

Radiation Exposure and Contrast Agent Reduction During Transcatheter Aortic Valve Implantation: An Ongoing Experience
Abstract: Objectives. To determine the patient radiation exposure and contrast agent variation during transcatheter aortic valve implantation (TAVI) procedures resulting from technological improvements. Methods. TAVI procedures from January 2008 to July 2015 were analyzed in three different time periods: 1st period, when the angiography was equipped with an image intensifier technology; 2nd period, starting with the installation of a new angiography system with flat-panel detector (FPD) technology; and 3rd period, starting with the systematic use of preprocedural multidetector computed tomography (MDCT) to individualize optimal fluoroscopic projections for the aortic prosthesis implantation. Results. Significant differences were found in contrast volume (198 ± 99 mL vs 139 ± 74 mL; P<.001), kerma area product (211 ± 135 Gy•cm2 vs 147 ± 120 Gy•cm2; P<.001) and effective dose (42 ± 27 mSv vs 29 ± 24 mSv; P<.001) between the 1st and 2nd periods, respectively. The reduction continued between the 2nd and 3rd periods for contrast volume (139 ± 74 mL vs 110 ± 61 mL; P<.001), kerma area product (147 ± 120 Gy•cm2 vs 111 ± 69 Gy•cm2, P<.001), and effective dose (29 ± 24 mSv vs 22 ± 11 mSv; P<.001), respectively. Conclusions. The present study suggests that the appropriate use of FPD technology and preprocedural MDCT to individualize fluoroscopic implant projections for TAVI temporally reduced the amount of radiation and contrast agent administered over time.
J INVASIVE CARDIOL 2016;28(11):459-465
Key words: transcatheter aortic valve implantation, radiation, contrast media, cardiac-gated imaging techniques
Transcatheter aortic valve implantation (TAVI) appears to be a suitable alternative treatment for patients with severe aortic stenosis who are considered at high or excessive risk for conventional surgical aortic valve replacement. Multiple registries and randomized clinical trials have demonstrated the feasibility and efficacy of TAVI.1-5 This procedure involves the use of radiation that has potential deterministic and stochastic adverse effects for both patients and operators. Recently, data regarding single-center experiences of radiation exposure during TAVI have been reported.1-8 At San Raffaele Hospital in Milan, Italy, TAVI was performed for the first time in 2004.6 Thus far, more than 1000 patients have been treated with TAVI using different valve types and procedural access sites.7-9 In this article, we describe the evolution of radiation exposure resulting from the improvement of catheterization laboratory technology, operator experience, and the introduction of the new generation of valves.
Methods
Study population. Data presented in this single-center study were collected between January 2008 and July 2015 at the Interventional Cardiology Unit of the San Raffaele Hospital in Milan, Italy. A total of 682 consecutive patients treated with TAVI were included. Patients treated via trans- apical, transaortic, or transaxillary approach were excluded. Furthermore, the first 37 consecutive TAVI patients (5.4%), from January 2008 through December 2008) were excluded from the three time period analyses in order to reduce the bias related to the operator learning curve. All patients signed an informed consent for the procedure and for the anonymous use of their data for retrospective evaluation, which has been approved by our local ethics committee.
Procedural time periods. Three different time periods were considered: 1st period, from January 2009 through January 2011, when the angiography was still equipped with image intensifier (II) technology and the experience of the operators was no longer at an early stage; 2nd period, from February 2011 through April 2013, and starting with the installation of a new angiography system with flat-panel detector (FPD) technology; and 3rd period, from May 2013 through July 2015, with the systematic use of preprocedural multidetector computed tomography imaging (MDCT) to individualize optimal fluoroscopic projections that permit orthogonal visualization of the aortic valve plane.
Equipment. All cases were carried out in the same catheterization laboratory using a Philips Integris 5000 single-plane C-arm with II technology (Philips Volcano) until the 2nd period and Philips Allura Xper FD 10 single-plane C-arm with FPD technology (Philips Volcano) for the 2nd and 3rd periods. Data on radiation exposure were collected from an integrated dosimeter on the x-ray tube collimator.
X-ray imaging modes. Fluoroscopy, cine angiography, and digital subtraction x-ray imaging acquisitions were used during TAVI procedures. Standard settings for image acquisition included 15 frames/s for fluoroscopy, 15 frames/s for fluoroscopy/cine acquisition, and 3 frames/s for digital subtraction utilized only in order to acquire images of femoral arteries. Only the FPD technology, utilized starting from the 2nd period, has the capacity to store fluoroscopic run images for documentation like cine run images.
