

Potential Contribution of Open-Cell Stent Design to Balloon Entrapment and Review of Techniques to Recover
ABSTRACT: Balloon entrapment during coronary angioplasty is a rare but potentially disastrous complication of percutaneous coronary intervention (PCI), described during both angioplasty alone, as well as with stents. This report describes the case of an entrapped stent-balloon within an extremely calcified proximal left anterior descending artery (LAD) lesion, and reviews techniques and strategies that can be applied in similar situations. In this case, we suspect the open-cell design of the specific stent used, combined with the high radial force of the calcified lesion, led to a “pincer effect,” and entanglement of the balloon material within the stent scaffolding. After exhaustion of all percutaneous options to retrieve the balloon, the patient was ultimately taken for urgent cardiac surgery for extraction of the balloon and vein patch of the LAD.
J INVASIVE CARDIOL 2011;23:E183–E187
________________________________________
Cook Video_edited.mp4 Balloon entrapment in a target lesion during coronary angioplasty is a rare but potentially disastrous complication of percutaneous coronary intervention (PCI). It has been described during both angioplasty alone1–3 as well as with balloons within stents.4–6 This report describes the case of an entrapped stent-balloon within an extremely calcified proximal left anterior descending artery (LAD) lesion, and reviews techniques and strategies that can be applied in similar situations. In this case, we suspect that the open-cell design of the specific stent used, combined with the high radial force of the calcified lesion, led to a “pincer effect” and entanglement of the balloon material within the stent scaffolding.
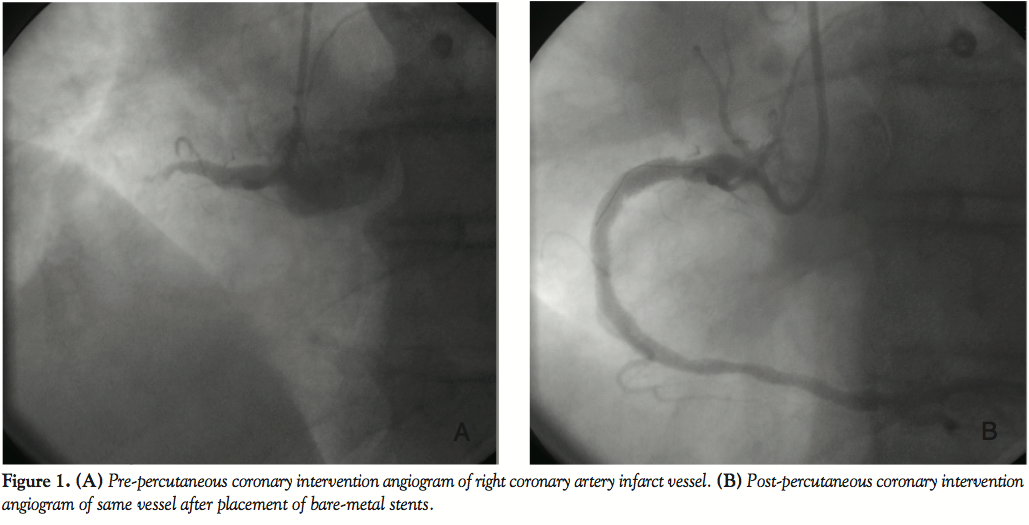 Case Report. A 75-year-old man with a history of hypertension presented to the emergency department on day 1 with inferior wall ST-elevation myocardial infarction (STEMI). He denied any prior cardiac history. He was taken directly to the cardiac catheterization lab for primary PCI. Angiogram revealed acute thrombosis within the right coronary artery (RCA), with 100% occlusion. PCI was performed within the infarct vessel, with placement of two bare-metal stents and reduction of the lesion to 0% residual stenosis and TIMI 3 flow in the distal vessel (Figures 1A and 1B).
