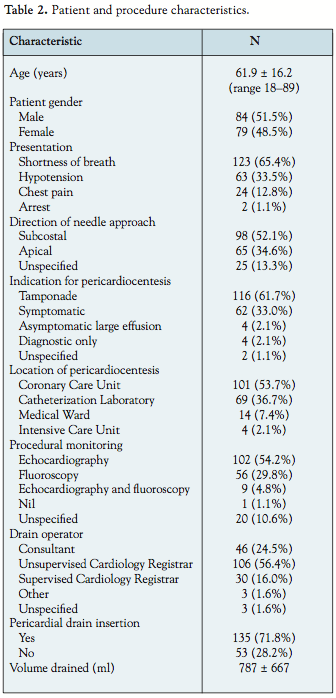 Patient and procedure characteristics. During the study period, 188 pericardiocenteses were performed in 163 patients. A total of 138 procedures were carried out at the John Radcliffe Hospital, 23 at High Wycombe Hospital, 21 at the Royal Berkshire Hospital, and 6 at Milton Keynes General Hospital. The patient and procedure characteristics are summarized in Table 2.
Patient and procedure characteristics. During the study period, 188 pericardiocenteses were performed in 163 patients. A total of 138 procedures were carried out at the John Radcliffe Hospital, 23 at High Wycombe Hospital, 21 at the Royal Berkshire Hospital, and 6 at Milton Keynes General Hospital. The patient and procedure characteristics are summarized in Table 2.
For those patients where the procedural monitoring was documented (167; 88.8%), all but one had echocardiography, fluoroscopy or both used as guidance. The patient for whom procedural monitoring was not used had experienced a cardiac arrest while in the Intensive Care Unit, with blind pericardiocentesis performed as a last resort.
Iatrogenic effusions. Cardiac surgery and other invasive cardiac procedures comprised the single largest cause of pericardial effusions requiring drainage (57; 35.0%). Twelve effusions occurred after cardiac surgery and required intervention between 5 and 90 days post-operatively; the median time to drainage was 34 days (inter-quartile range: 14–46 days). The effusions that were drained surgically are not included in this study.
Forty-five effusions occurred after a catheter-based procedure and two of these required repeat drainage. Twenty-three effusions were due to percutaneous coronary interventions, 15 were due to electrophysiological procedures, 6 were due to pacemaker insertion and 1 was due to percutaneous left atrial appendage closure. Twenty were diagnosed in the cardiac catheterization laboratory (44.4%); all of these patients had evidence of tamponade. For those presenting after completion of the procedure, all but 4 patients presented with tamponade. Overall, 91.5% of the effusions complicating catheter-based procedures presented with tamponade; this compares with the remainder of the study population, where 51.8% presented with tamponade (p < 0.0001). The median time to presentation was 5.0 hours (inter-quartile range: 2.0–40.5 hours). For effusions secondary to percutaneous coronary interventions, the cause of the effusion was specified in 16/23 cases (70.0%). Ten out of 16 (62.5%) were due to distal wire perforation, 2/16 (12.5%) occurred during rotablation, 2/16 (12.5%) occurred during balloon inflation and 2/16 (12.5%) occurred during stent placement.
 Anticoagulant and antiplatelet agents. Of the 47 pericardiocenteses that were performed for pericardial effusions secondary to a catheter-based procedure, 44 (93.6%) were carried out in patients who had received at least 1 antiplatelet or anticoagulant agent the same day. Twenty-one of these procedures (44.7%) were carried out in patients who had received 3 or more such drugs. For effusions due to all other causes, the equivalent figures are 50/141 (35.5%) for pericardiocenteses performed in patients taking 1 blood-thinning agent and 0/141 performed in patients taking 3 or more drugs (p < 0.0001). Table 3 shows a breakdown of these data by drug.
