

Predictive Value of SYNTAX Score in Risk Stratification of Patients Undergoing Unprotected Left Main Coronary Artery Angioplasty
Abstract: Background. The SYNTAX score is a useful tool to evaluate percutaneous coronary intervention risk regarding the number, complexity, and location of lesions. Despite its proven value in the prognosis of three-vessel disease, there are few data about its usefulness in other selected subsets of patients. This study aimed to evaluate the prognostic value of the SYNTAX score in a population of patients who underwent unprotected left main coronary artery (ULMCA) angioplasty in our hospital. Methods. This was a single-center study that included 118 patients (79.7% male; mean age, 66 ± 12 years) who underwent ULMCA angioplasty between March 1999 and December 2008. Multivariate Cox logistic regression analysis was used to assess the relation of SYNTAX score to the incidence of cardiovascular death and major adverse cardiac events (MACE) — an endpoint comprised of cardiovascular death, non-fatal acute myocardial infarction, and target vessel revascularization. Results. At 30 days, there were 5 cardiovascular deaths (4.2%). In the mean follow-up of 32 ± 24 months, there were 17 cardiovascular deaths (14.4%) and 30 MACE (25.4%). At 30 days, SYNTAX score had no predictive value, but at long-term follow-up, it significantly predicted the occurrence of cardiovascular death (adjusted hazard ratio, 1.069; 95% CI, 1.030-1.109; P<.0001) and MACE (adjusted hazard ratio, 1.044; 95% CI, 1.013-1.076; P=.005), even after adjustment for potential confounders. Area under the curve for the occurrence of cardiovascular death and MACE was 0.75 (P=.0006) and 0.63 (P=.032), respectively. Conclusions. In this population of patients undergoing ULMCA angioplasty, SYNTAX score was demonstrated to be a valuable tool to predict long-term cardiovascular mortality.
J INVASIVE CARDIOL 2011;23(12):494-499
Key words: SYNTAX score, unprotected left main angioplasty
___________________________________________
Unprotected left main coronary artery (ULMCA) stenosis is one of the most challenging findings of a coronary angiography; due to its critical location, acute occlusion is rapidly fatal, and medical treatment carries a poor prognosis with a 1-year mortality of approximately 20%.1 Several randomized clinical trials in the 1970s and 1980s unequivocally demonstrated the superiority of coronary artery bypass graft surgery (CABG) over medical therapy and early attempts by interventional cardiologists to treat ULMCA disease with balloon angioplasty2 and bare-metal stents (BMS) resulted in high rates of restenosis, leading to repeat revascularization and even sudden death. However, the evolution of percutaneous coronary intervention (PCI), especially the advent of drug-eluting stents (DES), manifested by an unequivocal reduction in restenosis rates, has led to a renewed interest in the percutaneous approach of left main lesions. A recent meta-analysis of eight studies including nearly 3000 patients comparing PCI and CABG suggests that there is no difference between the two strategies regarding the clinical endpoints of stroke, myocardial infarction, and death, although repeat revascularization is consistently higher following ULMCA PCI.3
PCI risk stratification is an emerging subject and even EuroSCORE, which is a surgical risk stratification score, has been applied to the ULMCA PCI population.4 The SYNTAX score, an angiographic classification system that aims to characterize coronary anatomy regarding the number, location, and complexity of lesions, was designed to predict cardiovascular outcomes in patients with three-vessel or ULMCA disease in the SYNTAX study.5-7 Higher SYNTAX scores are related to more complex disease and therefore are likely to lead to a worse prognosis in patients undergoing PCI.
The aim of our study was to evaluate the performance of SYNTAX score in predicting short- and long-term outcomes of a single-center population of patients undergoing ULMCA angioplasty.