Case Report. A 75-year-old man with a history of hypertension presented to the emergency department on day 1 with inferior wall ST-elevation myocardial infarction (STEMI). He denied any prior cardiac history. He was taken directly to the cardiac catheterization lab for primary PCI. Angiogram revealed acute thrombosis within the right coronary artery (RCA), with 100% occlusion. PCI was performed within the infarct vessel, with placement of two bare-metal stents and reduction of the lesion to 0% residual stenosis and TIMI 3 flow in the distal vessel (Figures 1A and 1B).
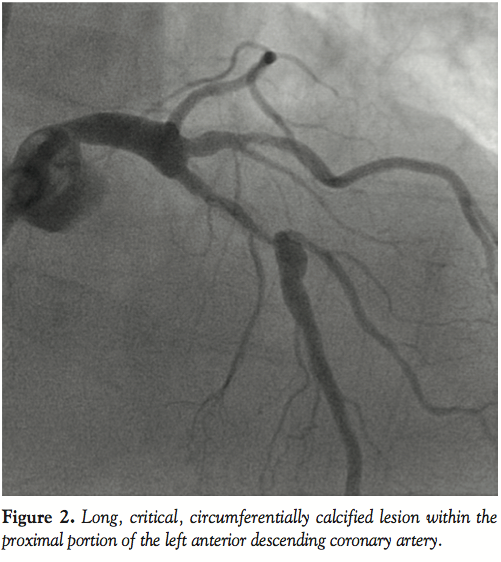 In addition to the RCA occlusion, there was also a long, critical, circumferentially calcified lesion within the proximal portion of the LAD (Figure 2). Staged revascularization of the LAD was subsequently recommended due to the large area of at-risk myocardium. Multiple options were considered, including PCI with stenting, rotational atherectomy (rotablation), single-vessel coronary artery bypass (CABG), and medical therapy alone — each modality with unique risks and benefits. After thorough discussion with the patient and family about these issues, PCI with stenting was ultimately chosen as the most appropriate treatment option.
In addition to the RCA occlusion, there was also a long, critical, circumferentially calcified lesion within the proximal portion of the LAD (Figure 2). Staged revascularization of the LAD was subsequently recommended due to the large area of at-risk myocardium. Multiple options were considered, including PCI with stenting, rotational atherectomy (rotablation), single-vessel coronary artery bypass (CABG), and medical therapy alone — each modality with unique risks and benefits. After thorough discussion with the patient and family about these issues, PCI with stenting was ultimately chosen as the most appropriate treatment option.
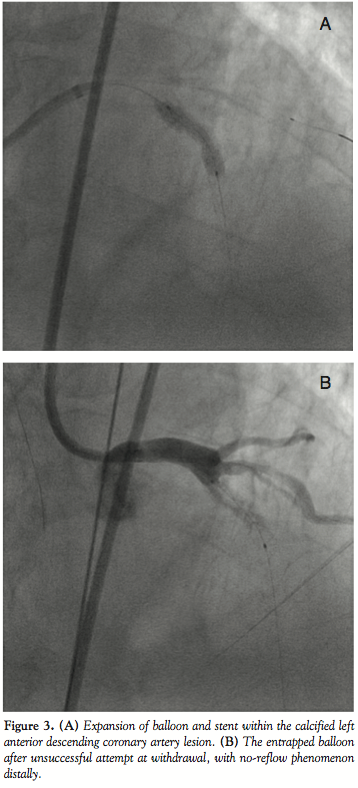 On day 3, the patient was brought back to the cath lab for staged PCI. An 8 French (Fr) Amplatz™ Left (AL) 2.0 guide (Boston Scientific, Natick, Massachusetts) was selected for increased support, and a Whisper™ wire (Abbott Vascular, Abbott Park, Illinois) was advanced easily through the lesion. Due to the lesion proximity to a large ramus intermedius bifurcation, a BMW™ wire (Abbott Vascular) was placed in the ramus for protection from potential plaque shift. A 3.0 x 20 mm Voyager™ NC noncompliant balloon (Abbott Vascular) was used for predilation, inflated at 14 atm for 30 seconds, to apparent full expansion. A Cypher sirolimus-eluting stent (on Bx Velocity™ platform [Cordis Corporation, Miami Lakes, Florida) was requested, but was not stocked in the 3.5 x 23 mm size that was required. Thus, a 4.0 x 24 mm Taxus paclitaxel-eluting stent (on Liberte™ platform [Boston Scientfic]) was chosen, deployed at 16 atm for 30 seconds. Postdeployment cineangiography appeared to demonstrate full expansion of the stent within the target stenosis (Figure 3A). However, when attempts were then made to withdraw the balloon into the guide, it would not disengage from the stent scaffolding.
