

Prognosis of Patients With Left Circumflex Artery Acute Myocardial Infarction in Relation to ST-Segment on Admission Electrocardiogram
Abstract
Background. Total thrombotic occlusion of the left circumflex (LCX) artery may present without ST-segment elevations; the clinical outcomes of such patients remain unclear. Objective. To examine the difference in clinical outcomes between patients with acute myocardial infarction (MI) due to LCX occlusion or stenosis with and without ST-segment elevation. Methods. The present study is based on an observational, retrospective cohort comprising all patients admitted to 2 centers between 2009 and 2019 with MI due to LCX disease. Clinical outcomes included recurrent percutaneous coronary intervention (PCI), hospitalization due to acute coronary syndrome (ACS), and mortality. Risk factors for mortality were assessed using logistic regression analysis. Results. During the study period, a total of 897 patients with LCX-related MI were treated. Most (56.6%) presented with non-ST segment elevation MI (NSTEMI), which was associated with higher rates of 1-year hospitalization for ACS (15.8% vs 11.1%; P=.05) and PCI (20.9% vs 14.4%; P=.05) compared with ST-segment elevation MI (STEMI) patients. STEMI was associated with higher 30-day mortality compared with NSTEMI (3.9% vs 1.7%, respectively; P=.05), with no difference in mortality after 1 year (6.7% vs 5.6%, respectively; P=.55). Multivariate analysis found left dominant circulation (odds ratio [OR], 2.62; 95% confidence interval [CI], 1.4-4.7) and diabetes mellitus (OR, 2.13; 95% CI, 1.2-3.6) to be independent predictors for 1-year mortality. Conclusion. Patients suffering from NSTEMI and STEMI related to LCX occlusion or stenosis have similar 1-year mortality. Left dominant circulation was associated with higher short- and long-term mortality. These results suggest that a substantial population of patients who present as NSTEMI should be treated as promptly and aggressively as STEMI patients.
J INVASIVE CARDIOL 2021;33(1):E20-E24. doi:10.25270/jic/20.00309
Key words: acute coronary syndrome, left circumflex artery, left dominant coronary arteries
In recent years, accumulating evidence has demonstrated that timely reperfusion is crucial for the improvement of clinical outcomes in patients with myocardial infarction (MI). The admission electrocardiogram (ECG) is vital in order to determine the timing of percutaneous coronary intervention (PCI). Emergency PCI should be performed when the ECG demonstrates elevated ST segments (STEMI).1 In the absence of ST-segment elevation (NSTEMI), the appropriate treatment strategy includes early coronary angiography, usually within the first 72 hours, with subsequent revascularization, when appropriate.2
Typically, patients with thrombotic occlusion of the left anterior descending coronary artery or right coronary artery have a clear ST-segment elevation pattern during the acute phase of MI, and therefore are referred for immediate reperfusion. However, this is not the case in patients with thrombotic occlusion of the left circumflex (LCX) artery. LCX occlusions may often present without ST-segment elevation;3-5 therefore, fewer primary PCIs are performed in these patients. Consequently, there is a higher burden of ischemia and more complications in this subgroup.5,6
To date, little is known about the differences in clinical outcomes of patients with MI involving the LCX as an infarct-related artery (IRA), presenting with or without ST-segment elevation. The present study aims to examine these differences, focusing on short- and long-term clinical outcomes.
Methods
The current analysis is based on a retrospective, observational, 2-center cohort that included all LCX-related acute MI patients admitted to the Rambam Health Care Campus (RHCC) and Hillel Yaffe Medical Centre (HYMC) between January 2009 and June 2019. RHCC and HYMC are both university-affiliated hospitals with coronary catheterization laboratories with a 24/7 on-call service for primary PCI.
The study was approved by the institutional ethics committees of both centers. Informed consent was waived due to the retrospective nature of the study.
All adult patients admitted to either site during the study period who were diagnosed with acute MI and underwent PCI were screened. Only patients with LCX-related acute MI were included in the analysis. The LCX was defined as the IRA if angiography revealed an LCX lesion with reduced Thrombolysis in Myocardial Infarction (TIMI) flow or single-vessel disease with significant (>75%) LCX stenosis. Exclusion criteria included previous coronary artery bypass grafting (CABG), thrombolysis during the index event, and chronic total occlusion of the LCX. MI was defined according to the latest definition available at the time of data extraction and analysis.7
The primary endpoints were 30-day and 1-year mortality. The secondary endpoints included repeat admission due to acute coronary syndrome (ACS) and repeat PCI at 30-day and 1-year follow-up. Repeat admission due to ACS was defined as admission with any ACS diagnosis (MI or unstable angina) as the primary diagnosis at discharge; repeated PCI was defined as any additional PCI during the follow-up period to any coronary vessel.