Anticoagulant and antiplatelet agents. Of the 47 pericardiocenteses that were performed for pericardial effusions secondary to a catheter-based procedure, 44 (93.6%) were carried out in patients who had received at least 1 antiplatelet or anticoagulant agent the same day. Twenty-one of these procedures (44.7%) were carried out in patients who had received 3 or more such drugs. For effusions due to all other causes, the equivalent figures are 50/141 (35.5%) for pericardiocenteses performed in patients taking 1 blood-thinning agent and 0/141 performed in patients taking 3 or more drugs (p < 0.0001). Table 3 shows a breakdown of these data by drug.
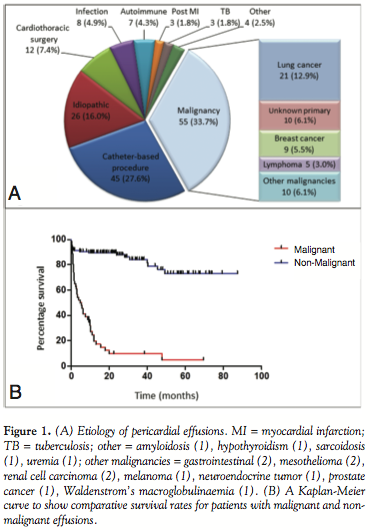 Pericardial effusions due to other causes. The underlying etiologies of all pericardial effusions requiring pericardiocentesis are shown in Figure 1A. Overall, malignancy and invasive cardiac procedures were the most common causes, jointly accounting for 68.7% of all pericardial effusions. Idiopathic effusions were the next most frequent (26; 16.0%); 5 patients in this group had a preceding febrile illness and a presumptive clinical diagnosis of viral pericarditis. Infection-related effusions (8; 4.9%) included 3 effusions that had confirmed bacteria on microscopy or culture from the pericardial fluid. The organisms isolated were Staphylococcus aureus, Streptococcus pneumoniae and diptheroids. They also included 5 reactive pericardial effusions that occurred after lower respiratory tract infections in 4 patients and meningococcal sepsis in 1. In these cases, the pericardial fluid was sterile.
Pericardial effusions due to other causes. The underlying etiologies of all pericardial effusions requiring pericardiocentesis are shown in Figure 1A. Overall, malignancy and invasive cardiac procedures were the most common causes, jointly accounting for 68.7% of all pericardial effusions. Idiopathic effusions were the next most frequent (26; 16.0%); 5 patients in this group had a preceding febrile illness and a presumptive clinical diagnosis of viral pericarditis. Infection-related effusions (8; 4.9%) included 3 effusions that had confirmed bacteria on microscopy or culture from the pericardial fluid. The organisms isolated were Staphylococcus aureus, Streptococcus pneumoniae and diptheroids. They also included 5 reactive pericardial effusions that occurred after lower respiratory tract infections in 4 patients and meningococcal sepsis in 1. In these cases, the pericardial fluid was sterile.
Of the 7 patients with autoimmune effusions, 4 were secondary to rheumatoid arthritis, 2 were secondary to systemic lupus erythematosus and 1 was secondary to dermatomyositis.
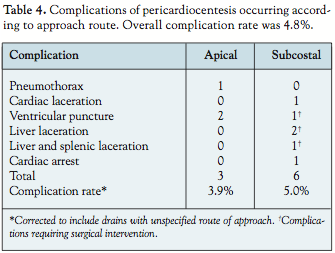 Complications. There were 9 significant complications as a result of pericardiocentesis recorded during the study period, giving an overall complication rate of 4.8% (Table 4). These comprised cardiac complications, including ventricular puncture, cardiac laceration and arrhythmias and damage to nearby organs, including the lung, liver and spleen.
Complications. There were 9 significant complications as a result of pericardiocentesis recorded during the study period, giving an overall complication rate of 4.8% (Table 4). These comprised cardiac complications, including ventricular puncture, cardiac laceration and arrhythmias and damage to nearby organs, including the lung, liver and spleen.
Four of the complications occurred in patients who had undergone catheter laboratory procedures; 1 had undergone elective PCI, 1 had undergone an elective ablation for atrial fibrillation and 2 had PCI following myocardial infarctions. One of these patients had received thrombolysis. The remaining complications occurred in patients with pericardial effusions of varied etiology: post-infarction, amyloid, malignant and idiopathic.