Methods
Patient population and data collection. This was a single-center, retrospective, observational study that included 118 patients who underwent ULMCA angioplasty between March 1999 and December 2008 with at least one stent implanted in the left main coronary artery (BMS or DES). The left main stem was defined as unprotected if there was no patent bypass graft to the left anterior descending artery (LAD) or circumflex (CX) artery. The studied population was divided into three groups according to their SYNTAX score tertiles (low score if <17; intermediate score if ≥17 and ≤28; and high score if >28). It must be pointed out that these SYNTAX score tertiles are different from those that were used in the SYNTAX trial, as this gives us better comprehension of the distribution of the SYNTAX score in our population and allows us to have well-balanced groups regarding the number of patients.
Patients were followed for the occurrence of major adverse cardiac events (MACE) as required by our continuous ongoing institutional registry (ACROSS). Post-discharge clinical follow-up was conducted by telephone interview. All angiograms were retrospectively visualized by two reviewers for assessment of the angiographic variables necessary for SYNTAX score calculation and blinded for clinical outcomes. In case of discrepancy between the reviewers’ scores, a third observer was consulted for a consensus to be reached. All data were entered into a centralized database (CardioBase).
Definitions. Acute myocardial infarction (AMI) during follow-up was defined as a clinical event with any new elevation of troponin I or creatine kinase-MB above the upper normal limit and included both ST- and non-ST elevation MI. Target vessel revascularization (TVR) and target lesion revascularization (TLR) were defined as any revascularization procedure of the target vessel or target lesion (from 5 mm distal to the stent up to 5 mm proximal to the stent), respectively. Cardiovascular death was defined as death due to a demonstrable cardiovascular cause or any unexplained death. MACE were the composite outcome of cardiovascular death, non-fatal MI, and TVR.