On day 3, the patient was brought back to the cath lab for staged PCI. An 8 French (Fr) Amplatz™ Left (AL) 2.0 guide (Boston Scientific, Natick, Massachusetts) was selected for increased support, and a Whisper™ wire (Abbott Vascular, Abbott Park, Illinois) was advanced easily through the lesion. Due to the lesion proximity to a large ramus intermedius bifurcation, a BMW™ wire (Abbott Vascular) was placed in the ramus for protection from potential plaque shift. A 3.0 x 20 mm Voyager™ NC noncompliant balloon (Abbott Vascular) was used for predilation, inflated at 14 atm for 30 seconds, to apparent full expansion. A Cypher sirolimus-eluting stent (on Bx Velocity™ platform [Cordis Corporation, Miami Lakes, Florida) was requested, but was not stocked in the 3.5 x 23 mm size that was required. Thus, a 4.0 x 24 mm Taxus paclitaxel-eluting stent (on Liberte™ platform [Boston Scientfic]) was chosen, deployed at 16 atm for 30 seconds. Postdeployment cineangiography appeared to demonstrate full expansion of the stent within the target stenosis (Figure 3A). However, when attempts were then made to withdraw the balloon into the guide, it would not disengage from the stent scaffolding.
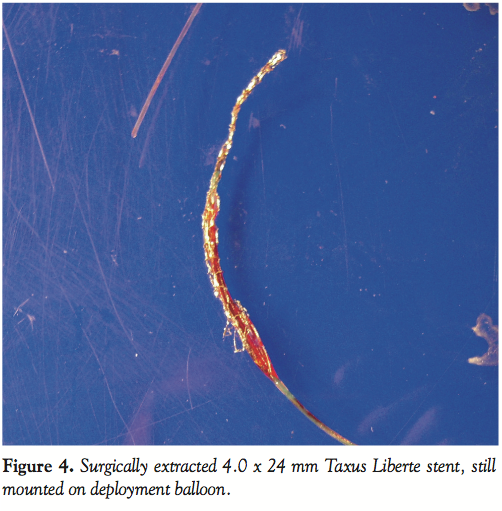 Subsequent views with the balloon in place revealed no-reflow distal to the stent (Figure 3B). A number of techniques were applied in attempts to free the balloon (see discussion below), but were proven unsuccessful. Ultimately, after all other percutaneous options to disengage the balloon were exhausted, the surgical backup team was alerted, and the patient was accepted for an emergent CABG. The patient was transferred directly to the surgical suite, where he underwent LAD bypass. Coronary arteriotomy at the level of the balloon and stent was performed, the balloon catheter and stent were removed, and a vein patch was applied. The stent and balloon were quite deformed (Figure 4). The postoperative course was uneventful, and the patient was discharged on postop day 13.
Subsequent views with the balloon in place revealed no-reflow distal to the stent (Figure 3B). A number of techniques were applied in attempts to free the balloon (see discussion below), but were proven unsuccessful. Ultimately, after all other percutaneous options to disengage the balloon were exhausted, the surgical backup team was alerted, and the patient was accepted for an emergent CABG. The patient was transferred directly to the surgical suite, where he underwent LAD bypass. Coronary arteriotomy at the level of the balloon and stent was performed, the balloon catheter and stent were removed, and a vein patch was applied. The stent and balloon were quite deformed (Figure 4). The postoperative course was uneventful, and the patient was discharged on postop day 13.