 Eight of the 9 procedures that resulted in complications (88.9%) were carried out in an emergency setting for patients who had developed tamponade. Six of the 9 complications (66.6%) occurred in patients on oral anticoagulant or antiplatelet therapy. The details of each complication are shown in Table 5.
Eight of the 9 procedures that resulted in complications (88.9%) were carried out in an emergency setting for patients who had developed tamponade. Six of the 9 complications (66.6%) occurred in patients on oral anticoagulant or antiplatelet therapy. The details of each complication are shown in Table 5.
Six of the pericardiocenteses that resulted in complications were performed via the subcostal approach; all of the complications requiring subsequent surgical intervention were via the subcostal route.
Long-term outcomes. Of the 163 patients undergoing pericardiocentesis, 22 required further percutaneous drainage of their pericardial effusions (13.5%). Two patients required more than 2 pericardiocenteses. The median time between the initial procedure and subsequent drainage was 18 days (interquartile range: 4.3–85.5 days). Thirteen patients required definitive surgical management of their pericardial effusion; 7 had a pericardial window and 6 required pericardectomy. Median survival for patients with malignant pericardial effusions was 5.4 months. Comparative survival rates for patients with malignant and non-malignant pericardial effusions are shown in Figure 1B.
Consent. Formal written consent was obtained prior to pericardiocentesis in 86 cases (45.7%); a further 4 cases (2.1%) had documented verbal consent. If all emergency procedures were excluded, this rose to 54.3% (38/70) for written consent and 4.3% (3/70) for documented verbal consent.
Discussion
The etiology of pericardial effusions requiring drainage is changing. Traditionally, the most common causes of pericardial effusions were malignancy and uremia,2 with tuberculosis being prevalent in low- and middle-income countries and in hospitals serving multiracial populations.6–8 However, in high-income countries, the rise in the number of catheter-based cardiac procedures being performed has lead to a concomitant rise in the proportion of pericardial effusions that occur as a complication of these procedures.3,9 This change is best shown in the large historical pericardiocentesis series from the Mayo Clinic in the United States, published in 2002.3 This group looked at pericardiocenteses over 21 years and demonstrated a significant increase in the proportion of cases that were caused by cardiac surgery (from 21 to 28%) and cardiac perforation from catheter-based procedures (from 4 to 14%).
The present study confirms that cardiac interventions constitute a major cause of pericardial effusions requiring drainage in contemporary practice, with 35.0% of all patients having an iatrogenic cause for their effusion. The majority of these (27.6%) are due to catheter-based procedures. It is this population that is of particular interest, because it varies from the remainder of the study population in two important ways. First, patients undergoing catheter-based procedures are significantly more likely to present acutely with overt tamponade, with 91.5% presenting in this fashion (p < 0.0001). Second, they are significantly more likely to be receiving antiplatelet and anticoagulant agents, with 95.7% of patients requiring pericardiocentesis after a cardiac intervention having received at least one anticoagulant or antiplatelet agent on the day of the procedure (p < 0.0001). Indeed, 44.7% had received 3 or more such drugs.
Anticoagulation is cited as a relative contraindication to performing pericardiocentesis by the European Cardiology Society guidelines and may impact on the risk profile and complication rate of the procedure.5 Combined with our observation that complications of pericardiocentesis may be more common when the procedure is being carried out for tamponade, it is clear that this changing patient population may bring new challenges to cardiologists carrying out pericardiocenteses.
The most common cause of pericardial effusion in this study was malignancy. This is in keeping with other series3,10,11 and, as previously found, lung and breast were the most common primary sites identified. Malignant pericardial effusions are associated with a poor prognosis and our study demonstrates that this has improved little with contemporary oncological practice. The development of a pericardial effusion remains a grave occurrence in malignant disease, with a subsequent median survival in this study of only 5.4 months. This is similar to findings in other series.12–15
The complication rate in this study was 4.9%. This compares favorably with other series published since the introduction of ultrasound-guided pericardiocentesis.3,8,16–18 The largest series of pericardiocenteses quotes a major complication rate (defined as requiring intervention) of 1.2% with a minor complication rate (defined as not requiring intervention) of 3.5%.3 Other smaller studies report complication rates of up to 20%.8,16
For those pericardial effusions occurring after a catheter-based procedure, the majority (91.5%) presented with tamponade and 44% presented in the catheter laboratory. However, over half presented outside the laboratory with a median time to presentation of 5 hours. This confirms the findings observed in other studies17,19 that delayed cardiac tamponade can occur after a catheter-based procedure and clinicians should have a high index of suspicion for this complication in acutely unwell patients even several hours after their procedure.