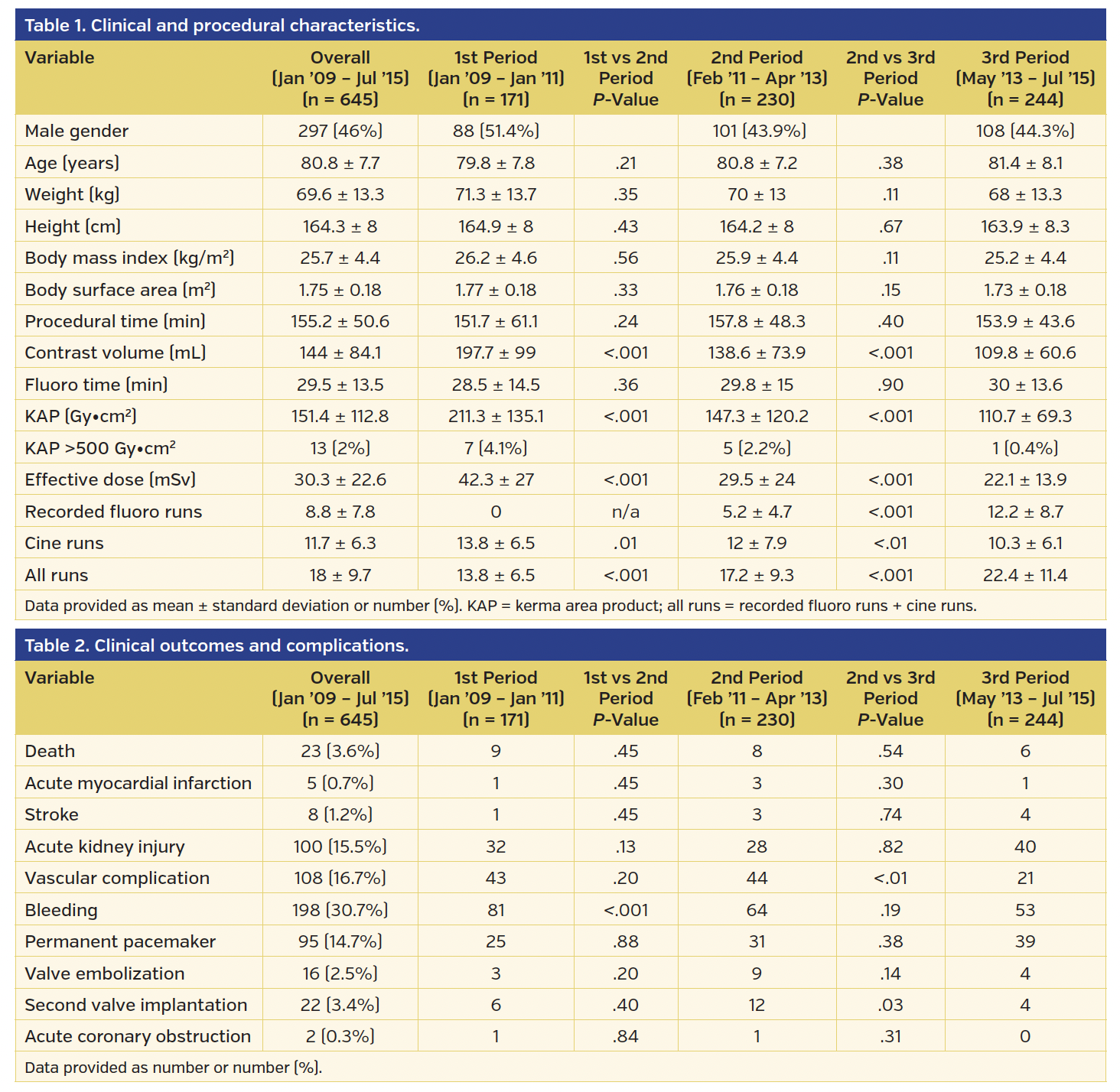
Radiation dose measurements. All interventional fluoroscopes were equipped with integrated dosimetric instrumentation. The performance of this instrumentation was verified semiannually as part of the hospital’s QA program by the internal Medical Physics Department. Radiation dose during the procedure was recorded using the air kinetic energy released per unit mass (kerma) area product (PKA or KAP), also known as the dose area product (DAP). The cumulative KAP measured in Gy•cm2 is the product of absorbed dose to air and beam cross-sectional area and is a quantity independent of the distance to the x-ray tube focal spot, which can be used in radiological exams to assess the effective dose in patients.10 The KAP meter (or DAP meter) technique is the most reliable measure for dynamic examinations such as fluoroscopy, in which the projections, direction, and parameters are continually varying.11 Data on patient physical characteristics, fluoroscopy time, procedure time, contrast volume, number of runs acquired divided by recorded fluoro runs, cine runs, and all runs (recorded fluoro runs + cine runs) were reported (Table 1) and data on main clinical outcomes and complications were also reported in accordance with the Valve Academic Research Consortium-2 (VARC-2) definitions12 (Table 2). According to the recent International Commission on Radiological Protection (ICRP) 120 recommendation,13 in cases where the procedure exceeds one of the trigger-level points for a potential skin injury (peak skin dose of 3 Gy, KAP of 500 Gy•cm2, and air kerma at the patient entrance reference point of 5 Gy), clinical follow-up at 4 weeks was performed for early detection and management of these injures.
