Pulmonary Arteriography in Pulmonary Vein Stenosis
Key words: angiographic CT, digital subtraction dynamic pulmonary angiography, pulmonary vein imaging
A 43-year-old woman underwent radiofrequency pulmonary vein ablation on November 2018 for symptomatic paroxysmal atrial fibrillation. Three months later, she developed worsening dyspnea and exercise intolerance.
Echocardiography identified right ventricular involvement with dyssynchronous movement of the septum and a high probability of pulmonary hypertension. Systolic pulmonary artery pressure (sPAP) was 58 mm Hg and tricuspid regurgitation reached a peak velocity of 3.6 m/s.
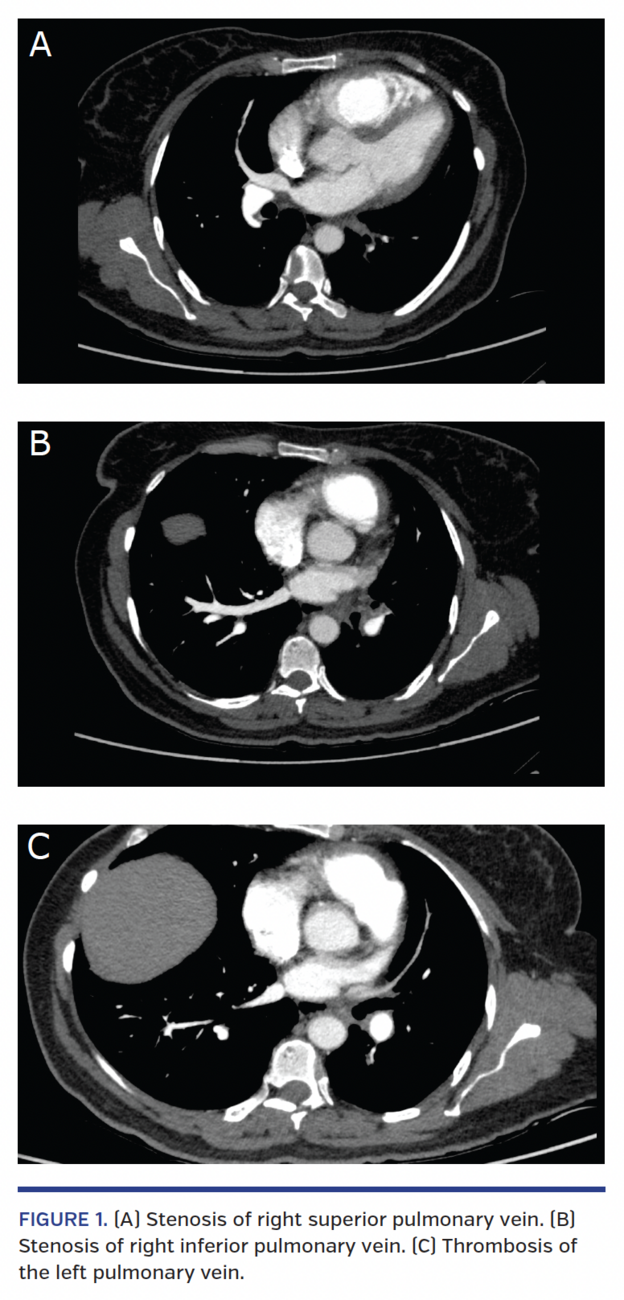
Angiographic computed tomography was performed (Figure 1), revealing severe stenosis of the four pulmonary veins, right ventricular dilation and suggesting total thrombosis of the left superior (LSPV) and left inferior (LIPV) pulmonary veins.
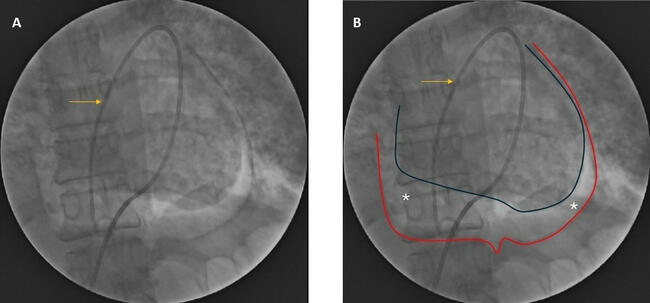
Digital subtraction dynamic pulmonary angiography showed a marked delay in the pulmonary capillary filling time, and in the left inferior pulmonary lobe there was no capillary filling with the contrast medium and an absence of venous return to the left atrium. The LSPV was clearly seen in the final phase of the angiography, ruling out thrombosis. The right superior (RSPV) and right inferior (RIPV) pulmonary veins had severe stenosis at the venoatrial junction with an abnormally small left atrium, and sPAP was 94 mm Hg (Video 1).
Balloon angioplasty was performed in the RSPV, RIPV, and LSPV with progressive balloon dilation, with a maximum diameter of 12 mm, 9 mm, and 10 mm, respectively. The LIPV was not intervened due to a high risk of embolism. After successful balloon angioplasty of all three pulmonary veins, the sPAP went from 94 mm Hg to 60 mm Hg. There were no complications and the patient was discharged 2 days later without dyspnea and with a normal functional status.
From the CES Cardiología, Clínica CES, CES University, Medellin, Colombia.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted October 2, 2019.
Address for correspondence: Laura Duque González, MD, Cl. 34 #43-66, San Diego Mall, North Tower, 11th floor, Medellin, Antioquia, Colombia. Email: duqueglaura@gmail.com