 Discussion. A number of maneuvers can be used to free an entrapped post-inflation stent-balloon. First, the balloon can be gently pushed forward within the stent, as well as gently rotated, to free entrapped material and rewrap the balloon, before again withdrawing.7,8 Care must be taken to not damage the shaft of the balloon itself during rotation, as it can fracture. Second, the balloon can be reinflated to low pressures and deflated in succession, then withdrawn. If these initial steps do not work, consideration should be given to alerting the surgical backup and preparing an OR suite. An attempt can now be made to advance a second wire distal to the trapped balloon to straighten the vessel and provide a second rail for withdrawal. A standard medium body wire is a reasonable choice for this purpose, though softer and/or hydrophilic wires can be used to facilitate passage. If the stent-balloon still does not disengage, a second low-profile balloon, 1.5–2.0 mm in diameter, such as a Medtronic Sprinter™ (0.021˝ crossing profile, semicompliant)9 or Boston Scientific Maverick™ (0.017˝ crossing profile, noncompliant)10 can be advanced on the second wire and inflated alongside the trapped balloon to free it. Another possible technique is to place a smaller sized catheter over the shaft of the balloon, such as a glide catheter (which will require cutting the end of the shaft), and advancing it over the trapped balloon so as to ensheath it. All of these techniques were tried in our particular case, without success. A final tactic is to use a microsnare in this situation, which is well-described.4,11
Discussion. A number of maneuvers can be used to free an entrapped post-inflation stent-balloon. First, the balloon can be gently pushed forward within the stent, as well as gently rotated, to free entrapped material and rewrap the balloon, before again withdrawing.7,8 Care must be taken to not damage the shaft of the balloon itself during rotation, as it can fracture. Second, the balloon can be reinflated to low pressures and deflated in succession, then withdrawn. If these initial steps do not work, consideration should be given to alerting the surgical backup and preparing an OR suite. An attempt can now be made to advance a second wire distal to the trapped balloon to straighten the vessel and provide a second rail for withdrawal. A standard medium body wire is a reasonable choice for this purpose, though softer and/or hydrophilic wires can be used to facilitate passage. If the stent-balloon still does not disengage, a second low-profile balloon, 1.5–2.0 mm in diameter, such as a Medtronic Sprinter™ (0.021˝ crossing profile, semicompliant)9 or Boston Scientific Maverick™ (0.017˝ crossing profile, noncompliant)10 can be advanced on the second wire and inflated alongside the trapped balloon to free it. Another possible technique is to place a smaller sized catheter over the shaft of the balloon, such as a glide catheter (which will require cutting the end of the shaft), and advancing it over the trapped balloon so as to ensheath it. All of these techniques were tried in our particular case, without success. A final tactic is to use a microsnare in this situation, which is well-described.4,11
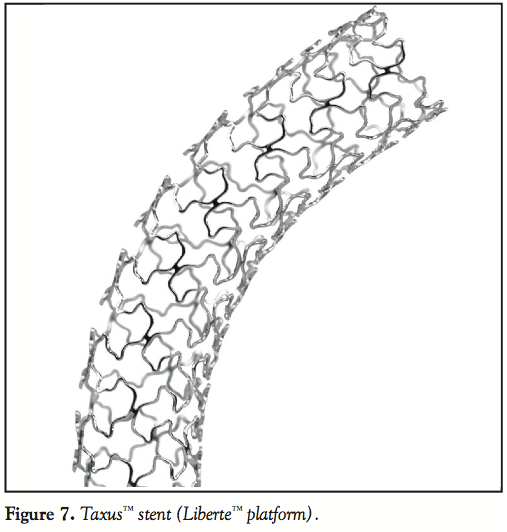
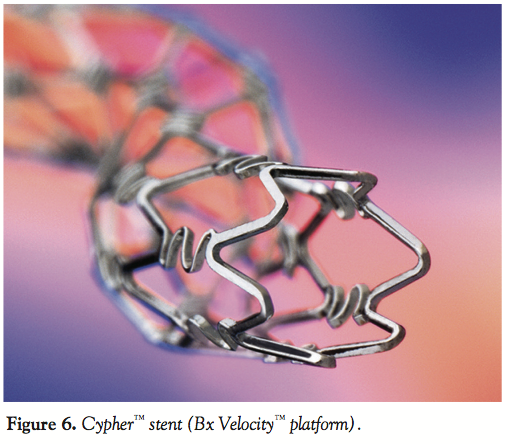 Early stents, such as the Cook Gianturco-Roubin™ and the Medtronic Wiktor™, were very flexible, but lack of longitudinal struts lead to poor radial strength.12 This led to development of today’s tubular stents, with longitudinal struts adjoined in different lengths and geometric patterns, adding significant radial strength while sacrificing flexibility. A related element is “open” versus “closed-cell” design, with the latter having longitudinal connections along the entirety of the stent, and the former employing areas without longitudinal struts. Open-cell stents tend to be more flexible and deliverable, and significantly change cell conformation with expansion.13 Closed-cell designs boast higher radial strength, maximum drug delivery, and better intimal coverage. Stents currently available have different ratios of each (Figures 5A and 5B). Contemporary drug-eluting stents include Taxus (which uses the Express and Liberte stent platforms), Cypher (Bx Velocity stent platform), Xience V™ (Vision™ stent platform; Abbott Vascular), and Endeavor™ (Driver™ stent platform; Medtronic, Minneapolis, Minnesota).14 Of these designs, the Bx Velocity platform has the most complete closed-cell design (Figure 6), compared with the Liberte platform (Figure 7).4,5