In order to compare TAVI procedures with other radiological procedures, we estimated approximately the effective dose (ED) using the following formula: ED (mSv) = KAP (Gy•cm2) x 0.2 (mSv/Gy•cm2).14
TAVI procedures. Patient and procedural planning, including selection of access route, was carried out at a dedicated multidisciplinary heart team meeting. The considered TAVI procedures were performed using a percutaneous transfemoral (TF) approach under local anesthesia, reflecting our default approach. For percutaneous TF-TAVI procedures, vascular access puncture for the large TAVI sheath was obtained using fluoroscopic guidance (as previously reported).15,16 Femoral access closure was performed using the Prostar XL or Perclose Proglide closure devices (Abbott Vascular). Different valve types were utilized: Edwards Sapien, Sapien XT, and Sapien 3 (Edwards Lifesciences), Medtronic CoreValve, CoreValve Evolut R (Medtronic, Inc), Direct Flow Medical Transcatheter Aortic Valve System (Direct Flow Medical, Inc), Lotus valve (Boston Scientific), and Portico valve (St. Jude Medical).
Evaluation of the aortic valve plane. MDCT imaging has emerged as an invaluable tool in the evaluation of patients for TAVI1,4 by providing accurate and highly reproducible measurements of the aortic valve and adjacent structures17-19 and the three-dimensional (3D) volume may be utilized to determine specific fluoroscopic implant projections.19,20 The CT analysis involved performing one tilt of the anteroposterior axis and one tilt of the lateral axis in the 3D-CT reconstruction in order to bring the originally axial view plane into position and double-oblique view orientation of the valve plane. These two tilt angles are selected carefully to bring the lowest hinge point of each of the three coronary cusps into the valve plane view. Once determined, the valve plane orientation is confirmed by scrolling distally to verify that all three leaflets appear in view immediately and simultaneously. The two tilt angles needed to rotate the axial plane into the valve plane are used to recreate the valve plane orientation geometrically and calculate the c-arm positions that will be in-line with it.
Statistical analysis. Continuous variables were compared among groups using analysis of variance with Fisher’s least-significant difference post hoc tests for correction for multiple comparisons and reported as mean ± standard deviation, based on the normality (Kolmogorov-Smirnov goodness of fit test) of the data. Categorical data are presented as counts or percentages; they were compared with the Pearson’s chi-square test. Two-side P-values <.05 were considered statistically significant.
Locally weighted scatterplot smoothing (Lowess), a non-parametric regression method, was used to demonstrate temporal trends on scatterplots with procedure date order as the variable on the horizontal axis. All data were analyzed with IBM SPSS Statistics for Windows, version 21.0 (IBM Corporation).
Results
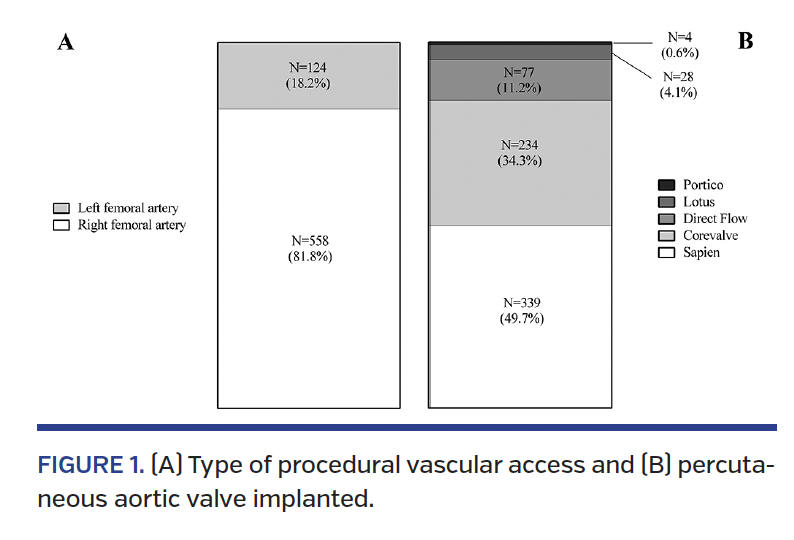
Baseline clinical, procedural, and dosimetric characteristics stratified according to the time periods are presented in Table 1 and Figure 1. The most utilized procedural access route was the right common femoral artery (Figure 1A). The percentage of each type of valve implanted is reported in Figure 1B.