Statistical analysis. Baseline and outcome variables were compared using student’s unpaired t-test or Mann-Whitney test for continuous variables, and the Chi-square test or Fisher exact test for categorical variables. The normality assumption for continuous variables was assessed by the Kolmogorov-Smirnov test. Event-free survival was computed using Kaplan-Meyer estimates and compared between groups with the log-rank test. The predictors of cardiovascular death and MACE were found by multivariate analysis with a Cox proportional hazard regression model. The discriminative capacity of SYNTAX score was analyzed by ROC curves. All P-values were 2-sided, and P<.05 was considered statistically significant. All analyses were conducted with SPSS version 17 statistical analysis software (SPSS Inc.).
Results
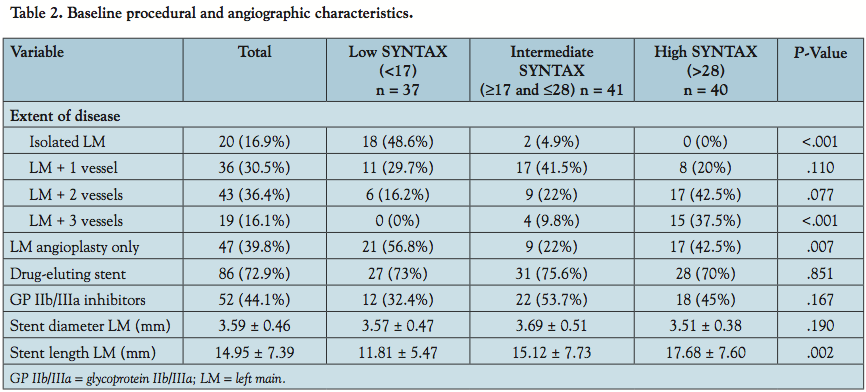
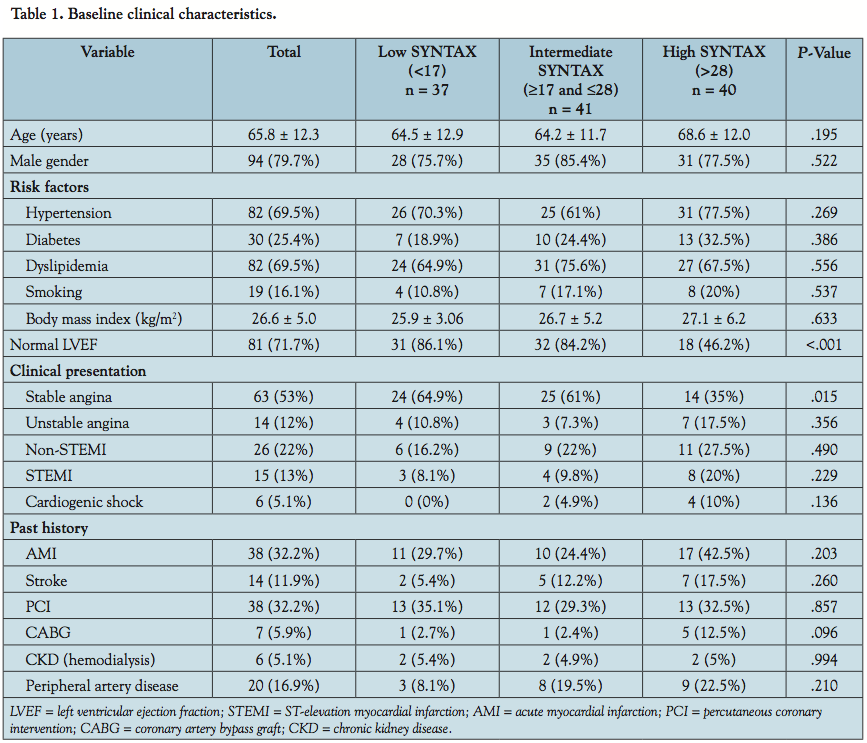 Baseline clinical, angiographic, and procedural variables. The mean overall SYNTAX score was 24.5 ± 11.8. The baseline clinical, angiographic, and procedural characteristics in the whole population and across the SYNTAX score tertiles are shown in Tables 1 and 2. Patients with higher SYNTAX scores were more likely to have depressed left ventricular ejection fraction (LVEF) and presented more often with acute coronary syndrome. As expected, higher scores were also related with more diseased vessels and a greater length of implanted stents.
Baseline clinical, angiographic, and procedural variables. The mean overall SYNTAX score was 24.5 ± 11.8. The baseline clinical, angiographic, and procedural characteristics in the whole population and across the SYNTAX score tertiles are shown in Tables 1 and 2. Patients with higher SYNTAX scores were more likely to have depressed left ventricular ejection fraction (LVEF) and presented more often with acute coronary syndrome. As expected, higher scores were also related with more diseased vessels and a greater length of implanted stents.
 30-day outcomes. There were 5 cardiovascular deaths (4.2%) and no other MACE during the first month. One death occurred in the low SYNTAX tertile (2.7%), 1 death in the intermediate tertile (2.4%), and 3 deaths in the higher tertile (7.5%); P=.451. By univariate analysis, SYNTAX score was not a predictor of mortality at 30 days: hazard ratio (HR), 1.024; 95% confidence interval (CI), 0.959-1.094; P=.481.
30-day outcomes. There were 5 cardiovascular deaths (4.2%) and no other MACE during the first month. One death occurred in the low SYNTAX tertile (2.7%), 1 death in the intermediate tertile (2.4%), and 3 deaths in the higher tertile (7.5%); P=.451. By univariate analysis, SYNTAX score was not a predictor of mortality at 30 days: hazard ratio (HR), 1.024; 95% confidence interval (CI), 0.959-1.094; P=.481.