Early stents, such as the Cook Gianturco-Roubin™ and the Medtronic Wiktor™, were very flexible, but lack of longitudinal struts lead to poor radial strength.12 This led to development of today’s tubular stents, with longitudinal struts adjoined in different lengths and geometric patterns, adding significant radial strength while sacrificing flexibility. A related element is “open” versus “closed-cell” design, with the latter having longitudinal connections along the entirety of the stent, and the former employing areas without longitudinal struts. Open-cell stents tend to be more flexible and deliverable, and significantly change cell conformation with expansion.13 Closed-cell designs boast higher radial strength, maximum drug delivery, and better intimal coverage. Stents currently available have different ratios of each (Figures 5A and 5B). Contemporary drug-eluting stents include Taxus (which uses the Express and Liberte stent platforms), Cypher (Bx Velocity stent platform), Xience V™ (Vision™ stent platform; Abbott Vascular), and Endeavor™ (Driver™ stent platform; Medtronic, Minneapolis, Minnesota).14 Of these designs, the Bx Velocity platform has the most complete closed-cell design (Figure 6), compared with the Liberte platform (Figure 7).4,5
 When planning PCI within highly calcified lesions, or in arteries with other factors that may increase radial recoil (elderly patient, high plaque burden, inability to fully predilate, etc.), we believe an important consideration is to preferentially use closed-cell stents. Open cells create small pockets into which the angioplasty balloon can prolapse, and if high radial forces act on the outside of stent, these areas can collapse, having a “pincer” effect on the balloon material. This may be worsened in lesions with acute curves, which can cause adjacent struts to project outward, or so-called “alligator backing,” increasing the risk for capturing the balloon at the underbelly of the curve. It is of note that the Taxus stent had early design issues resulting in suboptimal air passage from the balloon back into the catheter, leading to reports of nondeflation and sticking, prompting product recalls in 2004.15 A possible contributing factor is the adhesive characteristics of the polymer used in the Taxus stent.16 To be clear, nondeflation did not occur in our patient.
When planning PCI within highly calcified lesions, or in arteries with other factors that may increase radial recoil (elderly patient, high plaque burden, inability to fully predilate, etc.), we believe an important consideration is to preferentially use closed-cell stents. Open cells create small pockets into which the angioplasty balloon can prolapse, and if high radial forces act on the outside of stent, these areas can collapse, having a “pincer” effect on the balloon material. This may be worsened in lesions with acute curves, which can cause adjacent struts to project outward, or so-called “alligator backing,” increasing the risk for capturing the balloon at the underbelly of the curve. It is of note that the Taxus stent had early design issues resulting in suboptimal air passage from the balloon back into the catheter, leading to reports of nondeflation and sticking, prompting product recalls in 2004.15 A possible contributing factor is the adhesive characteristics of the polymer used in the Taxus stent.16 To be clear, nondeflation did not occur in our patient.
