

The Prediction of Coronary Artery Disease Based on Non-Invasive Examinations and Heme Oxygenase 1 Polymorphism Versus Virtual Histology
Download a PDF of this article.
Abstract: Objective. Prediction of coronary atherosclerosis in patients with stable angina based on non-invasive examinations. Methods. Pro-inflammatory markers, heme oxygenase-1 (HO-1) polymorphism, lipid levels, Framingham risk score (FRS), and carotid ultrasound were analyzed and compared to grayscale and virtual histology intravascular ultrasound (VH-IVUS). Results. A total of 101 patients were included, and genetic analysis was performed on 81 patients (80.2%). The HO-1 risk polymorphism was more frequent in patients post-myocardial infarction (61.3% vs 32%; P=.0097), or with diabetes (68.4% vs 35.5%; P=.011) or a higher FRS (21.5 vs 15.7; P=.014). Plaques in patients with the HO-1 risk polymorphism contained less fibro-fatty tissue (17.1% vs 23.2%; P=.005) and more necrotic core (NC; 17.1% vs 12.7%; P=.02) and calcification (10.2% vs 5.7%; P=.035) compared to patients without the HO-1 risk polymorphism. Carotid intima media thickness (P=.05) and carotid bulb plaque (P=.008) predicted plaque burden. The level of Apo A inversely correlated with NC (P=.047; r = -0.27) and was lower in patients with VH-thin-cap fibroatheroma (VH-TCFA; 1.19 mmol/L vs 1.3 mmol/L; P=.04). FRS correlated with NC (P=.007; r = 0.2), with angiographic disease severity (P=.032; r = 0.21) and was higher in patients with VH-TCFA (9.1 vs 7.8; P=.03). Conclusion. Carotid ultrasound and HO-1 polymorphism improve coronary atherosclerosis prediction.
J INVASIVE CARDIOL 2013;25(1):32-37
Key words: inflammation, plaque composition
_______________________________________________
Acute coronary syndrome (ACS) is the first manifestation of coronary artery disease (CAD) in more than 50% of patients. Traditional risk stratification is limited. Many myocardial infarctions (MIs) occur in patients in the intermediate-risk group. Risk stratification can be improved by assessment of non-coronary atherosclerosis like carotid intima media thickness (IMT)1 and markers of inflammation and oxidative stress.2
We recently published a study3 of 107 patients, 70 of whom were genetically studied, that focused on the relationship between a genetic polymorphism for endothelial nitric oxide synthase and heme oxygenase-1 (HO-1) versus atherosclerosis development. The most interesting finding of this study was the correlation between the HO-1 polymorphisms and the extent of coronary atherosclerosis. The aim of the present study is to extend our initial results to examine how the analysis of genetic polymorphisms for HO-1 can improve prediction of the extent and risk profile of atherosclerosis based on traditional risk factors, pro-inflammatory markers, and carotid ultrasound.
HO is a microsomal enzyme that catalyzes heme degradation to iron, carbon monoxide (CO), and biliverdin, which is subsequently converted to bilirubin. CO and bilirubin are substances with vasodilatory, antioxidative, angiogenic, and anti-inflammatory properties. Iron is a potentially pro-oxidant agent, but is sequestrated by ferritin.4 The enzyme HO exists as isoenzymes HO-1 (inducible), HO-2 (constitutive), and HO-3 (probably only a pseudotranscript of HO-2).5,6 The activity of the HO-1 gene is determined by the number of guanosine-thymidine (GT) dinucleotide repeats in the gene promoter. As the number of GT dinucleotide repeats increases, transcription of the gene, and thus its enzymatic activity, decreases.6 Increased risk for CAD development was found in patients with an HO-1 gene polymorphism demonstrating a higher GT repetition.7 Conversely, gene variants with a reduced number of GT repeats react to oxidative stress with increased transcriptional activity and thus act to protect against the development of atherosclerosis.8
The present study examined non-invasive predictors of the following coronary angiographic (CAG), intravascular ultrasound (IVUS), and virtual histology (VH-IVUS) parameters:
(1) Angio score (angio) from CAG — a parameter of total atherosclerotic burden of coronary arteries.
(2) Percent atheroma volume (PAV) from IVUS — relative volume of selected non-culprit plaque.
(3) Necrotic core (NC) from VH-IVUS — amount of necrotic core in selected non-culprit plaques.
(4) Thin cap fibroatheroma (TCFA) from VH-IVUS — rupture-prone high-risk type of plaque9 and a predictor of future cardiac events.10
Methods
Study patients. Because the objective of our study was to identify features of unstable plaques before the onset of ACS, only patients with stable angina pectoris (SAP) were included. All patients signed informed consent, and the study was approved by the local ethical committee.