Long-term outcomes. During the mean follow-up of 32 ± 24 months, 17 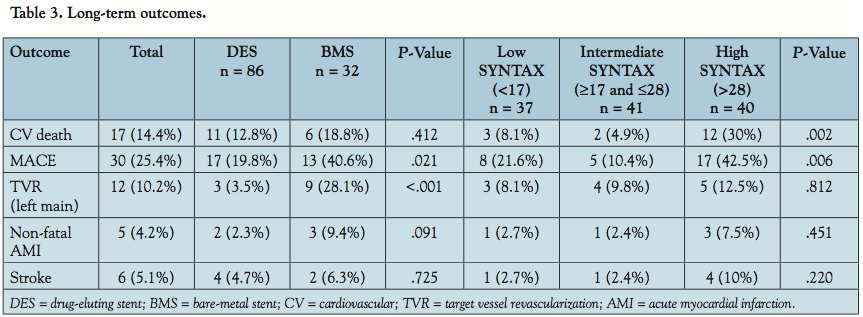 deaths (14.4%), and 30 MACE (25.4%) occurred. The rates of cardiovascular death were 8.1%, 4.9%, and 30% in patients with low, intermediate, and high SYNTAX scores, respectively. The rates of MACE were 21.6% in the first tertile, 10.4% in the second tertile, and 42.5% in the third tertile. The differences between the groups regarding MACE were mainly driven by cardiovascular death, since although there was a trend for a higher rate of TVR, AMI, and stroke in the high-score tertile, there were no statistically significant differences (Table 3). There were no significant differences between DES and BMS concerning cardiovascular death, but patients with BMS had higher rates of MACE, mainly due to repeat revascularization of the left main (Table 3).
deaths (14.4%), and 30 MACE (25.4%) occurred. The rates of cardiovascular death were 8.1%, 4.9%, and 30% in patients with low, intermediate, and high SYNTAX scores, respectively. The rates of MACE were 21.6% in the first tertile, 10.4% in the second tertile, and 42.5% in the third tertile. The differences between the groups regarding MACE were mainly driven by cardiovascular death, since although there was a trend for a higher rate of TVR, AMI, and stroke in the high-score tertile, there were no statistically significant differences (Table 3). There were no significant differences between DES and BMS concerning cardiovascular death, but patients with BMS had higher rates of MACE, mainly due to repeat revascularization of the left main (Table 3).
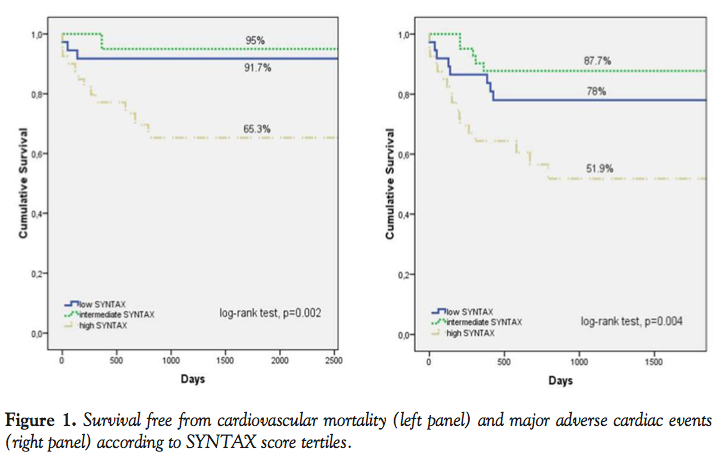 The cumulative incidence of survival free from cardiovascular death and MACE during the entire follow-up stratified across the SYNTAX score tertiles is shown in Figure 1.
The cumulative incidence of survival free from cardiovascular death and MACE during the entire follow-up stratified across the SYNTAX score tertiles is shown in Figure 1.
By univariate analysis, SYNTAX score was a predictor of long-term mortality (HR, 1.064; 95% CI, 1.030-1.100; P<.001) and MACE (HR, 1.036; 95% CI, 1.008-1.065; P=.01). Other predictors of long-term outcomes are presented in Figure 2.