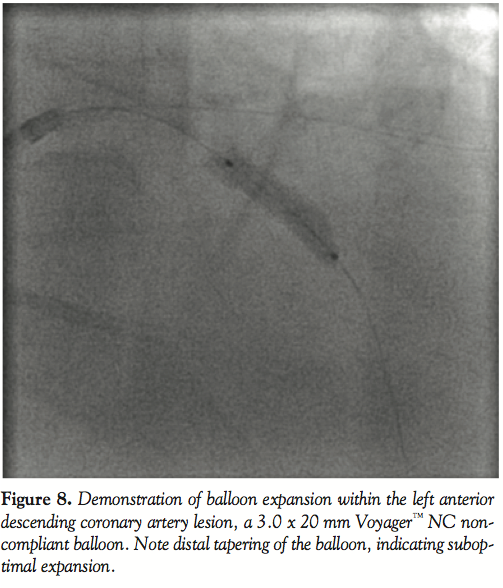 Of course, the extensive calcification in this particular case placed the patient at higher risk for complications overall; in fact, calcification of a lesion has been shown to be one of the most significant predictors of procedural failure in PCI.17 Retrospectively, perhaps more consideration could have been given to planned CABG, or the use of adjunctive techniques such as rotational atherectomy. Though the latter has fallen out of favor in recent years as a stand-alone technique, many reports have shown high procedural success when used for debulking of plaque prior to stenting (the so called Rota-stent technique) in heavily calcified lesions, achieving an impressive 89–98% procedural success.18 It also may be of particular utility for lesions in which the PCI balloon does not fully expand.19On careful review of the predilation image, this occurred to some extent at the distal tip of our balloon (Figure 8).
Of course, the extensive calcification in this particular case placed the patient at higher risk for complications overall; in fact, calcification of a lesion has been shown to be one of the most significant predictors of procedural failure in PCI.17 Retrospectively, perhaps more consideration could have been given to planned CABG, or the use of adjunctive techniques such as rotational atherectomy. Though the latter has fallen out of favor in recent years as a stand-alone technique, many reports have shown high procedural success when used for debulking of plaque prior to stenting (the so called Rota-stent technique) in heavily calcified lesions, achieving an impressive 89–98% procedural success.18 It also may be of particular utility for lesions in which the PCI balloon does not fully expand.19On careful review of the predilation image, this occurred to some extent at the distal tip of our balloon (Figure 8).
In conclusion, stent-balloon entrapment is a rare but potentially disastrous complication of PCI. A number of measures may have prevented the risk of this complication in our case; namely, a closed-cell stent system, such as the Bx Velocity platform, may have been less likely to entrap the balloon. Further, preparation of calcified lesions with rotational atherectomy remains a well-recognized indication for this device, and may have been helpful to facilitate stent delivery. Once the complication occurred, however, surgical backup played an important role in this patient’s survival. In the current PCI era, crossover to coronary artery bypass remains an important safety net in PCI for any number of complications. Though emergent bypass after a failed PCI has trended downward in numbers, from 3% in the pre-stent era to < 1% in the current era, the risk increases with the complexity of the specific coronary lesion being treated.20,21 Nearly all reports of trapped angioplasty balloon have required surgical rescue.
References
- Shyam JS, Thingnam KS, Das D. Surgical removal of entrapped and broken percutaneous transluminal coronary angioplasty balloon catheter. Interact CardioVasc Thorac Surg 2007;6:94–96
- Rosario PG, Donahoo JS. Coronary artery endarterectomy for retrieval of entrapped percutaneous cather. Ann Thorac Surg 1996;61:218–219.
- Columbo A, Skinner JM. Balloon entrapment in a coronary artery: Potential serious complications of balloon rupture. Cathet Cardiovasc Diagn 1990;19:23–25.