Considering the three time periods, no significant differences were found regarding the main clinical characteristics of patients. During TAVI, the mean radiation dose (KAP) was 151 ± 113 Gy•cm2, mean fluoroscopic time was 29 ± 13 minutes, and mean contrast volume used was 144 ± 84 mL. The contrast volume, KAP, and ED were significantly reduced across the three times periods (P<.001). In fact, considering the 1st and 2nd periods, where the procedures were performed using II and FPD technologies, respectively, without aortic implant plane CT calculation, we found significant differences in terms of contrast volume (198 ± 99 ml vs 139 ± 74 mL; P<.001), KAP (211 ± 135 Gy•cm2 vs 147 ± 120 Gy•cm2; P<.001), ED (42 ± 27 mSv vs 29 ± 24 mSv; P<.001), cine runs (14 ± 6 vs 12 ± 8; P=.01), and number of all runs acquired (14 ± 6 vs 17 ± 9; P<.001). Regarding clinical outcomes, no significant differences were found excluding for major vascular bleedings, which were significantly lower in the 2nd period (81 vs 64; P<.001) (Table 2).
Considering the 2nd and 3rd periods, in which FPD technology was the common denominator and systematic MDCT aortic implant plane evaluation was utilized only in the 3rd period, the mean of contrast volume, KAP, ED, and number