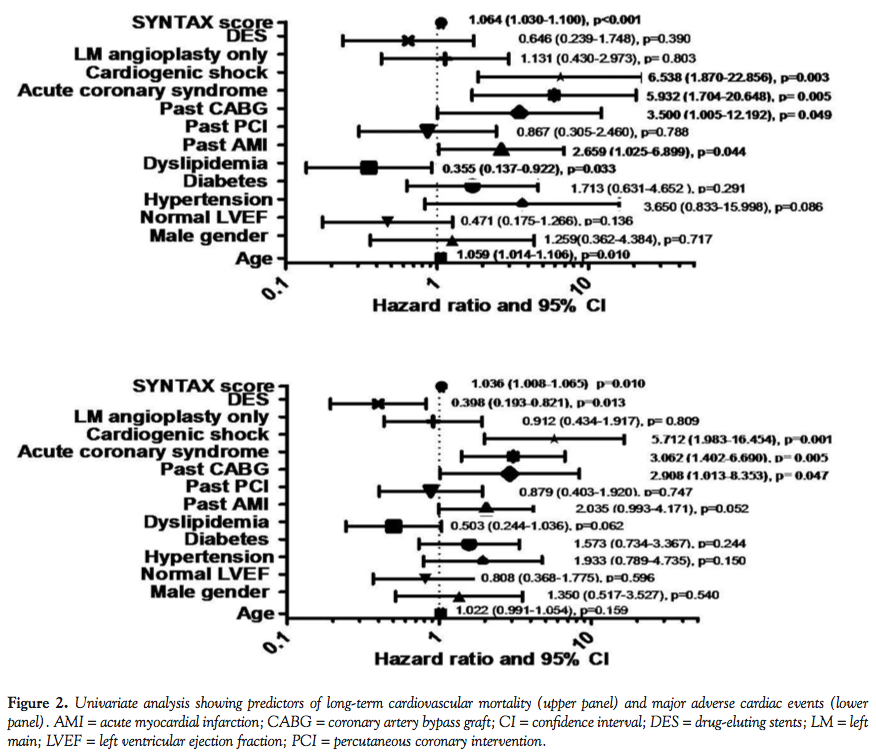 Multivariable analysis. After adjustment for potential confounders (age, gender, LVEF, diabetes, dyslipidemia, past AMI, past CABG, acute coronary syndrome in presentation, cardiogenic shock, and type of stent), SYNTAX score was the only independent predictor of long-term cardiovascular death (HR, 1.067; 95% CI, 1.032-1.104; P<.001) and remained an independent predictor of MACE (HR, 1.037; 95% CI, 1.008-1.066; P=.012), along with cardiogenic shock (HR, 3.808; 95% CI, 1.135-12.779; P=.03) and use of DES (HR, 0.385; 95% CI, 0.184-0.803; P=.011).
Multivariable analysis. After adjustment for potential confounders (age, gender, LVEF, diabetes, dyslipidemia, past AMI, past CABG, acute coronary syndrome in presentation, cardiogenic shock, and type of stent), SYNTAX score was the only independent predictor of long-term cardiovascular death (HR, 1.067; 95% CI, 1.032-1.104; P<.001) and remained an independent predictor of MACE (HR, 1.037; 95% CI, 1.008-1.066; P=.012), along with cardiogenic shock (HR, 3.808; 95% CI, 1.135-12.779; P=.03) and use of DES (HR, 0.385; 95% CI, 0.184-0.803; P=.011).