Framingham risk score (FRS). This risk score predicts a 10-year risk of coronary events according to a gender-specific model using age, diabetes mellitus (DM), total cholesterol or low density lipoprotein cholesterol (LDLc was used in this study), systolic and diastolic blood pressure, and smoking. Risk score was calculated using β-coefficients to compute the linear function as described by Wilson et al.11
Ultrasonographic examination of the carotid arteries. Carotid IMT measurement was performed using B-mode ultrasound with an 8 MHz linear probe on the outlying wall of the common carotid artery (ACC) and the internal carotid artery (ACI — on both sides) in longitudinal sections during end-diastole. For purposes of CAD prediction, we used IMTmass (sum of IMT in ACC and ACI for both sides) and IMTmax (maximum of all IMT measurements in every patient). Experienced ultrasonographers adjudicated carotid plaque presence in the carotid bulb if two of the following three criteria were met: (1) abnormal wall thickness (defined as IMT >1.5 mm); (2) abnormal shape (protrusion into the lumen, loss of alignment with adjacent arterial wall boundary); and (3) abnormal wall texture (brighter echoes than adjacent boundaries).12
Pro-inflammatory cytokines. We analyzed the following pro-inflammatory markers: vascular cellular adhesive molecule (VCAM), intercellular adhesive molecule (ICAM), tumor necrosis factor alpha (TNF alpha), CD 40 ligand, high-sensitivity C reactive protein (hsCRP), and interleukin 6 (IL-6). All markers were analyzed using the Enzyme Amplified Sensitivity Immunoassay (ELISA).
HO-1 polymorphism. Genomic DNA was isolated from peripheral blood leukocytes using standard procedures. The region of the HO-1 gene promoter containing a poly(GT)n repeat was amplified by polymerase chain reaction (PCR). We have divided alleles according to the number of GT repeats into two subclasses: promoters with less than 25 (GT)n – class S (short) alleles and promoters with 25 or more (GT)n – class L (long) alleles. Homozygous class S and heterozygous class S were grouped together (referred as protective type HO-1 polymorphism) and compared to the homozygous class L carriers (referred as high-risk type of HO-1 polymorphism in the Results and Discussion sections). This group classification was used because both homozygous and heterozygous carriers of the class S allele show a reduced inflammatory response and thus are protective.8 All patients signed informed content for genetic analysis.
Catheterization and grayscaler and VH-IVUS. The following angiographic score was used to assess the atherosclerotic burden in the coronary arteries. We calculated the sum of the numeric indices (1, 2, or 3 points as stated below) associated with all lesions exhibiting more than 20% diameter stenosis:
(1) 3 points: stenosis >50% in proximal third of a coronary artery.
(2) 2 points: stenosis <50% in proximal third of a coronary artery or stenosis >50% in the mid or distal third of a coronary artery.
(3) 1 point: stenosis <50% in the mid or distal third of a coronary artery.
After performing coronary angiography, the operator selected a target vessel for IVUS imaging. Only 1 native coronary artery with stenosis 20%-50% by angiography with no indication for either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) was investigated in each patient. Plaque length >20 mm was suitable for study. Plaque length was defined as the length of a continuous arterial segment with plaque burden >20% based on IVUS assessment.
In case of similar findings in more than 1 coronary artery, the artery with the largest plaque burden was selected for the analysis.
The IVUS phased-array probe (Eagle Eye, 20 MHz, 2.9 Fr monorail), IVUS console, software, and motorized pullback device (research pullback, model R-l00) were used for the studies (Volcano Corporation). After administration of 200 µg of intracoronary nitroglycerin, the IVUS probe was introduced into the selected coronary artery at least 10 mm distal to the plaque. Motorized pullback at 0.5 mm/s was performed through the rest of the coronary artery all the way to the ostium. Plaque volume was expressed as a percent atheroma volume (PAV), which was calculated as Σ (EEMCSA – Lumen CSA) divided by Σ (EEMCSA) x 100, where EEMCSA was the external elastic membrane cross-sectional area and Lumen CSA was the luminal cross-sectional area in the IVUS frames of the pullback sequence. Frames for IVUS analysis were taken from VH-IVUS mode, and all frames were analyzed.
Technical details of VH-IVUS as well as the analysis recommendations have been well-published.13 VH-IVUS uses spectral analysis of IVUS radiofrequency data to classify plaques into four components: fibrotic tissue (F), fibrous-fatty tissue (FF), calcification (DC), and necrotic core (NC).14 VH-IVUS analyses are reported in relative amounts (percentages of plaque). The definition of VH-derived TCFA (VH-TCFA13) was as follows: NC comprising more than 10% of the plaque in at least three consecutive cross-sections and direct contact of the NC with the vessel lumen.