of cine runs continued to decrease significantly, whereas the number of recorded fluoro runs and all runs acquired increase significantly (Table 1). Furthermore, we found fewer vascular complications (44 vs 21; P<.01) and need for second valve implantation (12 vs 4; P=.03) in the 3rd period (Table 2).
Considering the three different periods, we found no significant differences in mean fluoroscopy time (28 minutes vs 30 minutes vs 30 minutes, respectively).
The number of cases where the KAP trigger-level value of 500 Gy•cm2 was exceeded, as indicated by the ICRP13 for a potential skin injury, was 7 for the 1st period, 5 for the 2nd period, and 1 for the 3rd period. No case of skin injury was reported in these patients at the 4-week follow-up.
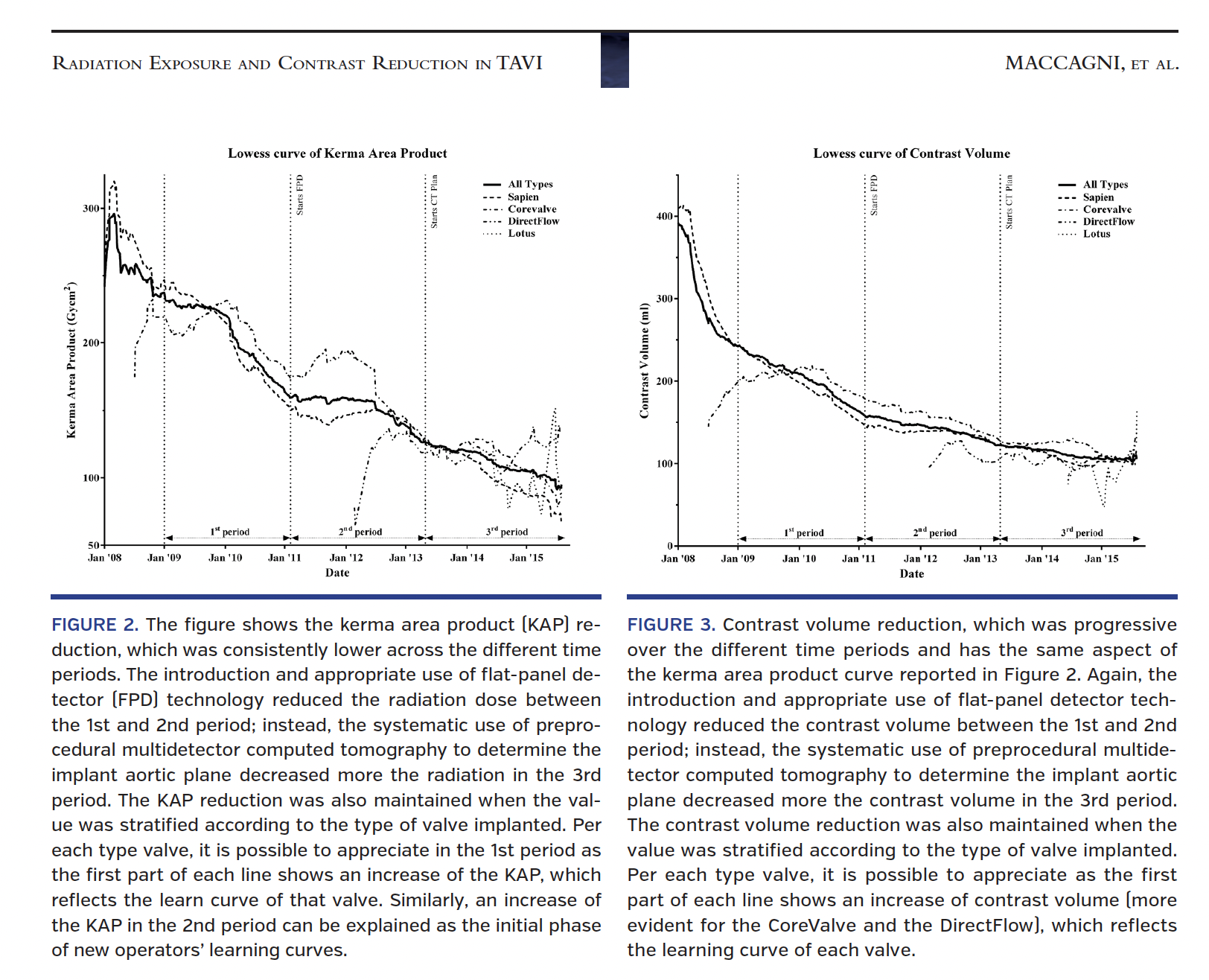
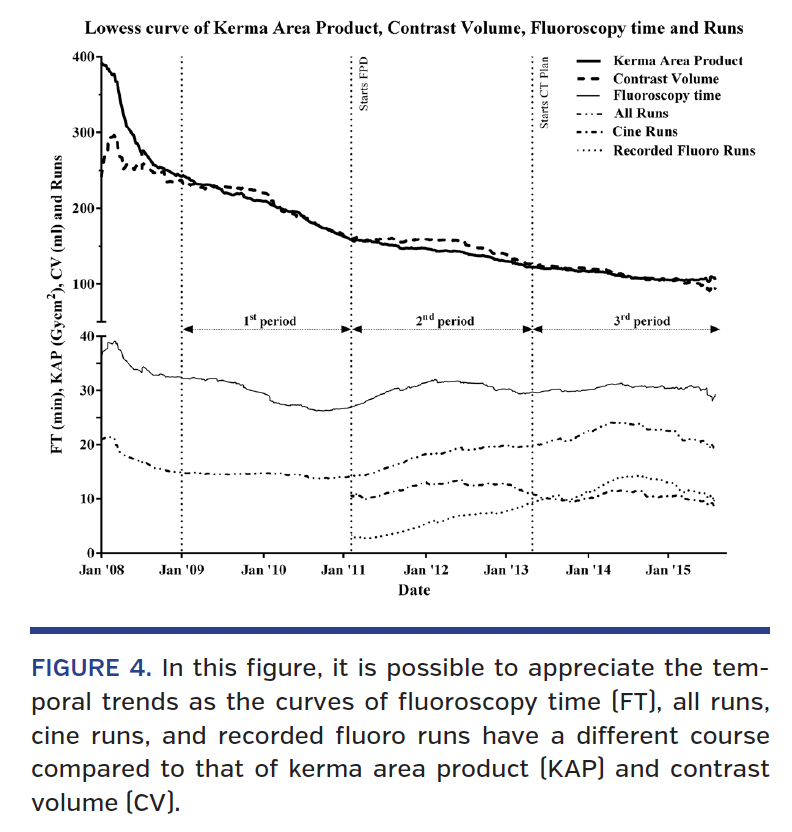
The continued trend toward decreases in dosimetric and procedural parameters are shown in Figures 2-4. Figures 2 and 3 reported the temporal trend for overall KAP and contrast volume, respectively, and are also stratified for the valve type implanted. The temporal trends for overall fluoroscopy time, KAP, contrast volume, and number of runs acquired divided by cine, recorded fluoro, and all runs are reported in Figure 4.