Fewer than half of the pericardiocenteses performed in this series had evidence of written consent in the medical notes. There are no formal guidelines on consent prior to pericardiocentesis. However, the United Kingdom’s General Medical Council recommends that written consent be obtained from a patient “if the investigation or treatment is complex or involves significant risks.”20 Given the significant complication rate of pericardiocentesis documented here and in other series, it would seem prudent that written consent should be obtained where clinically feasible.
There are two main factors that dictate the approach route chosen to perform pericardiocentesis: operator preference and the effusion characteristics.5 The Mayo Clinic advocates selection of approach route based purely on echocardiographic findings; they define the optimal entry site as “the point at which the distance from the skin to maximum fluid accumulation is minimized, with no intervening vital organs.” Using this method to select the entry site, the majority of their pericardiocenteses are performed via the chest wall, with only 18% of procedures carried out via a subcostal approach. In contrast, a survey of United Kingdom practices published in 2008 showed that of the 274 cardiologists who responded, 89% prefer a subcostal approach route for pericardiocentesis.21
A survey of 24 cardiologists from the Oxford region (unpublished data) showed an even divide in the preferred route of approach. Twenty-five percent cited personal preference as the most important factor in determining their choice of approach. Practical considerations, including easier access via the subcostal route when performing pericardiocentesis during a catheter-based procedure, were also given to explain selection of route.
In the present study, all of the major complications requiring surgical intervention occurred via the subcostal approach. This is because liver and splenic damage can only occur via this route. Although the absolute number of complications by either route was low, these data suggest that an apical approach may be favorable if circumstances allow. This may be a particularly important consideration when performing pericardiocentesis in heavily anticoagulated patients.
This study has a number of limitations. It is retrospective, and consequently relies on contemporaneous, accurate note keeping. Although thorough search methodology was used in an attempt to identify pericardial effusions, it is possible that some pericardiocenteses occurring in the study period were missed. Several different operators performed the drains and the technique used was not standardized. Comparisons are post hoc and non-randomized.
Nonetheless, it is the largest European series to date and provides an up-to-date understanding of the characteristics of patients undergoing pericardiocentesis and the potential complications in real-life practice.
Conclusion
This series confirms that pericardial effusions occurring as a complication of catheter-based procedures are rising as a proportion of the total number of effusions requiring drainage. The vast majority of patients undergoing such procedures receive blood-thinning agents, which may increase the risk of complications during pericardiocentesis. It appears that complications requiring surgery may occur more frequently with pericardiocentesis performed via a subcostal route, but further studies are needed to confirm this trend. Given the small but significant risk of complications, where practical, more attention should be made to ensure that patients provide adequate consent prior to pericardiocentesis.
References
- Wong B, Murphy J, Chang CJ, et al. The risk of pericardiocentesis. Am J Cardiol 1979;44:1110–1114.
- Guberman BA, Fowler NO, Engel PJ, et al. Cardiac tamponade in medical patients. Circulation 1981;64:633–640.
- Tsang TS, Enriquez-Sarano M, Freeman WK, et al. Consecutive 1,127 therapeutic echocardiographically guided pericardiocenteses: Clinical profile, practice patterns, and outcomes spanning 21 years. Mayo Clin Proc 2002;77:429–436.
- Spodick DH. Acute cardiac tamponade. New Engl J Med 2003;349:684–690.
- Maisch B, Seferović PM, Ristić AD, et al. Guidelines on the diagnosis and management of pericardial diseases. Executive summary: The Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Eur Heart J 2004;25:587–610.