Statistical analysis. Mean values ± standard deviation or percentages were calculated for all variables. Differences between the groups were compared by the χ2 test. Statistical significance was calculated by Fischer’s exact test for alternative variables. The statistical significance for continuous variables was determined by the Student’s t-test. Data were analyzed using JMP 3.2 statistical software (SAS Institute). A P-value of <.05 was considered statistically significant. Multivariate statistical analysis was performed using IBM SPSS software version 17.0. Linear regression analysis was used for three dependent variables: angio, PAV, and NC. Logistic regression was used for the dependent variable VH-TCFA. Optimal groups of predictors were chosen for achieving the best prediction of dependent variables.
Results
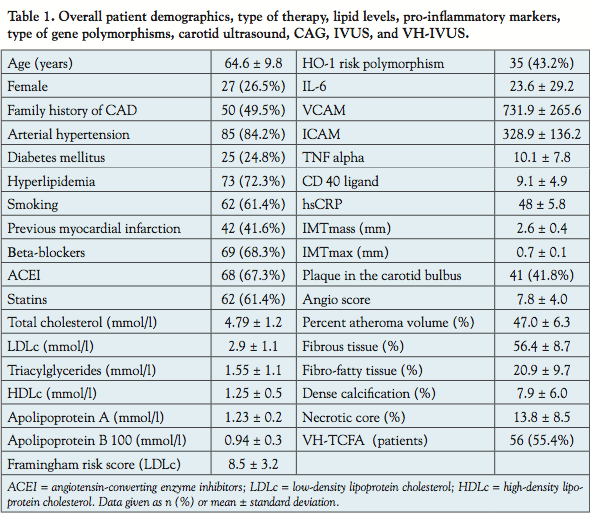 Patient population. Between November 2005 and April 2009, a total of 107 patients with SAP were included in the study. Data from 6 patients were unsuitable for VH-IVUS. Genetic analysis was performed in 81 patients (80.2%). Patient demographics are summarized in Table 1. The following arteries were analyzed: left anterior descending artery in 64 patients (63.4%), right coronary artery in 32 patients (31.7%), and left circumflex artery in 4 patients (4%).
Patient population. Between November 2005 and April 2009, a total of 107 patients with SAP were included in the study. Data from 6 patients were unsuitable for VH-IVUS. Genetic analysis was performed in 81 patients (80.2%). Patient demographics are summarized in Table 1. The following arteries were analyzed: left anterior descending artery in 64 patients (63.4%), right coronary artery in 32 patients (31.7%), and left circumflex artery in 4 patients (4%).
 Angio score. The highest angio scores were found in patients with the following: history of myocardial infarction (MI) (9.5 ± 3.9 vs 6.5 ± 3.6; P=.0001), risk type of HO-1 polymorphism (9.1 ± 4.2 vs 6.9 ± 3.1; P=.008), patients with LDLc <2.6 mmol/L on therapy (8.8 ± 3.8 vs 6.9 ± 4.0; P=.018), statin therapy (8.8 ± 3.8 vs 6.9 ± 4.0; P=.018), and past history of hyperlipidemia (8.3 ± 4.2 vs 6.4 ± 3.0; P=.03). The FRS significantly correlated with the angio score (P=.032; r = 0.21). Predictors of the angio score from multivariate analysis are summarized in Table 2.
Angio score. The highest angio scores were found in patients with the following: history of myocardial infarction (MI) (9.5 ± 3.9 vs 6.5 ± 3.6; P=.0001), risk type of HO-1 polymorphism (9.1 ± 4.2 vs 6.9 ± 3.1; P=.008), patients with LDLc <2.6 mmol/L on therapy (8.8 ± 3.8 vs 6.9 ± 4.0; P=.018), statin therapy (8.8 ± 3.8 vs 6.9 ± 4.0; P=.018), and past history of hyperlipidemia (8.3 ± 4.2 vs 6.4 ± 3.0; P=.03). The FRS significantly correlated with the angio score (P=.032; r = 0.21). Predictors of the angio score from multivariate analysis are summarized in Table 2.
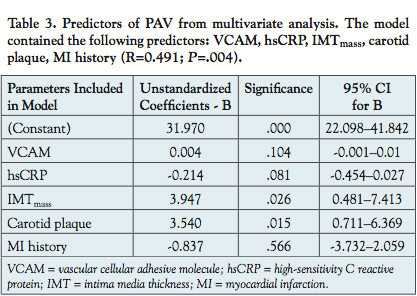 Prediction of PAV. Higher levels of PAV were found in patients with a risk type of HO-1 polymorphism (48.6 ± 6.6% vs 45.8 ± 5.8%; P=.04) and in patients with plaque in the carotid bulb (48.6 ± 5.7% vs 44.7 ± 6.8%; P=.008). PAV correlated with IMTmass (P=.05; r = 0.22). Predictors of PAV from multivariate analyses are summarized in Table 3.