The exposure variable was the nature of the index event, ie, STEMI vs NSTEMI. We collected a dataset of potential predictors and confounders, including patient demographics, clinical characteristics, laboratory results, and angiographic findings. We also performed a prespecified subgroup analysis according to coronary dominance. A proximal lesion was defined as the infarct-related lesion in the proximal LCX and proximal first obtuse marginal.
Patient data were collected from the medical records. RHCC and HYMC use an electronic patient register that includes clinical, laboratory, and radiological data. Angiographic and procedural data (IRA, TIMI flow, coronary dominance) were extracted from the PCI report. It also has access to the Israeli population records with updated mortality data. Data for RHCC patients were obtained using the Healthcare Data Sandbox (MDClone), while data for HYMC patients was obtained from the hospital cath lab registry.
Statistical analysis. Categorical variables were compared using Pearson’s Chi-square test or the Fisher’s exact test, while continuous variables were compared using the t-test or the Mann-Whitney U-test, as appropriate. Variables found significant on univariate analysis (P<.05) were entered into a multivariate, backward, stepwise, logistic-regression analysis, in which the dependent variable was mortality (both at 30 days and at 1 year). Variables that were not found to contribute to the model’s predictivity were excluded from the final model. The goodness of fit and predictive ability of the model were examined using the Hosmer-Lemeshow test and the receiver operating characteristics (ROC) curve, respectively.
Data analysis was performed using IBM Statistical Package for the Social Sciences statistics software, version 23 (IBM Corporation) and Excel, version 14.0 (Microsoft Corporation).
Results
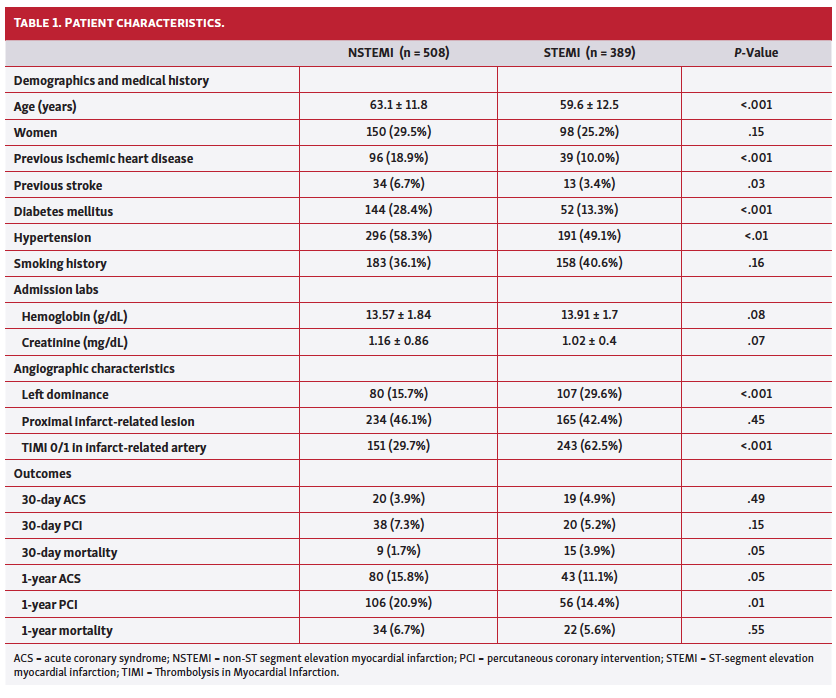
During the study period, a total of 897 patients fulfilled all the inclusion criteria and none of the exclusion criteria at both centers. The mean age of the study group was 61.8 years, with male predominance (Table 1). Out of the entire study population, 508 patients (56.6%) presented with NSTEMI and 389 (43.4%) presented with STEMI. One-year follow-up was completed in 811 patients (90.5%); no patient was lost to follow-up, but 86 patients underwent the index PCI <1 year before data analysis and were therefore not included in the 1-year analysis.
STEMI patients were younger and had less co-morbidity than NSTEMI patients. Similar proportions of proximal infarct-related lesions were found in both groups. More patients with STEMI had left-dominant coronary circulation and TIMI flow of 0/1 in the infarct-related artery. STEMI patients were characterized by higher 30-day mortality (3.9% vs 1.7% in NSTEMI patients; P=.05), with no significant difference at 1-year follow-up in the two groups.
NSTEMI patients were more likely to require recurrent PCI (20.9% vs 14.4% in STEMI patients; P=.01) and hospitalization due to ACS (15.8% vs 11.1% in STEMI patients; P=.05) at 1-year follow-up (Table 1).