- Kil UH, Jung HO, Koh YS, et al. Prognosis of large, symptomatic pericardial effusion treated by echo-guided percutaneous pericardiocentesis. Clin Cardiol 2008;31:531–537.
- Jain S, Sharma N, Varma S. Profile of cardiac tamponade in the medical emergency ward of a North Indian Hospital. Can J Cardiol 1999;15:672–675.
- Gibbs CR, Watson RD, Singh SP, et al. Management of pericardial effusion by drainage: A survey of 10 years’ experience in a city centre general hospital serving a multiracial population. Postgrad Med J 2000;76:809–813.
- Atar S, Chiu J, Forrester JS, et al. Bloody pericardial effusion in patients with cardiac tamponade: Is the cause cancerous, tuberculous, or iatrogenic in the 1990s? Chest 1999;116:1564–1569.
- Cornily JC, Pennec PY, Castellant P, et al. Cardiac tamponade in medical patients: A 10-year follow-up survey. Cardiology 2008;111:197–120.
- Ben-Horin S, Bank I, Guietta V, et al. Large symptomatic pericardial effusion as the presentation of unrecognized cancer: A study in 173 consecutive patients undergoing pericardiocentesis. Medicine 2006;85:49–53.
- Yonemori K, Kunitoh H, Tsuta K, et al. Prognostic factors for malignant pericardial effusion treated by pericardial drainage in solid-malignancy patients. Med Oncol 2007;24:425–430.
- Tsang TS, Seward JB, Barnes ME, et al. Outcomes of primary and secondary treatment of pericardial effusion in patients with malignancy. Mayo Clin Proc 2000;75:248–253.
- Gross JL, Younes RN, Deheinzelin D, et al. Surgical management of symptomatic pericardial effusion in patients with solid malignancies. Ann Surg Oncol 2006;13:1732–1738.
- Dequanter D, Lothaire P, Berghmans T, Sculier JP. Severe pericardial effusion in patients with concurrent malignancy: A retrospective analysis of prognostic factors influencing survival. Ann Surg Oncol 2008;15:3268–3271.
- Vayre F, Lardoux H, Pezzano M, et al. Subxiphoid pericardiocentesis guided by contrast two-dimensional echocardiography in cardiac tamponade: Experience of 110 consecutive patients. Eur J Echocardiography 2000;1:66–71.
- Tsang TS, Freeman WK, Barnes ME, et al. Rescue echocardiographically guided pericardiocentesis for cardiac perforation complicating catheter-based procedures. The Mayo Clinic experience. J Am Coll Cardiol 1998;32:1345–1350.
- Tsang TS, Barnes ME, Gersh BJ, et al. Outcomes of clinically significant idiopathic pericardial effusion requiring intervention. Am J Cardiol 2002;91:704–707.
- Fejka M, Dixon SR, Safian RD, et al. Diagnosis, management, and clinical outcome of cardiac tamponade complicating percutaneous coronary intervention. Am J Cardiol 2002;90:1183–1186.
- Consent: Patients and doctors making decisions together. General Medical Council. Published 2008.
- Balmain S, Hawkins NM, MacDonald MR, et al. Pericardiocentesis practice in the United Kingdom. Int J Clin Pract 2008;62:1515–1519.
_________________________________________
*Joint first authors.
From 1the Cardiology Department, Royal Berkshire Hospital, Reading, 2the Cardiology Department, Milton Keynes General Hospital, Milton Keynes, Buckinghamshire, 3the Cardiology Department, Wycombe Hospital, High Wycombe, 4Oxford Heart Centre, John Radcliffe Hospital, Headington, Oxford, United Kingdom.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted January 2, 2011, provisional acceptance given March 27, 2011, final version accepted April 14, 2011.
Address for correspondence: Dr. David Adlam, BA BM BCh DPhil MRCP, Department of Cardiology, Oxford Heart Centre, John Radcliffe Hospital, Headley Way, Oxford, 9DU 8FT, United Kingdom. Email: dadlam@well.ox.ac.uk