Prediction of PAV. Higher levels of PAV were found in patients with a risk type of HO-1 polymorphism (48.6 ± 6.6% vs 45.8 ± 5.8%; P=.04) and in patients with plaque in the carotid bulb (48.6 ± 5.7% vs 44.7 ± 6.8%; P=.008). PAV correlated with IMTmass (P=.05; r = 0.22). Predictors of PAV from multivariate analyses are summarized in Table 3.
Prediction of NC. The percentage of NC measured using VH-IVUS analysis correlated with FRS (P=.007; r = 0.2), PAV (P=.04; r = 0.2) and inversely with the level of apolipoprotein A (Apo A; P=.047; r = - 0.27). Higher content of NC was found in patients with risk type of HO-1 polymorphism (17.1 ± 8.9% vs 12.7 ± 7.8%; P=.02) and with 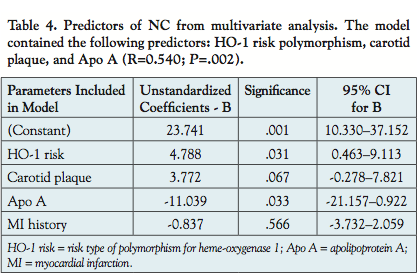 HDLc less than 1.6 mmol/L (15.1 ± 8.5% vs 10.4 ± 7.4%; P=.02). Besides the NC percentage, the PAV also correlated with DC (P=.02; r = 0.23) and inversely with FF (P=.05; r = -0.19). Predictors of NC from multivariate analyses are summarized in Table 4.
HDLc less than 1.6 mmol/L (15.1 ± 8.5% vs 10.4 ± 7.4%; P=.02). Besides the NC percentage, the PAV also correlated with DC (P=.02; r = 0.23) and inversely with FF (P=.05; r = -0.19). Predictors of NC from multivariate analyses are summarized in Table 4.
Prediction of VH-TCFA. Patients with VH-TCFA lesion phenotype more often had an LDLc <2.6 mmol/L on treatment (58.9% vs 34.9%; P=.018), lower level of Apo A (1.19 ± 0.16 mmol/L vs 1.3 ± 0.26 mmol/L; P=.04), higher FRS (9.1 ± 3.1 vs 7.8 ± 3.1; P=.03), and higher angio score (8.9 ± 4.2 vs 6.4 ± 3.2; P=.001)  compared to patients without VH-TCFA. A trend was observed for a more frequent occurrence of VH-TCFA lesion phenotype in patients with the risk type of HO-1 polymorphism (51.1% vs 30.3%; P=.06). However, the important role of the HO-1 polymorphism in the prediction of VH-TCFA was confirmed by multivariate analyses. The predictors of VH-TCFA from the multivariate analysis are summarized in Table 5.
compared to patients without VH-TCFA. A trend was observed for a more frequent occurrence of VH-TCFA lesion phenotype in patients with the risk type of HO-1 polymorphism (51.1% vs 30.3%; P=.06). However, the important role of the HO-1 polymorphism in the prediction of VH-TCFA was confirmed by multivariate analyses. The predictors of VH-TCFA from the multivariate analysis are summarized in Table 5.
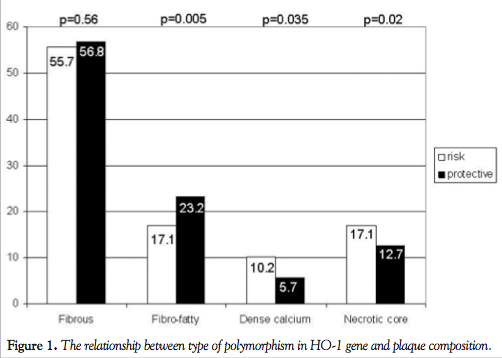
The polymorphism of HO-1 gene. The risk type of polymorphism in the HO-1 gene was found more frequently in patients with a history of MI (61.3% vs 32%; P=.0097) and in patients with diabetes (68.4% vs 35.5%; P=.011). In addition, patients with the high-risk type of polymorphism in the HO-1 gene had a higher FRS (21.5 ± 12.5 vs 15.7 ± 8.0; P=.014), higher angio score (9.1 ± 4.2 vs 6.9 ± 3.1; P=.008), and also a higher PAV (results are mentioned above) than patients with the protective type of polymorphism in the HO-1 gene. The relationship between the specific type of HO-1 polymorphism and the plaque composition is shown in Figure 1.
Discussion
The main findings of our study are as follows:
 (1) High-risk type polymorphism of HO-1 gene was found more frequently in high-risk patients (MI in past, DM, higher FRS).
(1) High-risk type polymorphism of HO-1 gene was found more frequently in high-risk patients (MI in past, DM, higher FRS).
(2) High-risk type polymorphism of HO-1 correlated with extent of atherosclerosis (angio score and PAV) as well as plaque risk profile (larger NC and more frequent VH-TCFA).