- Madronero JL, Hein F, Bergbauer M. Removal of a ruptured, detached, and entrapped angioplasty balloon after coronary stenting. J Invasive Cardiol 2000;12:102–104.
- Panda BR, ThomsonVS, Shankar R, et al. Stuck coronary angioplasty balloon: A surgical emergency. Ind J Thorac Cardiovasc Surg 2009;25:124–126.
- Matt P, Zerkowski HR, Pfisterer M, et al. Troubleshooting for a stuck balloon catheter. Ann Thorac Surg 2007;83:320.
- Nguyen TN, Ischinger T, Nhan VT, Kumar R. Balloon angioplasty. In: Practical Handbook of Advanced Interventional Cardiology, 3rd edition. Blackwell Publishing, Malden, Massachusetts: 2008. pp. 84–95.
- Rizzo TF, Werres R, Ciccone J, et al. Entrapment of an angioplasty balloon catheter: A case report. Cathet Cardiovasc Diagn 1988;14:255–257.
- Rhoads CS, Fort S. Indications, safety and warning information webpage for Sprinter Legend RX Semicompliant Balloon Dilatation Catheter. Available at https://www.medtronic.com/for-healthcare-professionals/products-therapies/cardiovascular/catheters/balloon-dilatation-catheters/sprinter-legend-rx-semicompliant-balloon-dilatation-catheter/index.htm.
- https://www.bostonscientific.com.
- Watson LE. Snare loop technique for removal of broken steerable PTCA wire. Cathet Cardiovasc Diagn 1987;13:44–49.
- Perrins EJ. Intracoronary stenting. In: Essential Interventional Cardiology, 2nd edition. Norell MS, Perrins EJ (eds). W.B. Saunders, Philadelphia, Pennsylvania: 2008.
- Hara H, Nakamura M, Palmaz JC, Schwartz RS. Role of stent design and coatings on restenosis and thrombosis. Adv Drug Deliv Rev 2006;58:377–386.
- Popma JJ, Baim DS, Resnic FS. Percutaneous coronary and valvular intervention. In: Braunwald’s Heart Disease, 8th edition. W.B. Saunders, Philadelphia, Pennsylvania: 2008.
- Baim DS, Mehran R, Kereiakes DJ, et al. Postmarket surveillance for drug-eluting coronary stents: A comprehensive approach. Circulation 2006;113:891–897.
- Turk M, Gupta V, Fischel TA. Evaluation of balloon withdrawal forces with bare-metal stents, compared with Taxus and Cypher drug-eluting stents: Balloon, stent, and polymer interactions. J Invasive Cardiol 2010;22:117–118.
- Tan K, Sulke N, Taub N, Sowton E. Clinical and lesion morphologic determinants of coronary angioplasty success and complications: Current experience. J Am Coll Cardiol 1995;25:855–865.
- Tran T, Brown M, Lasala J. An evidene-based approach to the use of rotational and directional coronary atherectomy in the era of drug-eluting stents: When does it make sense? Catheter Cardiovasc Interv 2008;72:650–662.
- Silber S, Albertsson P, Aviles FF, et al. Guidelines for percutaneous coronary interventions. Eur Heart J 2005;26:804–847.
- Yang EH, Gumina RJ, Lennon RJ, et al. Emergency coronary artery bypass surgery for percutaneous coronary interventions: Changes in the incidence, clinical characteristics, and indications from 1979–2003. J Am Coll Cardiol 2005;46:2004–2009.
- Seshadri N, Whitlow PL, Acharya N, et al. Emergency coronary artery bypass surgery in the contemporary percutaneous intervention era. Circulation 2002;106:2346–2350.
________________________________________
From the 1Department of Cardiology and 2Department of Cardiothoracic Surgery, Illinois Masonic Medical Center, Chicago, Illinois.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 26, 2010, provisional acceptance given November 29, 2010, final version accepted January 24, 2011.
Address for correspondence: Jeffrey R. Cook, MD, Department of Cardiology, Illinois Masonic Medical Center, 836 W. Wellington, Chicago, IL 60657. Email: jrcook79@yahoo.com