Discussion
This study represents the largest single-center cohort of TAVI patients evaluated for radiation exposure during the procedure. The principal findings are: (1) the appropriate use of FPD technology reduced the radiation and contrast volume utilized for TAVI procedures between the 1st and 2nd period; (2) the systematic use of preprocedural MDCT to determine the implant aortic plane decreased even further the radiation and contrast volume in the 3rd period; (3) the fluoroscopy time was not associated with an increase in patients’ radiation exposure levels.
Before our study, Signorotto et al reported radiation exposure of 76 TAVI procedures performed at our center between 2007 and 2008.21 They observed a mean KAP of 259 Gy•cm2, which clearly refers to the initial phase of the operators’ learning curves, when FPD technology was not present and delivery valve technology was at an early stage. The mean KAP observed in the present study (151 Gy•cm2) is much lower than that reported by Signorotto et al (2013-2015), when the imaging tools and the operators skills were markedly improved, and was also considerably less in the 3rd period (111 Gy•cm2). It is important to note that the introduction of FPD technology does not produce an automatic savings in patient dose if operators don’t apply the practical principles of radiation protection and don’t take full advantage of the possibilities offered by this digital technology.22-24 For example, in our procedures, one of the useful tools offered by the FPD technology utilized was the possibility to acquire fluoroscopy images instead of cine runs to reduce radiation exposure to both patients and operators. A recorded fluoro run instead of a cine run results in a decrease in the patient’s radiation dose up to 12 times, for an equal number of frames acquired.25
Mean KAP observed in the 3rd period for the TF approach was lower compared with values reported by Daneault et al (236 Gy•cm2)26 and Steinvil et al (248 Gy•cm2)27 and was similar to the value reported by Sharma et al (102 Gy•cm2).28 Possible explanations for such differences can be found in the lower mean value of body mass index (BMI) discovered in our patients (25.2 kg/m2 vs 25.8 kg/m2 vs 27 kg/m2 for our study vs Daneault vs Steinvil, respectively) and in the differences in the radiological parameters and machines utilized. As previously reported, higher values of weight and BMI are associated with greater amounts of radiation during TAVI26 and other radiological procedures.29-31 Patients with high BMI require an increase of the radiological parameters in the x-ray tube to generate sufficiently visible images.
Once again, it should be noted that fluoroscopy time can be used as a surrogate for procedural complexity, but should not be used as a patient radiation exposure parameter32 because its doesn’t include the exposure time from the other radiological modality available like cine runs or digital subtraction acquisitions. In fact, we found no significant differences in mean fluoroscopy time in the three different periods (28 minutes vs 30 minutes vs 30 minutes, respectively); instead, a significant difference was reported in terms of mean KAP between the 1st period and the other 2 periods (211 Gy•cm2 vs 147 Gy•cm2 vs 111 Gy•cm2, respectively; P<.001), which is considered one of the main descriptors of patient dose, together with the air kerma at the patient entrance reference point and the peak skin dose.33
Particular attention should be placed to trigger-level points for a potential skin injury, as indicated in the recent ICRP 120 recommendation:13 peak skin dose of 3 Gy, KAP of 500 Gy•cm2, and air kerma at the patient entrance reference point of 5 Gy. When the patient’s radiation dose during the procedure exceeds one of these trigger levels, clinical follow-up should be performed for early detection and management of skin injuries. Patients who have received a substantial radiation dose should have follow-up 2-4 weeks after the procedure for detection of potential radiation injuries. In the present experience, we noted only 1 case (0.4%) of radiation exposure exceeding the trigger level for skin injury in the 3rd period (2013-2015) in a severely obese patient (BMI, 43.5 kg/m2) as compared with the 1st period (7 cases; 4.1%) and none of these had skin injures at 4-week follow-up exam. This could be a consequence of the combination of a better angiography system, operator experience, and preprocedural planning.
We found an estimated mean ED of 22 mSv in the 3rd period; this value can be used to compare TAVI procedures with other interventional cardiology procedures. The estimated ED value of TAVI procedures was not different when compared with other PCI procedures (15 mSv).34
All interventional procedures have evidence of a learning curve.35-37 TAVI procedures are also subject to this rule, especially when operator experience is at an early stage.38 In order to reduce the bias effect related to the operator learning curve, we decided to exclude 37 TAVI procedures performed between January and December 2008.
Similar to a study by Alli et al,38 several aspects impacted the learning curve: the use of preprocedural MDCT to determine valve measures, the best angiographic projection for valve deployment, and the best access site have decreased the use of several angiographic cine runs, decreasing contrast volume used and radiation dose. In addition, the appropriate analysis of MDCT contributed to a lower rate of vascular complications and to more accurate valve sizing. Finally, the use of intraprocedural echocardiography in order to immediately evaluate the severity of periprosthetic and internal valve regurgitation has reduced the necessity for angiograms post valve implantation.