No statistically significant difference was noted in the short- and long-term mortality between NSTEMI and STEMI patients with left dominant coronary anatomy (5.0% vs 6.6%, respectively, for 30-day mortality; 10.0% vs 10.2%, respectively, for 1-year mortality) or with totally occluded LCX (2.0% vs 3.7%, respectively, for 30-day mortality; 5.9% vs 4.6%, respectively, for 1-year mortality).
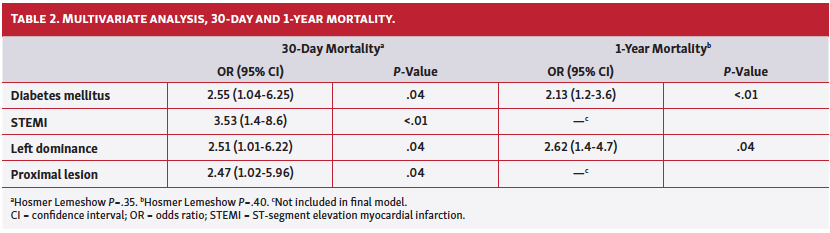
The final multivariate models, which predicted independent risk factors for the 30-day and 1-year mortality, are presented in Table 2. Left-dominant coronary circulation and diabetes mellitus independently predicted both 30-day (odds ratio [OR], 2.51; 95% confidence interval [CI], 1.01-6.22 and OR, 2.55; 95% CI, 1.04-6.25, respectively) and 1-year mortality (OR, 2.62; 95% CI, 1.4-4.7 and OR, 2.13; 95% CI, 1.2-3.6).
Discussion
The current study aimed to investigate the clinical characteristics and outcomes of patients sustaining an LCX-related MI. The rate of mortality among STEMI patients in the current study was 3.9% at 30 days and 5.6% at 1 year, which is comparable to the results of a large registry.8 The mortality rates of NSTEMI patients in the present study (1.7% at 30 days and 6.7% at 1 year) were also similar to previous data.9 When comparing clinical outcomes of the groups, it should be noted that there were differences in the timing of PCI, as patients presenting with STEMI underwent primary PCI immediately, while NSTEMI patients were treated according to the guidelines that advocate early PCI.2,10
The high incidence of TIMI 0/1 flow before PCI in the NSTEMI group (29.7%) underlines the overlap between LCX-related STEMI and NSTEMI. NSTEMI with LCX as the IRA was found to be associated with a higher level of troponin compared with LAD- or RCA-related NSTEMI, and higher incidence of occluded IRA compared with LAD-related NSTEMI.11 Previous data demonstrated a higher risk of MACE and mortality among patients with NSTEMI and a totally occluded IRA.12
Left-dominant coronary circulation (ie, LCX artery supplying the posterior descending artery) is observed in 30% of patients undergoing coronary angiography. It has been linked in the pre-PTCA era to higher adverse events due to insufficient collateral circulation opening during MI. Furthermore, an LCX-dominant circulation is more likely to have an aberrant course, complicating the option for PCI.13 In our cohort, and in line with previous data, left dominance was more prevalent in the STEMI group.14,15
Subgroup analysis of patients with left-dominant coronary circulation and patients with TIMI flow 0, were performed. In both groups, we found no difference in the 30-day and 1-year mortality rates between the STEMI and NSTEMI groups. However, due to the relatively low number of events, these results must be interpreted with caution. The outcomes of patients with left-dominant coronary circulation and LCX as the IRA were evaluated in the past in a small study that included only 9 patients with 44% hospital mortality and 67% cardiogenic shock,16 demonstrating the significantly increased risk in this subgroup of patients.
A previous meta-analysis found left-dominant coronary circulation to be associated with significantly increased risk of in-hospital mortality (OR, 1.54; 95% CI, 1.12-2.11; P<.01), 30-day mortality (OR, 2.16; 95% CI, 1.22-3.84; P<.01), and long-term mortality (OR, 1.83; 95% CI, 1.33-2.50; P<.001).17 It was also found to be an independent risk factor for 30-day mortality when compared with RCA-related STEMI (OR, 2.88; P<.01).18 These results are in line with our results showing left-dominant circulation to be an independent and significant predictor of long- and short-term mortality. To the best of our knowledge, the long-term risk of mortality associated with left-dominant coronary circulation was not previously published. We also found diabetes mellitus to be independently and significantly associated with 30-day and 1-year mortality, similar to previously published data.19 The higher age and prevalence of cardiovascular comorbidities in the NSTEMI group (28.4% vs 13.3% in the STEMI group; P<.001) may explain the higher prevalence of 1-year recurrent PCI and readmissions with ACS in the NSTEMI group.