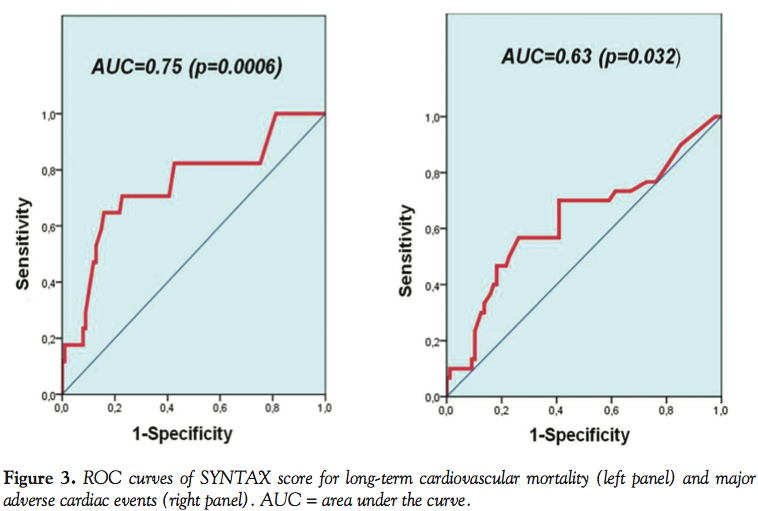 Discriminatory performance. The c-statistic of SYNTAX score for long-term cardiovascular mortality and MACE was 0.75 and 0.63, respectively (Figure 3). The scores of 32.5 and 28 were the optimal cut-off values to discriminate between high- and low-risk patients for cardiovascular death and MACE, respectively. When the patients were stratified according to those cut-off values, the hazard ratio of SYNTAX score for the occurrence of cardiovascular death was 8.687; 95% CI, 3.009-25.076; P<.001 and the hazard ratio of SYNTAX score for occurrence of MACE was 3.013; 95% CI, 1.435-6.328; P=.004.
Discriminatory performance. The c-statistic of SYNTAX score for long-term cardiovascular mortality and MACE was 0.75 and 0.63, respectively (Figure 3). The scores of 32.5 and 28 were the optimal cut-off values to discriminate between high- and low-risk patients for cardiovascular death and MACE, respectively. When the patients were stratified according to those cut-off values, the hazard ratio of SYNTAX score for the occurrence of cardiovascular death was 8.687; 95% CI, 3.009-25.076; P<.001 and the hazard ratio of SYNTAX score for occurrence of MACE was 3.013; 95% CI, 1.435-6.328; P=.004.
Discussion
Risk assessment is a key feature when evaluating the most suitable myocardial revascularization strategy, and its value applies not only to the physician but also to the patient who must play an active role throughout the decision-making process. Furthermore, it allows quality control as it is a tool for operators and institutions to evaluate and compare performance. Recently, the guidelines on myocardial revascularization have recommended SYNTAX score as a risk stratification score to be used in candidates for percutaneous coronary intervention (class IIa, level of evidence B) but not for CABG (class III, level of evidence B).8 This recommendation was based on a single randomized trial;5 since then, the use of the SYNTAX score has gained widespread interest in various subsets of patients. This risk model was first assessed in the ARTS II (Arterial Revascularization Therapies Study part II) trial designed for multivessel coronary disease and it showed a better ability to predict early and long-term MACCE than the previous angiographic classification of the American College of Cardiology/American Heart Association.9 However, a recent study by Kim et al that evaluated the performance of SYNTAX score for prediction of outcomes after ULMCA revascularization in a large multicenter Asian registry10 reported that this risk model was only modestly predictive of 3-year outcomes in patients treated with DES, less predictive after BMS implantation and not surprisingly even worse in predicting outcomes after CABG.
We consider the following key points as the main findings of our study: SYNTAX score is an independent predictor of long-term cardiovascular death (HR, 1.067; 95% CI, 1.032-1.104) and MACE (HR, 1.037; 95% CI, 1.008-1.066), but not a predictor of early outcomes (although there were few 30-day events in our study and we can hypothesize that with a larger population the results would have been different concerning this endpoint). The c-statistic of SYNTAX score for long-term cardiac mortality and MACE is 0.75 and 0.63, respectively. These results are in agreement with a previous study showing the benefit of SYNTAX score in predicting long-term outcomes after PCI for ULMCA disease.11
The SYNTAX score has a better performance at predicting long-term cardiovascular mortality than the composite endpoint of MACE. When each outcome was analyzed individually, we observed that the rates of TVR (8.1% in the lowest tertile, 9.8% in the intermediate tertile, and 12.5% in the highest tertile) and non-fatal MI (2.4% in the lowest tertile, 2.4% in the intermediate tertile, and 7.5% in the highest tertile) were not significantly different across the SYNTAX score risk tertiles. As a conclusion, cardiovascular mortality accounts for the differences in MACE across the tertiles and the ability of SYNTAX score to predict this composite outcome is given mainly by its performance in predicting cardiovascular death. However, there are pitfalls regarding this conclusion: for instance, we only considered left main revascularization even though the SYNTAX score takes into account all the significant stenoses in the coronary vasculature; in theory, if we had assessed repeat revascularization of all treated vessels, the ability of the score to predict it would have been better.