Study limitations. This is a retrospective single-center observational analysis and is subject to many limitations of such analyses. First, the sample size is relatively small, which may be a limitation in the interpretation of the data. Second, the learning curve for each of the operators resulted in a greater efficiency and “comfort” of the operators with the procedure. This is a variable that cannot be easily measured and undoubtedly constitutes a lack of evaluation, and therefore a methodological limit. However, there were no major changes in the procedure technique during the three time periods, which can explain the significant decrease in radiation exposure. Indeed, standard techniques for percutaneous vascular access and the diminution of vascular complications, such as angiographically guided arterial puncture and crossover wire protection, are still performed. Furthermore, the fluoroscopy time, which may be considered a surrogate of procedural length, did not change during the three periods. Third, the impact of new-generation devices on simplifying the procedure is difficult to evaluate, especially since some of these devices allow for repositioning and retrievability, thus impacting radiation exposure and contrast dose.
Conclusion
The present study suggests that the appropriate use of FPD technology and preprocedural gated cardiac MDCT to individualize fluoroscopic implant projections for TAVI temporally reduces the amount of radiation and contrast agent administered over time. Particular attention should be given to skin injury trigger levels, which could be higher when operator experience is in the early stage.
References
1. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597-1607.
2. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198.
3. Holmes Jr. DR, Mack MJ, Kaul S, et al. 2012 ACCF/AATS/SCAI/STS expert consensus document on transcatheter aortic valve replacement. J Am Coll Cardiol. 2012;59:1200-1254.
4. Makkar RR, Fontana GP, Jilaihawi H, et al. Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N Engl J Med. 2012;366:1696-1704.
5. Adams DH, Popma JJ, Reardon MJ. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;371:967-968.
6. Colombo A, Bianconi L, Montorfano M, et al. [Severe aortic stenosis successfully treated with percutaneous aortic valve implantation]. Ital Heart J Suppl. 2005;6:291-296.
7. Godino C, Maisano F, Montorfano M, et al. Outcomes after transcatheter aortic valve implantation with both Edwards-SAPIEN and CoreValve devices in a single center: the Milan experience. JACC Cardiovasc Interv. 2010;3:1110-1121.
8. Buchanan GL, Chieffo A, Montorfano M, et al. The role of sex on VARC outcomes following transcatheter aortic valve implantation with both Edwards SAPIEN and Medtronic CoreValve ReValving System(R) devices: the Milan registry. EuroIntervention. 2011;7:556-563.
9. Taramasso M, Latib A, Cioni M, et al. Quality of life improvement is maintained up to two years after transcatheter aortic valve implantation in high-risk surgical candidates. EuroIntervention. 2012;8:429-436.
10. Godino C, Maccagni D, Pavon AG, et al. Estimating incidence of organ cancer related to PCI radiation exposure in patients treated for acute and chronic total occlusions. J Invasive Cardiol. 2013;25:441-445.
11. Betsou S, Efstathopoulos EP, Katritsis D, Faulkner K, Panayiotakis G. Patient radiation doses during cardiac catheterization procedures. Br J Radiol. 1998;71:634-639.
12. Kappetein AP, Head SJ, Genereux P, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol. 2012;33:1438-1454.
13. Cousins C, Miller DL, Bernardi G, et al. ICRP Publication 120. Radiological protection in cardiology. Ann ICRP. 2013;42:1-125.
14. Rehani MM, Ciraj-Bjelac O, Vañó E, et al. ICRP Publication 117. Radiological protection in fluoroscopically guided procedures performed outside the imaging department. Ann ICRP. 2010;40:1-102.
15. Sharp AS, Michev I, Maisano F, et al. A new technique for vascular access management in transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2010;75:784-793.
16. Buchanan GL, Chieffo A, Montorfano M, et al. A “modified crossover technique” for vascular access management in high-risk patients undergoing transfemoral transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2013;81:579-583.
17. Gurvitch R, Webb JG, Yuan R, et al. Aortic annulus diameter determination by multidetector computed tomography: reproducibility, applicability, and implications for transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2011;4:1235-1245.
18. Jilaihawi H, Kashif M, Fontana G, et al. Cross-sectional computed tomographic assessment improves accuracy of aortic annular sizing for transcatheter aortic valve replacement and reduces the incidence of paravalvular aortic regurgitation. J Am Coll Cardiol. 2012;59:1275-1286.