(3) Carotid ultrasound and Apo A level can improve the prediction of coronary atherosclerosis PAV (carotid ultrasound) and plaque risk profile (Apo A).
(4) Complex risk assessment is necessary for prediction of high-risk patients and the extent of coronary atherosclerosis.
Polymorphism in HO-1 gene and high-risk patients. We found a higher occurrence of a high-risk polymorphism in HO-1 gene in patients with a past history of MI, in patients with DM, and in patients with higher FRS. The common factor for cardiovascular disease and DM is an increased activity of reactive oxygen species (ROS).15 Low activity of HO-1 increases levels of intracellular ROS that is associated with insulin resistance in adipocytes.16 The HO-1 system has been shown to suppress insulin resistance17 and enhance insulin sensitivity. Hemin, an inducer of the HO system, is effective against streptozocin-induced diabetes.18 Oda et al19 have shown a negative association between bilirubin level and glycosylated hemoglobin (HbA1c) in healthy Japanese men and women.
In animal studies, the absence of HO-1 renders animals more susceptible to myocardial ischemia/reperfusion damage,20 while induction of HO-1 can act protectively against cardiac ischemia/reperfusion in vivo.21 Induction of HO-1 increases adult cardiomyocyte tolerance to ischemia after in vivo transplantation.22 Furthermore, CO has been shown to inhibit platelet aggregation.23 These findings are consistent with the higher occurrence of MI in patients with the high-risk type of HO-1 polymorphism.
The activity of HO-1 plays an important protective role not only in development of DM and MI, but also in the development of arterial hypertension. The HO-1 system serves as a negative control mechanism to the pressor activity of angiotensin II21 while CO regulates blood pressure cooperatively with NO.24 The higher frequency of DM and arterial hypertension are consistent with the higher FRS in patients with the risk polymorphism in the HO-1 gene.
Polymorphism in HO-1 gene and prediction of coronary atherosclerosis. We found higher angio scores, greater PAV, more NC together with DC, and lower FF tissue percentages in patients with the risk type of HO-1 polymorphism. Greater PAV and necrotic core are known risk features of unstable plaques. On the other hand, the role of calcifications inside plaque remains unclear. Calcified plaques are thought to be stable; however, microcalcifications increase plaque vulnerability, ie, they increase risk of plaque rupture for higher plaque stiffness.25 Thus, carriers of the high-risk type of HO-1 polymorphism developed more pronounced coronary atherosclerosis with a higher-risk profile. Li et al26 found higher expression of HO-1 in patients with CAD and levels of HO-1 protein were highest in those with a greater disease burden. It seems that HO-1 expression is a consequence of the disease process and so may be a defense mechanism.27 The mechanism of anti-atherosclerotic effects of HO-1 is the reduction of ROS, reduction of inflammatory mediators, and a reversion of decreased activity of endothelial NO synthase caused by oxidized LDLc and TNF alpha.28 It was found that CO has an anti-apoptotic effect29 and induction of HO-1 prevents cell death.30 These pathways are probably responsible for transforming the plaque composition from primarily fibrous and fibro-fatty to containing increasingly more necrotic tissue with calcifications.
Carotid ultrasound and Apo A level. We did not find a robust correlation between carotid IMT and CAD; rather, we found only borderline correlation between IMTmass and plaque volume. A similar finding was published in the study done by Kranjec.31 It is known that carotid IMT is an independent but relatively modest predictive factor for CAD.32 Moreover, Wald et al33 published a large meta-analysis of 18 studies including 44,861 patients that found a detection rate lower than 65% for CAD based on carotid IMT or carotid plaque.
In contrast, patients with plaque present in the carotid bulb had higher PAV. The presence of carotid plaques seems to be a better predictor for coronary atherosclerosis34 and cardiac event than elevated IMT.35-37 Nicholls et al described in more than 4000 patients the relationship between increasing burden of coronary atherosclerosis, as determined by IVUS, and subsequent clinical outcomes.38
Apo A inversely correlated with amount of NC (better than HDLc). Furthermore, Apo A and the high-risk type of HO-1 polymorphisms were identified as independent predictors of NC using multivariate analysis. We found correlations between VH-TCFA and levels of ApoA. Van Craeyld et al39 found in an experimental mouse model that increased HDLc following ApoA-1 gene transfer elevates collagen content in atherosclerotic lesions. These results confirm the role of Apo A in the process of plaque stabilization. The necessity to implement Apo A assessment among classical risk factors was reiterated in the study by Walldius et al.40
Complex risk assessment is necessary for prediction of high-risk plaque profile. FRS, age, and angio score correlated with occurrence of VH-TCFA. Rodriguez-Granillo et al41 did not find a significant correlation between the occurrence of VH-TCFA and separate atherosclerotic risk factors; more complex risk assessment using the FRS was a predictor for VH-TCFA in the study done by Marso,42 and higher FRS was associated with a higher occurrence of VH-TCFA in the PREDICT study.43 FRS also correlated with NC content in plaques and with angio score. These data underline the necessity of more complex assessment of atherosclerotic risk factors such as FRS for plaque risk profile and extent of coronary atherosclerosis.
