

Rapid Stent Surface Coverage After Endothelial Progenitor Cell Capture (Genous) Stent Implantation: First Optical Coherence Tomography Report
Abstract: A 78-year-old man was referred for anterior wall motion abnormality on echocardiogram. In anticipation of the urgent surgery for stomach cancer, an endothelial progenitor cell Genous capture stent (Orbus Neich Medical Technology) was implanted. After 2 weeks, optical coherence tomography was done to confirm the coverage of stent struts and all struts were fully covered by reendothelialization. The patient could undergo stomach surgery without antiplatelet therapy successfully.
J INVASIVE CARDIOL 2012;24(4):188-189
Key words: antiplatelet therapy, endothelialization, optical coherence tomography
_____________________________________________
Case Report
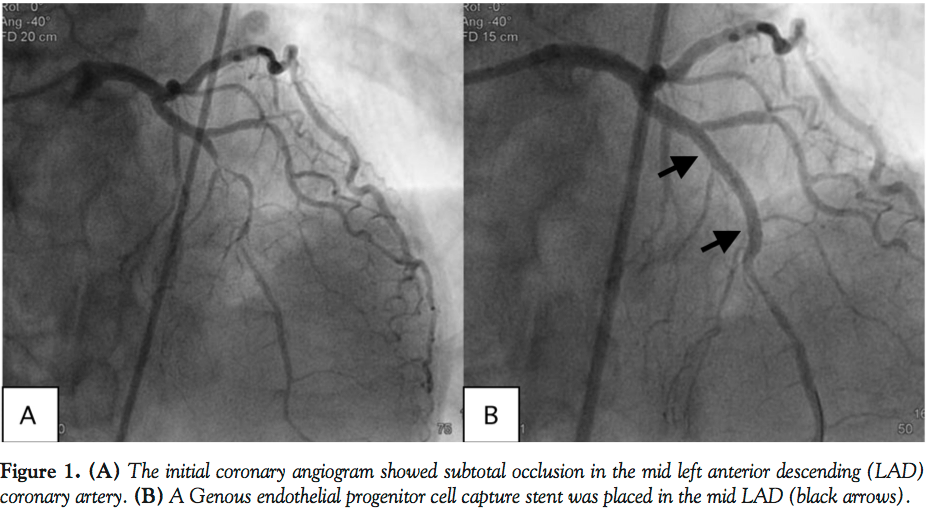 A 78-year-old man was referred for intermittent chest pain during preoperative risk assessment for stomach cancer. Echocardiogram showed anterior wall motion abnormality during chest pain. Coronary angiogram revealed tight stenosis in the mid left anterior descending (LAD) coronary artery (Figure 1A). In anticipation of the urgent surgery and chest pain due to unstable angina, plain old balloon angioplasty (POBA) was applied to the stenotic lesion. However, there was still significant residual stenosis and minor dissection was
A 78-year-old man was referred for intermittent chest pain during preoperative risk assessment for stomach cancer. Echocardiogram showed anterior wall motion abnormality during chest pain. Coronary angiogram revealed tight stenosis in the mid left anterior descending (LAD) coronary artery (Figure 1A). In anticipation of the urgent surgery and chest pain due to unstable angina, plain old balloon angioplasty (POBA) was applied to the stenotic lesion. However, there was still significant residual stenosis and minor dissection was 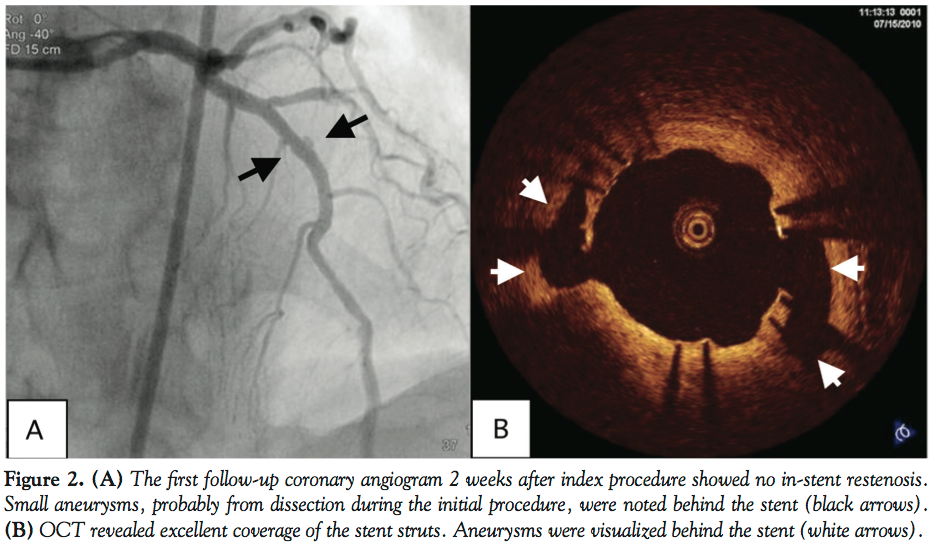 suspected after POBA. It seemed that the deployment of a stent was inevitable. An endothelial progenitor cell (EPC) capture stent (Genous; Orbus Neich Medical Technology) was implanted (Figure 1B) to promote reendothelialization by CD 34 antibodies attached to stent struts. The patient was started on dual antiplatelet therapy after the procedure. Two weeks later, the patient underwent repeat coronary angiography and optical coherence tomography (OCT). There was no in-stent restenosis; however, two newly developed small aneurysms were found behind the stent struts (Figure 2). All stent struts were covered on OCT.
suspected after POBA. It seemed that the deployment of a stent was inevitable. An endothelial progenitor cell (EPC) capture stent (Genous; Orbus Neich Medical Technology) was implanted (Figure 1B) to promote reendothelialization by CD 34 antibodies attached to stent struts. The patient was started on dual antiplatelet therapy after the procedure. Two weeks later, the patient underwent repeat coronary angiography and optical coherence tomography (OCT). There was no in-stent restenosis; however, two newly developed small aneurysms were found behind the stent struts (Figure 2). All stent struts were covered on OCT.
 The patient underwent uneventful stomach surgery without antiplatelet therapy, 2 weeks after OCT. Two weeks later, OCT was repeated to follow the aneurysmal changes behind the stent. The signal-free areas have decreased in size without communication with the lumen.
The patient underwent uneventful stomach surgery without antiplatelet therapy, 2 weeks after OCT. Two weeks later, OCT was repeated to follow the aneurysmal changes behind the stent. The signal-free areas have decreased in size without communication with the lumen.
The first-line therapy for patients with non-deferrable surgery is POBA with dual antiplatelet therapy for 2 weeks or implantation of bare-metal stent with dual  antiplatelet therapy for 1 month. EPC capture stent implantation with shorter antiplatelet therapy may be a good option for patients who need urgent surgery, under confirmation of full reendothelialization by OCT.
antiplatelet therapy for 1 month. EPC capture stent implantation with shorter antiplatelet therapy may be a good option for patients who need urgent surgery, under confirmation of full reendothelialization by OCT.
Acknowledgment. We are grateful to Ik-Kyung Jang from Massachusetts General Hospital of Harvard Medical School for his invaluable support and assistance with this report.
_____________________________________________
From the Department of Cardiology, Kyung-Hee University Hospital at Gangdong, Seoul, Korea.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 5, 2011, provisional acceptance given October 11, 2011, final version accepted October 24, 2011.
Address for correspondence: Professor Jinman Cho, Kyunghee University, Cardiovascular Center, #149 Sangil-Dong Gangdong-Gu, Seoul, 134-727, South Korea. Email: aceri@medimail.co.kr