19. Gurvitch R, Wood DA, Leipsic J, et al. Multislice computed tomography for prediction of optimal angiographic deployment projections during transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2010;3:1157-1165.
20. Binder RK, Leipsic J, Wood D, et al. Prediction of optimal deployment projection for transcatheter aortic valve replacement: angiographic 3-dimensional reconstruction of the aortic root versus multidetector computed tomography. Circ Cardiovasc Interv. 2012;5:247-252.
21. Signorotto P, del Vecchio A, Montorfano M, et al. Dosimetric data and radiation risk analysis for new procedures in interventional cardiology. Radiat Prot Dosimetry. 2010;142:201-208.
22. Chida K, Inaba Y, Saito H, et al. Radiation dose of interventional radiology system using a flat-panel detector. Am J Roentgenol. 2009;193:1680-1685.
23. Bogaert E, Bacher K, Lapere R, Thierens H. Does digital flat detector technology tip the scale towards better image quality or reduced patient dose in interventional cardiology? Eur J Radiol. 2009;72:348-353.
24. Davies AG, Cowen AR, Kengyelics SM, Moore J, Sivananthan MU. Do flat detector cardiac x-ray systems convey advantages over image-intensifier-based systems? Study comparing x-ray dose and image quality. Eur Radiol. 2007;17:1787-1794.
25. Kuon E. Radiation exposure in invasive cardiology. Heart. 2008;94:667-674.
26. Daneault B, Balter S, Kodali SK, et al. Patient radiation exposure during transcatheter aortic valve replacement procedures. EuroIntervention. 2012;8:679-684.
27. Steinvil A, Aviram G, Konigstein M, et al. Radiation dose of patients undergoing transcatheter aortic valve implantation: a comparison between Edwards Sapien XT and Medtronic CoreValve aortic valve prostheses. Catheter Cardiovasc Interv. 2013;82:E578-E582.
28. Sharma D, Ramsewak A, O’Conaire S, Manoharan G, Spence MS. Reducing radiation exposure during transcatheter aortic valve implantation (TAVI). Catheter Cardiovasc Interv. 2015;85:1256-1261.
29. Kim KP, Miller DL, Berrington de Gonzalez A, et al. Occupational radiation doses to operators performing fluoroscopically-guided procedures. Heal Phys. 2012;103:80-99.
30. Detorie N, Mahesh M, Schueler BA. Reducing occupational exposure from fluoroscopy. J Am Coll Radiol. 2007;4:335-337.
31. Nickoloff EL, Lu ZF, Dutta A, So J, Balter S, Moses J. Influence of flat-panel fluoroscopic equipment variables on cardiac radiation doses. Cardiovasc Interv Radiol. 2007;30:169-176.
32. Padovani R, Bernardi G, Malisan MR, Vano E, Morocutti G, Fioretti PM. Patient dose related to the complexity of interventional cardiology procedures. Radiat Prot Dosimetry. 2001;94:189-192.
33. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann ICRP. 2007;37:1-332.
34. Mettler Jr. FA, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology. 2008;248:254-263.
35. Ahmadi RA, Schillinger M, Haumer M, Willfort A, Minar E. Carotid stenting in a case of combined kinking and stenosis. Cardiovasc Interv Radiol. 2001;24:197-199.
36. Lurz P, Coats L, Khambadkone S, et al. Percutaneous pulmonary valve implantation: impact of evolving technology and learning curve on clinical outcome. Circulation. 2008;117:1964-1972.
37. Gurvitch R, Tay EL, Wijesinghe N, et al. Transcatheter aortic valve implantation: lessons from the learning curve of the first 270 high-risk patients. Catheter Cardiovasc Interv. 2011;78:977-984.
38. Alli OO, Booker JD, Lennon RJ, Greason KL, Rihal CS, Holmes DR Jr. Transcatheter aortic valve implantation: assessing the learning curve. JACC Cardiovasc Interv. 2012;5:72-79.
From the 1Cardio-Thoracic-Vascular Department, San Raffaele Hospital, Milan, Italy; 2AITRI (Italian Association of Interventional Radiographers), Milan, Italy; and 3EMO-GVM Centro Cuore Columbus, Milan, Italy.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Latib is a consultant for Medtronic and Direct Flow Medical. Dr Colombo was a minor shareholder in Direct Flow Medical. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 11, 2016, provisional acceptance given May 18, 2016, final version accepted June 22, 2016.
Address for correspondence: Davide Maccagni, RT, San Raffaele Hospital. Via Olgettina 60, 20132 Milan, Italy. Email: maccagni.davide@gmail.com