The more frequent occurrence of VH-TCFA and higher angio score in patients with LDLc <2.6 mmol/L was problematic. However, these patients were in the well-treated high-risk group where we found more diabetics (68% vs 41.3%; P=.02), more smokers (55.7% vs 35.9%; P=.05), and more patients with a prior MI (69.1% vs 32.8%; P=.0003). It is not surprising that lipid levels in well-treated patients with DM or a history of an MI were lower compared to patients with “only” hyperlipidemia. However, lipid-lowering therapy successfully decreased the level of LDLc, but unfortunately failed to change plaque composition in terms of reducing NC as it was demonstrated in the IBIS-244 and HEAVEN45 trials.
The presence of VH-TCFA in 56.4% of patients with stable angina agrees with a study done by Hong et al,46 which analyzed all three coronary arteries with VH-IVUS and found 1.7 VH-TCFAs per patient with stable angina.
Conclusions
The main finding of this study is the correlation between the HO-1 risk type polymorphism and high-risk plaque features (higher plaque volume, larger NC). These types of plaque together with more frequent DM can probably explain the higher number of MIs in patients with risk HO-1 polymorphism. Based on our results, we can recommend implementation of genetic polymorphism for HO-1 screening in addition to the traditional risk assessment of CAD. HO-1 GT repeat genotyping and the subsequent distribution of patients based on the presence of high-risk HO-1 polymorphisms (generally, the presence of more than 25 GT repeats in the HO-1 gene promoter) and protective HO-1 polymorphisms (generally, the presence of less than 25 GT repeats in the HO-1 gene promoter, as described in the Methods section) is currently relatively easy to perform. Analysis of these polymorphisms may improve the prediction accuracy of the plaque risk profile, especially the prediction of necrotic core and VH TCFA. We expect that inducers of HO-1 or CO-donors may represent a new treatment approach for patients with CAD.
Additional non-invasive parameters were shown to further improve CAD prediction. The presence of plaque in carotid bulb correlated with plaque volume and was a better predictor than carotid IMT. Low level of Apo A was a predictor for high-risk plaque features, such as a large NC and the finding of a VH-TCFA.
The presented study indicates that genetic risk factors are likely to play an important diagnostic and eventually treatment role in the comprehensive management of cardiovascular disease.
Study limitations. A limitation of the present study is the relatively small number of patients enrolled, especially considering the assessment of possible correlation between the atherosclerotic risk factors and plaque composition. Additionally, only 80.2% of patients underwent genetic analysis; however, the study sample size is sufficient to generate statistically significant results and thus allow initial conclusions to be drawn. Finally, the study allowed detailed VH-IVUS assessment of only one plaque in a single coronary artery per subject.
Acknowledgments. The authors thank Dr. Dean Kellog, Jr. (University of Texas Health Science Center at San Antonio, Texas, United States) for critical reading of the manuscript.
References
- Nguyen-Thanh HT, Benzaquen BS. Screening for subclinical coronary artery disease measuring carotid intima media thickness. Am J Cardiol. 2009;104(10):1383-1388.
- van Wijk DF, Boekholdt SM. Improving risk stratification for cardiovascular disease. Expert Rev Cardiovasc Ther. 2010;8(8):1091-1109.
- Kral A, Kovarnik T, Kralik L, et al. Genetic variants in haem oxygenase-1 and endothelial nitric oxide synthase influence the extent and evolution of coronary artery atherosclerosis. Folia Biologica (Praha). 2011;57(5):182-190.
- Taha H, Skrzypek K, Guevara I, et al. Role of heme oxygenase-1 in human endothelial cells: lesson from the promoter allelic variants. Arterioscler Thromb Vasc Biol. 2010;30(8):1634-1641.
- Hayashi S, Omata Y, Sakamoto H, Hara T, Sagara Y, Noguchi M. Characterization of rat heme oxygenase-3 gene. Implication of processed pseudogenes derived from heme oxygenase-2 gene. Gene. 2004;336(2):241-250.
- Peterson SJ, Frishman WH. Targeting heme oxygenase. Therapeutic implications for diseases of the cardiovascular system. Cardiol Rev. 2009;17(3):99-111.
- Kaneda H, Ohno M, Taguchi J, et al. Heme oxygenase-1 gene promoter polymorphism is associated with coronary artery disease in Japanese patients with coronary risk factors. Arterioscler Thromb Vasc Biol. 2002;22(10):1680-1685.
- Morita T. Heme oxygenase and atherosclerosis. Artherioscler Thromb Vasc Biol. 2005;25(9):1786-1795.