An interesting feature is the poor performance of SYNTAX score in stratifying risk among the low and intermediate tertiles. In fact, the rates of cardiovascular death were 8.1%, 4.9%, and 30% in patients with low, intermediate, and high SYNTAX scores, respectively, and the rates of MACE were 21.6% in the first tertile, 10.4% in the second tertile, and 42.5% in the third tertile. As described in the Methods section, the SYNTAX score tertiles in this study are different from those in the SYNTAX trial in order to achieve an equilibrium between the groups, as the intermediate score group would be much smaller. However, had the SYNTAX trial tertiles been used, the absolute frequency of mortality and MACE within the groups would have been exactly the same and even though the relative frequencies would have changed, we would still observe the poor risk stratification performance among the low and intermediate tertiles. Such a finding is in agreement not only with the study by Valgimigli et al,9 which evaluated this score in multivessel coronary disease, but also with Capodano et al,11 who tested SYNTAX score in left main angioplasty. Our study supports the suggestion by those authors of dichotomizing the score in order to achieve better results. In our case, the optimal cut-off values for mortality and MACE are 32.5 and 28, respectively.
The results of our study demonstrate the usefulness of SYNTAX score in predicting adverse outcomes in this population, but it raises some important questions that suggest caution in using it alone to choose the most appropriate revascularization strategy in each case. In fact, it only takes into account the anatomy, extension, and complexity of coronary artery disease and does not incorporate clinical and procedural factors. This is probably the most important factor that might limit the applicability of SYNTAX score as a tool to indicate angioplasty of left main disease. Indeed, variables such as age, heart failure, or kidney insufficiency have demonstrated their role in outcomes after PCI in previous risk models.12,13 Some authors have addressed this important subject, showing that risk scores that merge clinical and angiographic variables (Global Risk Classification System)14 or even with the addition of procedure characteristics (NERS score)15 have a better predictive ability in ULMCA disease than the SYNTAX score alone.
The population of this study shows many similarities with other contemporary left main revascularization studies. The RESEARCH and T-SEARCH16 registries, for example, have a similar age and male gender prevalence, but a lower burden of diabetes and hypertension. Presentation as acute coronary syndrome and cardiogenic shock is higher in those registries than in ours. On the other hand, the group that compared NERS and SYNTAX score had a younger population, a similar burden of cardiovascular risk factors and prevalence of men, but a lower rate of acute coronary syndrome at presentation.15 Albeit differences and similarities, there are features that make this population unique and that fact has to be taken into account when interpreting these results.
Study limitations. Some limitations may be pointed out in our study. In fact, the limited number of patients may have influenced the power of the results. Moreover, not only DES patients were included but also BMS, which goes against the contemporary practice in ULMCA angioplasty. Also, our analysis did not take into account the location of the lesions in the left main and the different stenting techniques for distal and bifurcation lesions. Not only have there been variations in the stenting strategies throughout the study period, but these also play a role in defining the complexity and success of the procedure and would help to interpret our results. Finally, in spite of accounting for several confounding factors in this analysis, it is not possible to exclude any residual confounders inherent to specific selection criteria for left main stenting, especially if we bear in mind that a large part of this population was included at a period when CABG would be regarded as a more common choice.
Conclusions
SYNTAX score demonstrated a good predictive and discriminative performance for long-term cardiovascular mortality in patients undergoing unprotected LMCA percutaneous intervention. Although it is also a predictor of long-term MACE, its ability to predict this outcome is mainly driven by cardiovascular mortality.