Study limitations. As a retrospective study, the current study was based on existing databases with their inherent limitations. The angiographic characteristics relied on the PCI report formed at the time of the procedure. As echocardiographic data are stored in separate databases, it was not feasible for extraction and analysis in our study. High-sensitive troponin assays were introduced in both centers during the study period. Therefore, there is no consistency in the reference value of troponin during the entire study period and it was therefore not included in the analysis. The door-to-balloon time intervals were recorded only for STEMI patients; therefore, they were not included in the analysis.
Nonetheless, the present registry included all consecutive patients admitted for LCX-related MI, so we have no reason to believe that the retrospective nature of our cohort could have made an impact on the difference between the study groups. Further research is needed to fully understand the pathophysiology underlying the current findings.
Conclusion
Patients sustaining NSTEMI or STEMI related to LCX occlusion or stenosis have similar 1-year mortality rates. Left-dominant circulation was associated with higher short- and long-term mortality. These results suggest a substantial population of NSTEMI patients should be treated as promptly and aggressively as STEMI patients.
*Joint first authors.
From the 1Department of Cardiology, Hillel Yaffe Medical Center, Hadera, Israel; 2Department of Cardiology, Rambam Health Care Campus, Haifa, Israel; and 3Rappaport, Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Final version accepted June 20, 2020.
Address for correspondence: Ofer Kobo, MD, Department of Cardiology, Hillel Yaffe Medical Center, Hadera, Israel. Email: Ofermkobo@gmail.com
- Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119-177.
- Roffi M, Patrono C, Collet JP, et al. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC), Eur Heart J. 2016;37:267-315.
- Stribling WK, Kontos MC, Abbate A, et al. Left circumflex occlusion in acute myocardial infarction (from the National Cardiovascular Data Registry). Am J Cardiol. 2011;108:959-963.
- From AM, Best PJ, Lennon RJ, Rihal CS, Prasad A. Acute myocardial infarction due to left circumflex artery occlusion and significance of ST-segment elevation. Am J Cardiol. 2010;106:1081-1085.
- Krishnaswamy A, Lincoff AM, Menon V. Magnitude and consequences of missing the acute infarct-related circumflex artery. Am Heart J. 2009;158:706-712.
- Vives-Borrás M, Moustafa AH, Álvarez-García J, et al. Clinical and prognostic value of the electrocardiogram in patients with acute occlusion of the left circumflex coronary artery. Am J Cardiol. 2017;120:1487-1494.
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction. Eur Heart J. 2018;138:1-33.
- Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016;37:3232-3245.
- Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345:494-502.
- Wong CK, White HD. Patients with circumflex occlusions miss out on reperfusion: how to recognize and manage them. Curr Opin Cardiol. 2012;27:327-330.
- Halim SA, Clare RM, Newby LK, et al. Frequency, clinical and angiographic characteristics, and outcomes of high-risk non-ST-segment elevation acute coronary syndromes patients with left circumflex culprit lesions. Int J Cardiol. 2016;203:708-713.
- Khan AR, Golwala H, Tripathi A, Bin Abdulhak AA, Bavishi C. Impact of total occlusion of culprit artery in acute non-ST elevation myocardial infarction: a systematic review and meta-analysis. Eur Heart J. 2017;38:3082-3089.
- Allwork SP. The applied anatomy of the arterial blood supply to the heart in man. J Anat. 1987;153:1-16.
- Waziri H, Jørgensen E, Kelbæk H, et al. Acute myocardial infarction and lesion location in the left circumflex artery: importance of coronary artery dominance. EuroIntervention. 2016;12:441-448.
- Chua SK, Shyu KG, Cheng JJ, et al. Significance of left circumflex artery-related acute myocardial infarction without ST-T changes. Am J Emerg Med. 2010;28:83-88.
- Ilia R, Cafri C, Weinstein JM. Acute myocardial infarction due to occlusion of the dominant left circumflex artery proximally. Am J Cardiol. 2003;92:54-55.
- Khan MS, Usman MS, Akhtar T, et al. Meta-analysis evaluating the effect of left coronary dominance on outcomes after percutaneous coronary intervention. Am J Cardiol. 2018;122:2026-2034.
- Chen YL, Hang CL, Fang HY. Comparison of prognostic outcome between left circumflex artery-related and right coronary artery-related acute inferior wall myocardial infarction undergoing primary percutaneous coronary intervention. Clin Cardiol. 2011;34:249-253.
- Strain WD, Paldánius PM. Diabetes, cardiovascular disease and the microcirculation. Cardiovasc Diabetol. 2018;17:57.