- Virmani R, Burke AP, Kolodgie FD, Farb A. Pathology of thin-cap fibroatheroma: a type of vulnerable plaque. J Interv Cardiol. 2003;16(3):267-272.
- Stone GW, Maehara A, Lansky A, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364(3):226-235.
- Wilson P, D´Agostino R, Levy D, Belanger A, Silbershatz H, Kannel W. Prediction of coronary heart disease using risk factors categories. Circulation. 1998;97(18):1837-1847.
- Nambi V, Chambless L, Folsom AR, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis Risk In Communities) study. J Am Coll Cardiol. 2010;55(15):1600-1607.
- García-García HM, Mintz GS, Lerman A, et al. Tissue characterisation using intravascular radiofrequency data analysis: recommendations for acquisition, analysis, interpretation and reporting. Eurointervention. 2009;5(2):177-189.
- Wald DS, Bestwick JP, Morton G, et al. Combining carotid intima-media thickness with carotid plaque on screening for coronary heart disease. J Med Screen. 2009;16(3):155-159.
- Abraham NG, Kappas A. Pharmacological and clinical aspects of heme oxygenase. Pharmacol Rev. 2008;60(1):79-127.
- Lin Y, Berg AH, Iyengar P, et al. The hyperglycemia-induced inflammatory response in adipocytes: the role of reactive oxygen species. J Biol Chem. 2005;280(6):4617-4626
- Ndisang JF, Lane N, Syed N, Jadhav A. Up-regulating the heme oxygenase system with hemin improves insulin sensitivity and glucose metabolism in adult spontaneously hypertensive rats. Endocrinology. 2010;151(2):549-560.
- Ndisang JF, Jadhav A. Heme oxygenase system enhances insulin sensitivity and glucose metabolism in streptozotocin-induced diabetes. Am J Physiol Endocrinol Metab. 2009;296(4):E829-E841.
- Oda E, Kawai R. Bilirubin is negatively associated with hemoglobin A1c independently of other cardiovascular risk factors in apparently healthy Japanese men and women. Circ J. 2011;75(1):190-195.
- Liu X, Wei J, Peng DH, Layne MD, Yet SF. Absence of heme oxygenase-1 exacerbates myocardial ischemia/reperfusion injury in diabetic mice. Diabetes. 2005;54(3):778-784.
- Hangaishi M, Ishizaka N, Aizawa T, et al. Induction of heme oxygenase-1 can act protectively against cardiac ischemia/reperfusion in vivo. Biochem Biophys Res Commun. 2000;279(2):582-588.
- Abraham NG, Kappas A. Heme oxygenase and the cardiovascular and renal system. Free Radic Biol Med. 2005;39(1):1-25.
- Beltowski J, Jamroz A, Borkowska E. Heme oxygenase and carbon monoxide in the physiology and pathology of the cardiovascular system. Postepy Hig Med Dosw (Online). 2004;58:83-99.
- Ushiyama M, Morita T, Katayama S. Carbon monoxide regulates blood pressure cooperatively with nitric oxide in hypertensive rats. Heart Vessels. 2002;16(5):189-195.
- Bluestein D, Alemu Y, Avrahami I, et al. Influence of microcalcifications on vulnerable plaque mechanics using FSI modeling. J Biomech. 2008;41(5):1111-1118.
- Li YG, Wang DM, Chen SM, et al. Heme oxygenase-1 expression and coronary heart disease — association between levels of heme oxygenase-1 expression and angiographic morphology as well as the quantity of coronary lesions. Acta Cardiol. 2006;61(3):295-300.
- Idriss NK, Blann AD, Lip G. Hemoxygenase-1 in cardiovascular disease. J Am Coll Cardiol. 2008;52(12):971-978.
- Kawamura K, Ishikawa K, Wada Y, et al. Bilirubin from heme oxygenase-1 attenuates vascular endothelial activation and dysfunction. Arterioscler Thromb Vasc Biol. 2005;25(1):155-160.
- Otterbein LE, Kolls JK, Mantell LL, Cook JL, Alam J, Choi AM. Exogenous administration of heme oxygenase-1 by gene transfer provides protection against hyperoxia-induced lung injury. J Clin Invest. 1999;103(7):1047-1054.
- Ferris CD, Jaffrey SR, Sawa A, et al. Heme oxygenase-1 prevents cell death by regulating cellular iron. Nat Cell Biol. 1999;1(3):152-157.
- Kranjec I. Atherosclerotic burden in coronary and peripheral arteries in patients with first clinical manifestation of coronary artery disease. J Cardiovasc Med. 2011;12(4):297-299.
- Simon A, Megnien JL, Chironi G. The value of carotid intima-media thickness for predicting cardiovascular risk. Arterioscler Thromb Vasc Biol. 2010;30(2):182-185.