References
- Yusuf S, Zucker D, Peduzzi P, et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet. 1994;344(8922):563-570.
- O’Keefe JH Jr, Hartzler GO, Rutherford BD, et al. Left main coronary angioplasty: early and late results of 127 acute and elective procedures. Am J Cardiol. 1989;64(3):144-147.
- Lee MS, Yang T, Doot J, Liao H. Meta-analysis of clinical studies comparing coronary artery bypass grafting with percutaneous coronary intervention and drug-eluting stents in patients with unprotected left main coronary artery narrowings. Am J Cardiol. 2010;105(8):1070-1075.
- Kim YH, Dangas GD, Solinas E, et al. Effectiveness of drug-eluting stent implantation for patients with unprotected left main coronary artery stenosis. Am J Cardiol. 2008;101(6):801-806.
- Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972.
- Sianos A, Morel MA, Kappentein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005;1(2):219-227.
- Ong ATL, Serruys PW, Mohr FW, et al. The SYNergy between percutaneous coronary intervention with TAXus and cardiac surgery (SYNTAX) study: design, rationale, and run-in phase. Am Heart J. 2006;151(6):1194-1204.
- Wijns W, Kolh P, Danchin N, et al; Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS); European Association for Percutaneous Cardiovascular Interventions (EAPCI). Guidelines on myocardial revascularization. Eur Heart J. 2010;31(20):2501-2555.
- Valgimigli M, Serruys PW, Tsuchida K, et al. Cyphering the complexity of coronary artery disease using the SYNTAX score to predict clinical outcome in patients with three-vessel lumen obstruction undergoing percutaneous coronary intervention. Am J Cardiol. 2007;99(8):1072-1081.
- Kim Y-H, Park D-W, Kim W-J, et al. Validation of SYNTAX (Synergy between PCI with TAXUS and Cardiac Surgery) scores for prediction of outcomes after unprotected left main coronary revascularization. JACC Cardiovasc Interv. 2010;3(6):612-623.
- Capodano D, Di Salvo ME, Cincotta G, et al. Usefulness of the SYNTAX score for predicting clinical outcome after percutaneous coronary intervention of unprotected left main coronary artery disease. Circ Cardiovasc Interv. 2009;2(4):302-308.
- Singh M, Peterson ED, Milford-Beland S, Rumsfeld JS, Spertus JA. Validation of the Mayo Clinic risk score for in-hospital mortality after percutaneous coronary interventions using the National Cardiovascular Data Registry. Circ Cardiovasc Interv. 2008;1(1):36-44.
- Madan P, Elayda MA, Lee V, Wilson JM. Predicting major adverse cardiac events after percutaneous coronary intervention: the Texas Heart Institute risk score. Am Heart J. 2008;155(6):1068-1074.
- Capodano D, Miano M, Cincotta G, et al. EuroSCORE refines the predictive ability of SYNTAX score in patients undergoing left main percutaneous coronary intervention. Am Heart J. 2010;159(1):103-109.
- Chen S, Chen JP, Mintz G, et al. Comparison between the NERS (new risk stratification) score and the SYNTAX (synergy between percutaneous coronary intervention with TAXUS and cardiac surgery) score in outcome prediction for unprotected left main stenting. JACC Cardiovasc Interv. 2010;3(6):632-641.
- Onuma Y, Girasis C, Piazza N, et al. Long-term clinical results following stenting of the left main stem. JACC Cardiovasc Interv. 2010;3(6):584-594.
___________________________________________
From the Hospital Santa Cruz, Carnaxide, Portugal.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 13, 2011, provisional acceptance given August 5, 2011, final version accepted October 6, 2011.
Address for correspondence: Dr. João D. Brito, Hospital Santa Cruz, Cardiology, Av. Prof. Dr. Reinaldo dos Santos, Carnaxide, 2795-053, Portugal. Email: jdbrito@netcabo.pt