- Wald DS, Bestwick JP. Carotid ultrasound screening for coronary heart disease: results based on a meta-analysis of 18 studies and 44,861 subjects. J Med Screen. 2009;16(3):147-154.
- Belcaro G, Nicolaides AN, Laurora G, et al. Ultrasound morphology classification of the arterial wall and cardiovascular events in a 6-year follow-up study. Arterioscler Thromb Vasc Biol. 1996;16(7):851-856.
- Morito N, Inoue Y, Urata M, et al. Increased carotid artery plaque score is an independent predictor of the presence and severity of coronary artery disease. J Cardiol. 2008;51(1):25-32.
- Inaba Y, Chen JA, Bergmann SR. Carotid plaque, compared with carotid intima-media thickness, more accurately predicts coronary artery disease events: a meta-analysis. Atheroscleroris. 2012;220(1):128-133.
- Seo Y, Watanabe D, Ishizu T, et al. Echolucent carotid plaques as a feature in patients with acute coronary syndrome. Circ J. 2006;70(12):1629-1634.
- Nicholls SJ, Hsu A, Wolski K, et al. Intravascular ultrasound-derived measures of coronary atherosclerotic plaque burden and clinical outcome. J Am Coll Cardiol. 2010;55(21):2399-2407.
- Van Craeyveld E, Gordts SG, Nefyodova E, Jacobs F, De Geest B. Regression and stabilization of advanced murine atherosclerotic lesions: a comparison of LDL lowering and HDL raising gene transfer strategies. J Mol Med. 2011;89(6):555-567.
- Walldius G, Jungner I. Apolipoprotein A-1 versus HDL cholesterol in the prediction of risk for myocardial infarction and stroke. Curr Opin Cardiol. 2007;22(4):359-367.
- Rodriguez-Granillo GA, Garcia-Garcia HM, McFadden EP, et al. In vivo intravascular ultrasound-derived thin-cap fibroatheroma detection using ultrasound radiofrequency data analysis. J Am Coll Cardiol. 2005;46(11):2038-2042.
- Marso SP, Frutkin AD, Mehta SK, et al. Intravascular ultrasound measures of coronary atherosclerosis are associated with the Framingham risk score: an analysis from a global IVUS registry. EuroIntervention. 2009;5(2):212-218.
- Abdel-Wahab M, Khattab AA, Liska B, et al. Relationship between cardiovascular risk as predicted by established risk scores and coronary artery plaque composition as detected by virtual histology intravascular ultrasound analysis. The PREDICT pilot study. EuroIntervention. 2008;3(4):482-489.
- Serruys PW, Garcia-Garcia HM, Buszman P, et al. Effects of the direct lipoprotein-associated phospholipase A2 inhibitor darapladib on human coronary atherosclerosis plaque. Circulation. 2008;118(11):1172-1182.
- Kovarnik T, Mintz GS, Skalicka H, et al. Virtual histology evaluation of atherosclerosis regression during atorvastatin and ezetimibe administration — HEAVEN study. Circ J. 2012;76(1):176-183.
- Hong MH, Mintz GS, Lee CW, et al. A three-vessel virtual histology intravascular ultrasound analysis of frequency and distribution of thin-cap fibroatheromas in patients with acute coronary syndromes or stable angina pectoris. Am J Cardiol. 2008;101(5):568-572.
From the 12nd Department of Medicine – Department of Cardiovascular Medicine, First Faculty of Medicine, Charles University in Prague and General University Hospital in Prague, Czech Republic, 2Cardiovascular Research Foundation, New York New York, 3Department of Pediatrics, First Faculty of Medicine, Charles University in Prague and General University Hospital in Prague, Czech Republic, 4Institute for Research and Development of Education, Faculty of Education, Charles University in Prague, Czech Republic, 5Department of Electrical and Computer Engineering, The University of Iowa, Iowa City, Iowa, and 6Department of Laboratory Diagnostics, First Faculty of Medicine, Charles University in Prague, and General University Hospital in Prague, Czech Republic.
Funding: This work was supported by IGA (Internal Grant Agency of Czech Ministry of Health) NR 9214-3 grant, Charles University (UNCE 204011/2012 and P24/LF1/3) grants, and by the US National Institutes of Health grant R01 HL063373.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Mintz reports that he is a consultant to and receives grant support from Volcano Corporation, and honoraria and grant support from Boston Scientific. The other authors report no disclosures related to the content herein.
Manuscript submitted May 10, 2012, provisional acceptance given August 16, 2012, final version accepted October 18, 2012.
Address for correspondence: Tomas Kovarnik, MD, PhD, 2nd Department of Medicine – Department of Cardiovascular Medicine, First Faculty of Medicine, Charles University in Prague and General University Hospital in Prague, II. interni klinika, U nemocnice 2, Prague, 12808 Czech Republic. Email: tomas.kovarnik@vfn.cz











